Name______Completion Date______
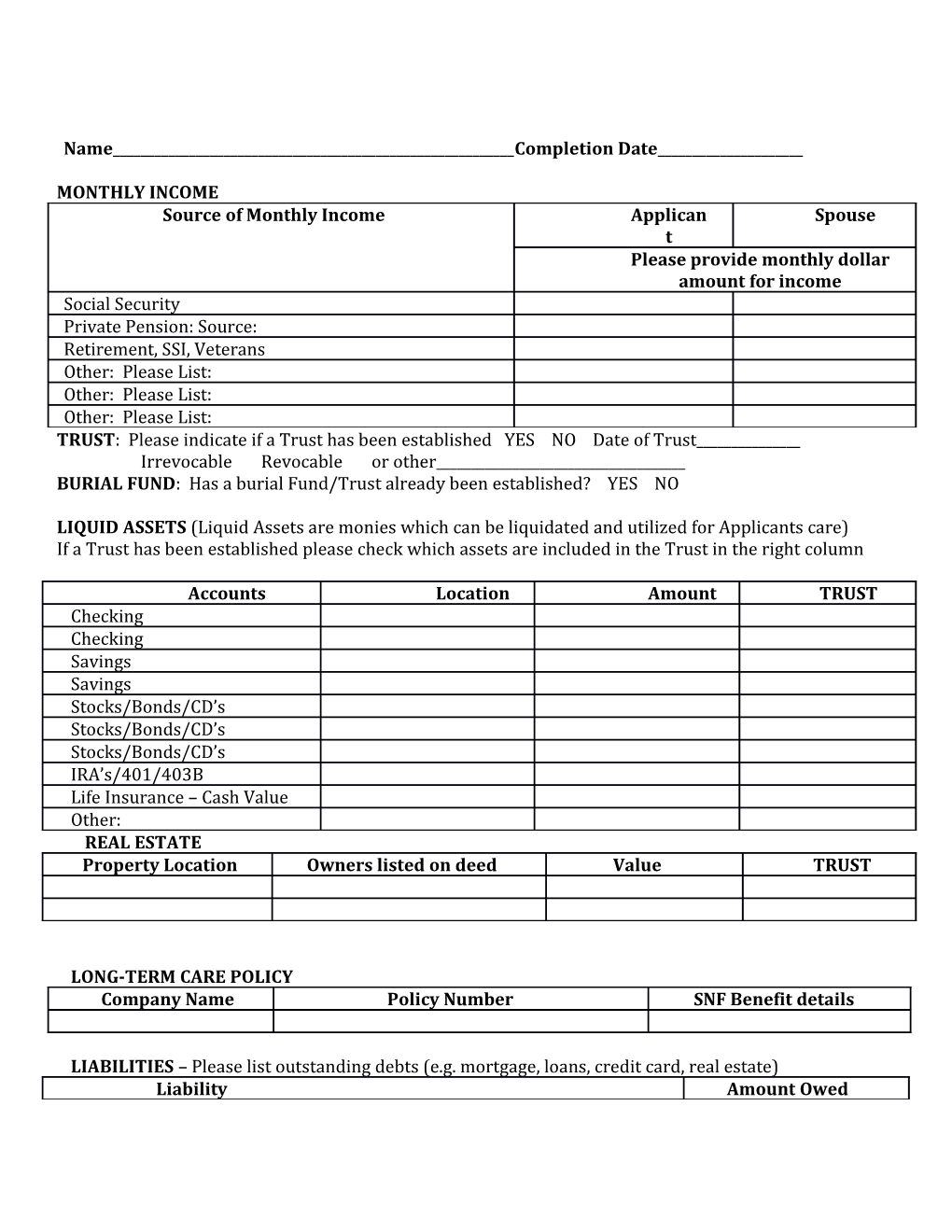
MONTHLY INCOME Source of Monthly Income Applican Spouse t Please provide monthly dollar amount for income Social Security Private Pension: Source: Retirement, SSI, Veterans Other: Please List: Other: Please List: Other: Please List: TRUST: Please indicate if a Trust has been established YES NO Date of Trust______Irrevocable Revocable or other______BURIAL FUND: Has a burial Fund/Trust already been established? YES NO
LIQUID ASSETS (Liquid Assets are monies which can be liquidated and utilized for Applicants care) If a Trust has been established please check which assets are included in the Trust in the right column
Accounts Location Amount TRUST Checking Checking Savings Savings Stocks/Bonds/CD’s Stocks/Bonds/CD’s Stocks/Bonds/CD’s IRA’s/401/403B Life Insurance – Cash Value Other: REAL ESTATE Property Location Owners listed on deed Value TRUST
LONG-TERM CARE POLICY Company Name Policy Number SNF Benefit details
LIABILITIES – Please list outstanding debts (e.g. mortgage, loans, credit card, real estate) Liability Amount Owed ASSET TRANSFER Current look back period when applying for Medicaid is five (5) years. It is important to know that transfers of assets within this look back period could potentially result in a penalty or denial of Medicaid eligibility by the Department of Social Services. Assets can not only be monetary but real estate, land, stocks and investments.
ASSET TRANSFERRED TRANSFERRED TO AMOUNT OF TRANSFER
Has a Medicaid application been submitted on behalf of the applicant? YES NO Date of application submission:______County______Name of Case Worker______Phone______I hereby declare that the statement of assets and monthly income levels are true to the best of my knowledge and belief. Upon completion of this form, I acknowledge that the total of the applicants resources is $______and these assets/monies will be utilized for the services and care provided by the Fairport Baptist Homes.
It is mandated that the Fairport Baptist Homes be notified three (3) months prior to the exhaustion of resources available for the applicants care so that the Medicaid application can be initiated. The Fairport Baptist Homes reserves the right to request additional financial information including, but not limited to, copies of financial statements and/or the most recently completed 1089 form(s).
Please be advised that upon admission to the Fairport Baptist Homes skilled nursing that a security deposit equal to one months’ (30 days) private room rate is required for all private pay Residents.
Print Name______
Signature Power of Attorney/Responsible Party______Date______