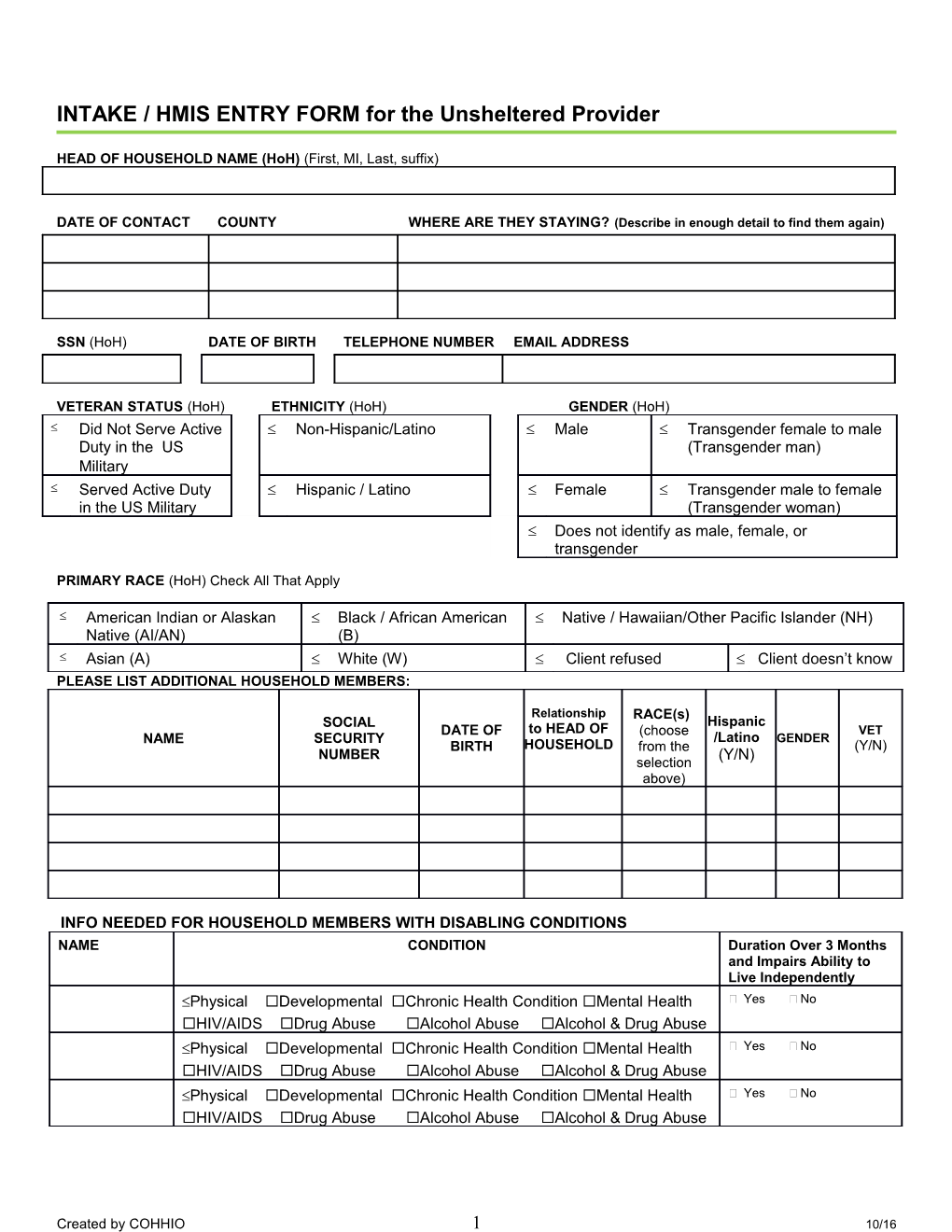
INTAKE / HMIS ENTRY FORM for the Unsheltered Provider
HEAD OF HOUSEHOLD NAME (HoH) (First, MI, Last, suffix)
DATE OF CONTACT COUNTY WHERE ARE THEY STAYING? (Describe in enough detail to find them again)
SSN (HoH) DATE OF BIRTH TELEPHONE NUMBER EMAIL ADDRESS
VETERAN STATUS (HoH) ETHNICITY (HoH) GENDER (HoH) Did Not Serve Active Non-Hispanic/Latino Male Transgender female to male Duty in the US (Transgender man) Military Served Active Duty Hispanic / Latino Female Transgender male to female in the US Military (Transgender woman) Does not identify as male, female, or transgender
PRIMARY RACE (HoH) Check All That Apply
American Indian or Alaskan Black / African American Native / Hawaiian/Other Pacific Islander (NH) Native (AI/AN) (B) Asian (A) White (W) Client refused Client doesn’t know PLEASE LIST ADDITIONAL HOUSEHOLD MEMBERS:
Relationship RACE(s) SOCIAL Hispanic DATE OF to HEAD OF (choose VET NAME SECURITY /Latino GENDER BIRTH HOUSEHOLD from the (Y/N) NUMBER (Y/N) selection above)
INFO NEEDED FOR HOUSEHOLD MEMBERS WITH DISABLING CONDITIONS NAME CONDITION Duration Over 3 Months and Impairs Ability to Live Independently Physical Developmental Chronic Health Condition Mental Health Yes No HIV/AIDS Drug Abuse Alcohol Abuse Alcohol & Drug Abuse Physical Developmental Chronic Health Condition Mental Health Yes No HIV/AIDS Drug Abuse Alcohol Abuse Alcohol & Drug Abuse Physical Developmental Chronic Health Condition Mental Health Yes No HIV/AIDS Drug Abuse Alcohol Abuse Alcohol & Drug Abuse
Created by COHHIO 1 10/16 CURRENT UNSHELTERED HOMELESS EPISODE: (please fill out separately for each adult if adults have different past living situations) Client Name (if multiple adults in the “Residence Prior Place not meant for Household with differing Residence to Project Entry” habitation Priors)
LENGTH OF STAY ZIP of Last Permanent Address More than 1 1 night or 90 days or more but week, but less less less than 1 year than 1 month 2 nights 1 year 1 to 3 to 1 or months week longer
TIME ON THE STREETS, EMERGENCY SHELTER, OR SAFE HAVEN Including this and any previous shelter stays or unsheltered episodes, Approximate Date / / Homelessness Started (Month/Day/Year): Total number of months homeless on the street, in ES Number of times the client has been on the street, in or SH in past 3 years? ES or SH in the past 3 years including today? Institutional stays of less than 90 days are not a break. Stays less than 7 days in other places are not a break. 1 2 3 4 5 6 7 8 9 10 11 1 2 3 4 or more 12 or more
ADULTS AFFECTED BY DOMESTIC VIOLENCE YES NO NAME EXTENT OF DOMESTIC VIOLENCE Within past 3 months Within the past 6-12 months Within the past 3-6 months More than 1 year ago Currently Fleeing? Yes No
Within past 3 months Within the past 6-12 months Within the past 3-6 months More than 1 year ago Currently Fleeing? Yes No
Notes
Created by COHHIO 2 10/16