PATIENT KNEE BRACE EVALUATION FORM
Patient Name______DOB______Male Female
Physician ______NPI No. ______General Patient Profile
Walks: Independently Uses CaneUses Walker Uses Wheel Chair Weight (lbs.) ______Height______
Dr. Rx Medical Necessity VertaLoc Dynamic Knee Brace VertaLoc Max OA Knee Brace
To facilitate healing following a surgical procedure to the knee or related soft tissues. Date of procedure ______Description:______ To facilitate healing following an injury to the knee or related soft tissues. Description:______ To reduce pain by restricting mobility of the knee.
To otherwise support instability of the knee.
Patient Measurement :
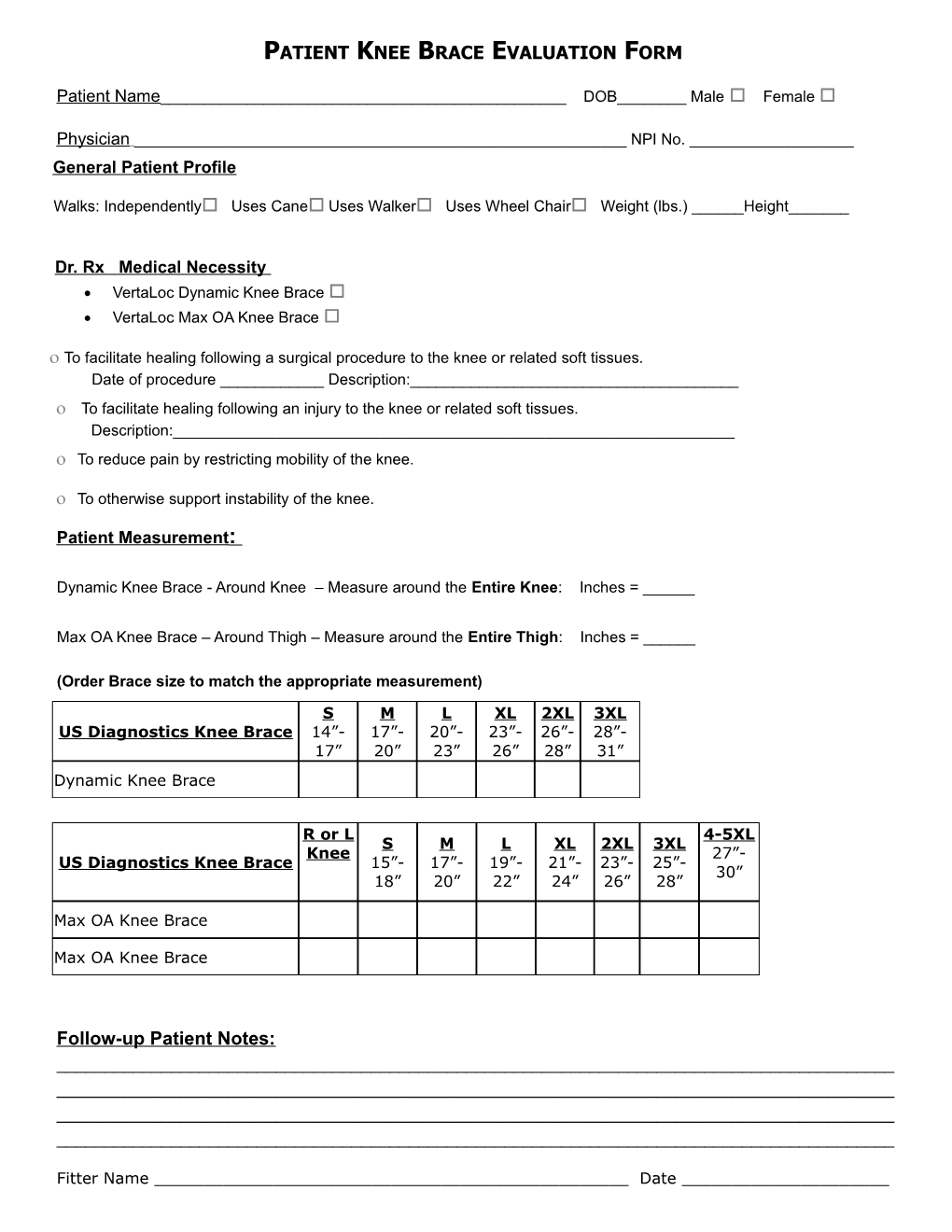
Dynamic Knee Brace - Around Knee – Measure around the Entire Knee: Inches = ______
Max OA Knee Brace – Around Thigh – Measure around the Entire Thigh: Inches = ______
(Order Brace size to match the appropriate measurement)
S M L XL 2XL 3XL US Diagnostics Knee Brace 14”- 17”- 20”- 23”- 26”- 28”- 17” 20” 23” 26” 28” 31” Dynamic Knee Brace
R or L 4-5XL S M L XL 2XL 3XL Knee 27”- US Diagnostics Knee Brace 15”- 17”- 19”- 21”- 23”- 25”- 30” 18” 20” 22” 24” 26” 28”
Max OA Knee Brace
Max OA Knee Brace
Follow-up Patient Notes: ______
Fitter Name ______Date ______