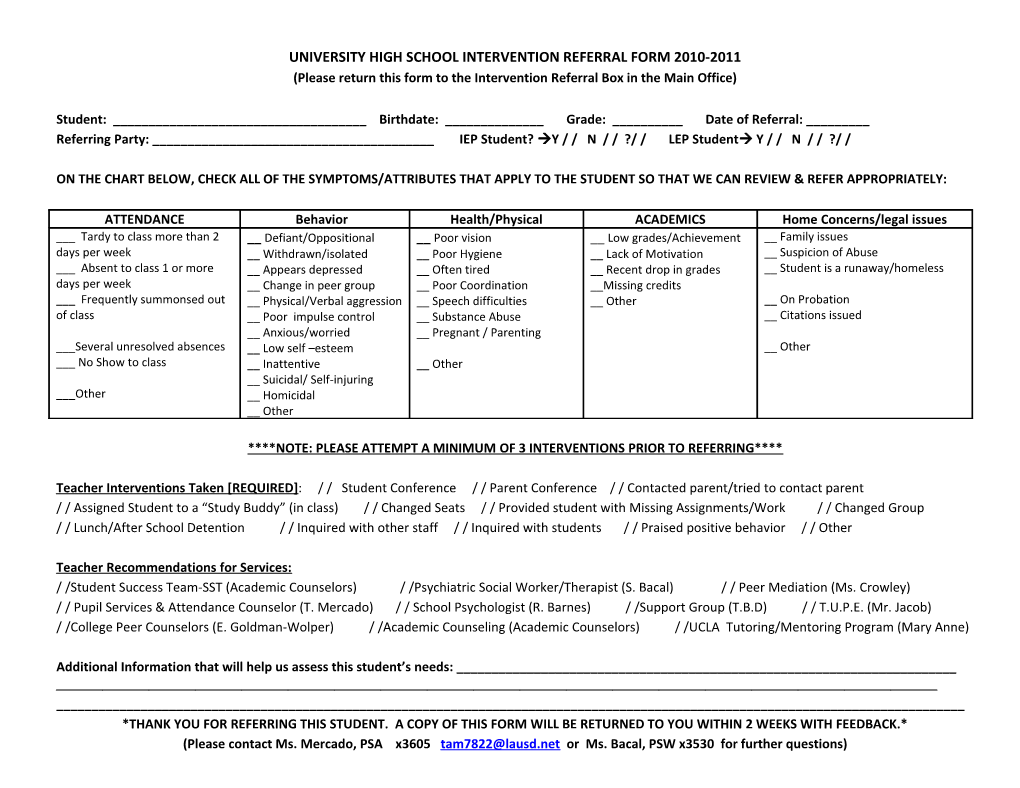
UNIVERSITY HIGH SCHOOL INTERVENTION REFERRAL FORM 2010-2011 (Please return this form to the Intervention Referral Box in the Main Office)
Student: ______Birthdate: ______Grade: ______Date of Referral: ______Referring Party: ______IEP Student? Y / / N / / ?/ / LEP Student Y / / N / / ?/ /
ON THE CHART BELOW, CHECK ALL OF THE SYMPTOMS/ATTRIBUTES THAT APPLY TO THE STUDENT SO THAT WE CAN REVIEW & REFER APPROPRIATELY:
ATTENDANCE Behavior Health/Physical ACADEMICS Home Concerns/legal issues ___ Tardy to class more than 2 __ Defiant/Oppositional __ Poor vision __ Low grades/Achievement __ Family issues days per week __ Withdrawn/isolated __ Poor Hygiene __ Lack of Motivation __ Suspicion of Abuse ___ Absent to class 1 or more __ Appears depressed __ Often tired __ Recent drop in grades __ Student is a runaway/homeless days per week __ Change in peer group __ Poor Coordination __Missing credits ___ Frequently summonsed out __ Physical/Verbal aggression __ Speech difficulties __ Other __ On Probation of class __ Poor impulse control __ Substance Abuse __ Citations issued __ Anxious/worried __ Pregnant / Parenting ___Several unresolved absences __ Low self –esteem __ Other ___ No Show to class __ Inattentive __ Other __ Suicidal/ Self-injuring ___Other __ Homicidal __ Other
****NOTE: PLEASE ATTEMPT A MINIMUM OF 3 INTERVENTIONS PRIOR TO REFERRING****
Teacher Interventions Taken [ REQUIRED ]: / / Student Conference / / Parent Conference / / Contacted parent/tried to contact parent / / Assigned Student to a “Study Buddy” (in class) / / Changed Seats / / Provided student with Missing Assignments/Work / / Changed Group / / Lunch/After School Detention / / Inquired with other staff / / Inquired with students / / Praised positive behavior / / Other
Teacher Recommendations for Services: / /Student Success Team-SST (Academic Counselors) / /Psychiatric Social Worker/Therapist (S. Bacal) / / Peer Mediation (Ms. Crowley) / / Pupil Services & Attendance Counselor (T. Mercado) / / School Psychologist (R. Barnes) / /Support Group (T.B.D) / / T.U.P.E. (Mr. Jacob) / /College Peer Counselors (E. Goldman-Wolper) / /Academic Counseling (Academic Counselors) / /UCLA Tutoring/Mentoring Program (Mary Anne)
Additional Information that will help us assess this student’s needs: ______
______*THANK YOU FOR REFERRING THIS STUDENT. A COPY OF THIS FORM WILL BE RETURNED TO YOU WITHIN 2 WEEKS WITH FEEDBACK.* (Please contact Ms. Mercado, PSA x3605 [email protected] or Ms. Bacal, PSW x3530 for further questions) REFERRAL FEEDBACK FORM
The student you referred was discussed by the Coordination of Services Team (COST) on ______. The following was determined:
Student was referred to:
/ /Student Success Team-SST (Academic Counselors) / /Psychiatric Social Worker/Therapist (S. Bacal) / / Peer Mediation (Ms. Crowley) / / Pupil Services & Attendance Counselor (T. Mercado) / / School Psychologist (R. Barnes) / /Support Group ______/ /College Peer Counselors (E. Goldman-Wolper) / /Academic Counseling (Academic Counselors) / /UCLA Tutoring/Mentoring Program (Mary Anne) / / Off campus tutoring / / Alternative Ed. Placement ______/ / T.U.P.E. (Mr. Jacob) / / LAUSD Homeless Unit / / LAUSD Foster Care Unit / / Referred to Mental Health Agency / / Probation / Law agency / / Basic Needs [food, shelter, transportation] / / Medi-Cal / / Healthy Families / / Private Insurance / / Other______
Additional Comments:
Revised 9/24/10