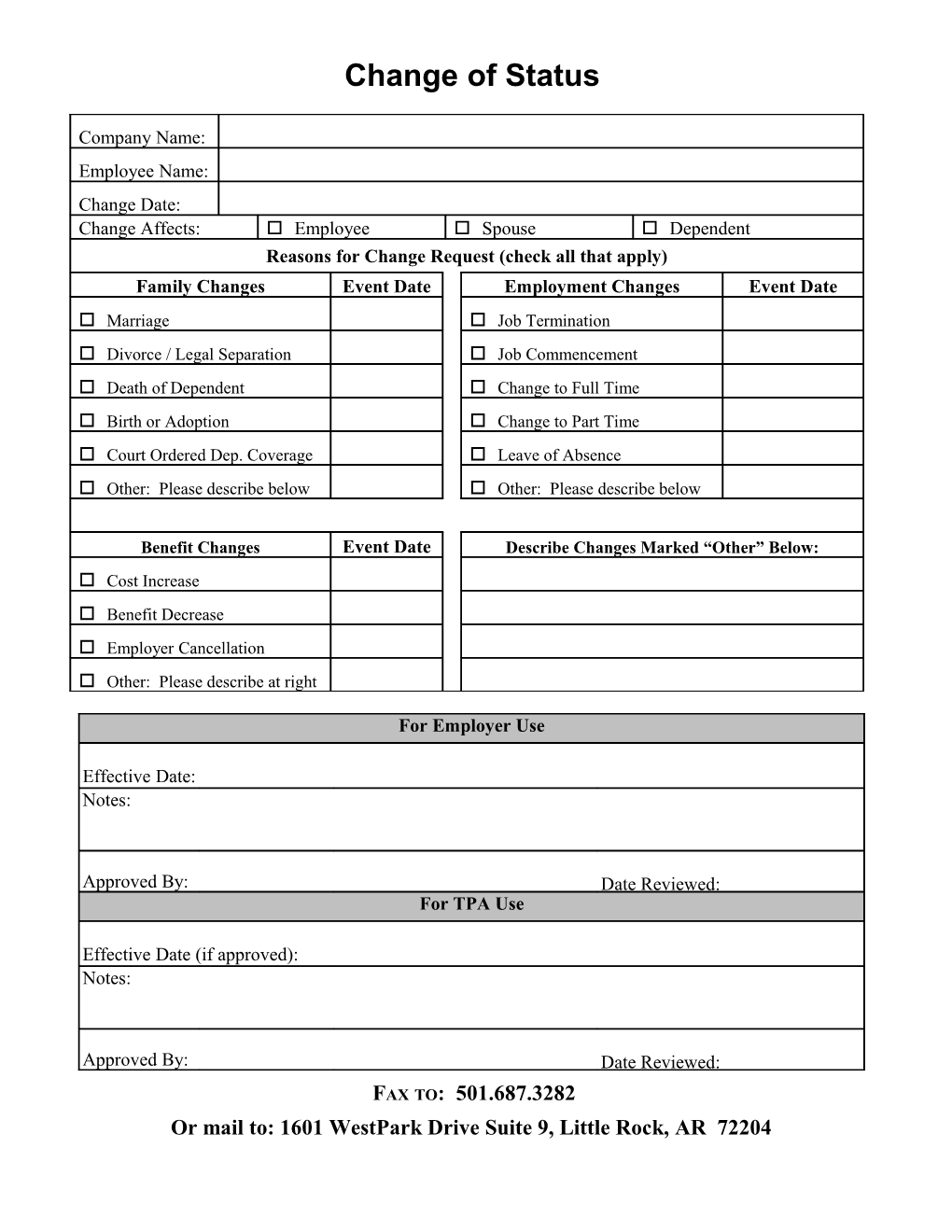
Change of Status
Company Name: Employee Name: Change Date: Change Affects: o Employee o Spouse o Dependent Reasons for Change Request (check all that apply) Family Changes Event Date Employment Changes Event Date o Marriage o Job Termination o Divorce / Legal Separation o Job Commencement o Death of Dependent o Change to Full Time o Birth or Adoption o Change to Part Time o Court Ordered Dep. Coverage o Leave of Absence o Other: Please describe below o Other: Please describe below
Benefit Changes Event Date Describe Changes Marked “Other” Below: o Cost Increase o Benefit Decrease o Employer Cancellation o Other: Please describe at right
For Employer Use
Effective Date: Notes:
Approved By: Date Reviewed: For TPA Use
Effective Date (if approved): Notes:
Approved By: Date Reviewed: FAX TO: 501.687.3282 Or mail to: 1601 WestPark Drive Suite 9, Little Rock, AR 72204