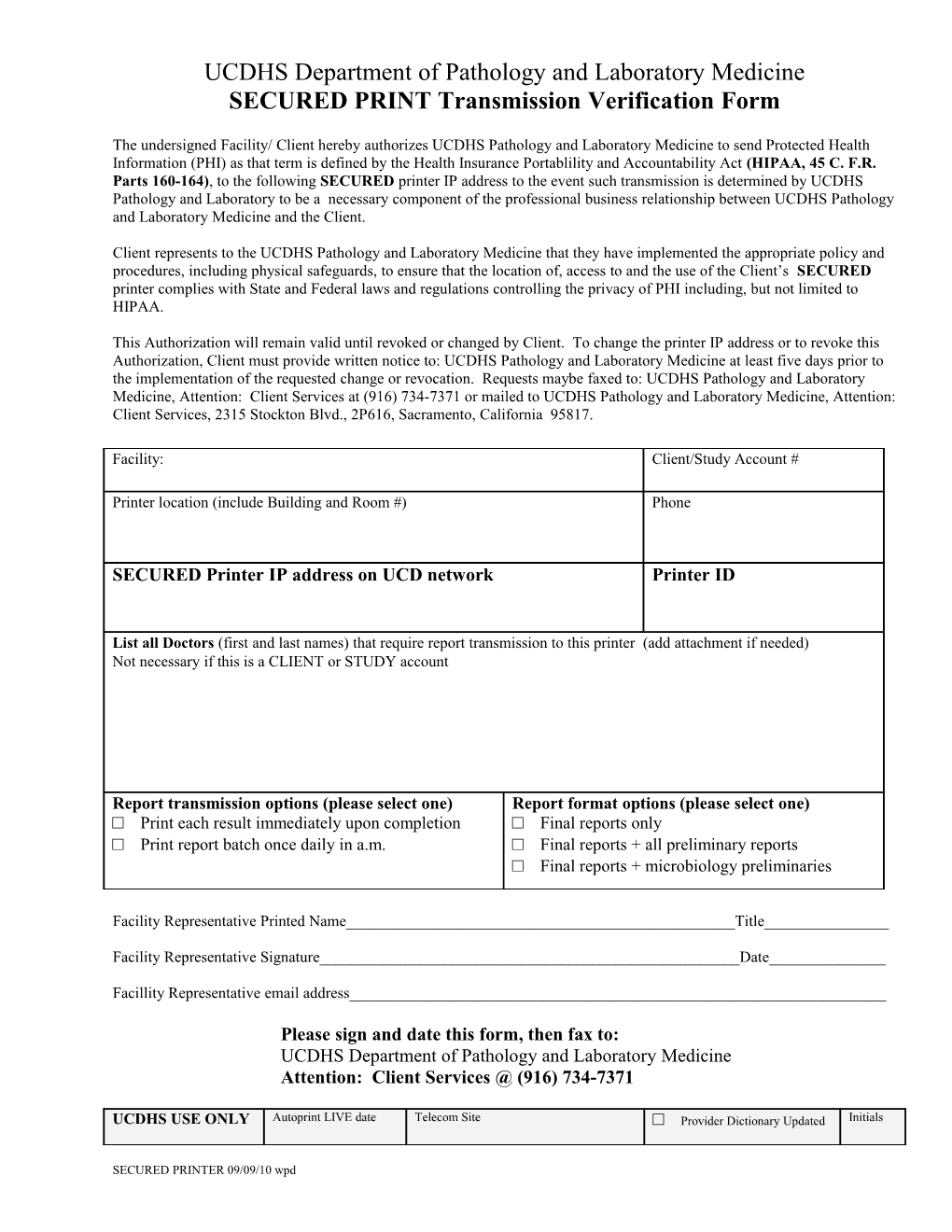
UCDHS Department of Pathology and Laboratory Medicine SECURED PRINT Transmission Verification Form
The undersigned Facility/ Client hereby authorizes UCDHS Pathology and Laboratory Medicine to send Protected Health Information (PHI) as that term is defined by the Health Insurance Portablility and Accountability Act (HIPAA, 45 C. F.R. Parts 160-164), to the following SECURED printer IP address to the event such transmission is determined by UCDHS Pathology and Laboratory to be a necessary component of the professional business relationship between UCDHS Pathology and Laboratory Medicine and the Client.
Client represents to the UCDHS Pathology and Laboratory Medicine that they have implemented the appropriate policy and procedures, including physical safeguards, to ensure that the location of, access to and the use of the Client’s SECURED printer complies with State and Federal laws and regulations controlling the privacy of PHI including, but not limited to HIPAA.
This Authorization will remain valid until revoked or changed by Client. To change the printer IP address or to revoke this Authorization, Client must provide written notice to: UCDHS Pathology and Laboratory Medicine at least five days prior to the implementation of the requested change or revocation. Requests maybe faxed to: UCDHS Pathology and Laboratory Medicine, Attention: Client Services at (916) 734-7371 or mailed to UCDHS Pathology and Laboratory Medicine, Attention: Client Services, 2315 Stockton Blvd., 2P616, Sacramento, California 95817.
Facility: Client/Study Account #
Printer location (include Building and Room #) Phone
SECURED Printer IP address on UCD network Printer ID
List all Doctors (first and last names) that require report transmission to this printer (add attachment if needed) Not necessary if this is a CLIENT or STUDY account
Report transmission options (please select one) Report format options (please select one) □ Print each result immediately upon completion □ Final reports only □ Print report batch once daily in a.m. □ Final reports + all preliminary reports □ Final reports + microbiology preliminaries
Facility Representative Printed Name______Title______
Facility Representative Signature______Date______
Facillity Representative email address______
Please sign and date this form, then fax to: UCDHS Department of Pathology and Laboratory Medicine Attention: Client Services @ (916) 734-7371
UCDHS USE ONLY Autoprint LIVE date Telecom Site □ Provider Dictionary Updated Initials
SECURED PRINTER 09/09/10 wpd Secured Printer Verification Form 08/04/11 wpd
SECURED PRINTER 09/09/10 wpd