Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 1 of 7 WBC = White Blood Cell; APC = Antigen Presenting Cell; NK cells = Natural Killer cells
Note: There’s a good outline for these slides posted online There’s a few slides in here that I don’t have any text for, but that’s probably because in class I didn’t catch exactly where he changed slides. I don’t think he completely skipped any of these slides (slides 1-32).
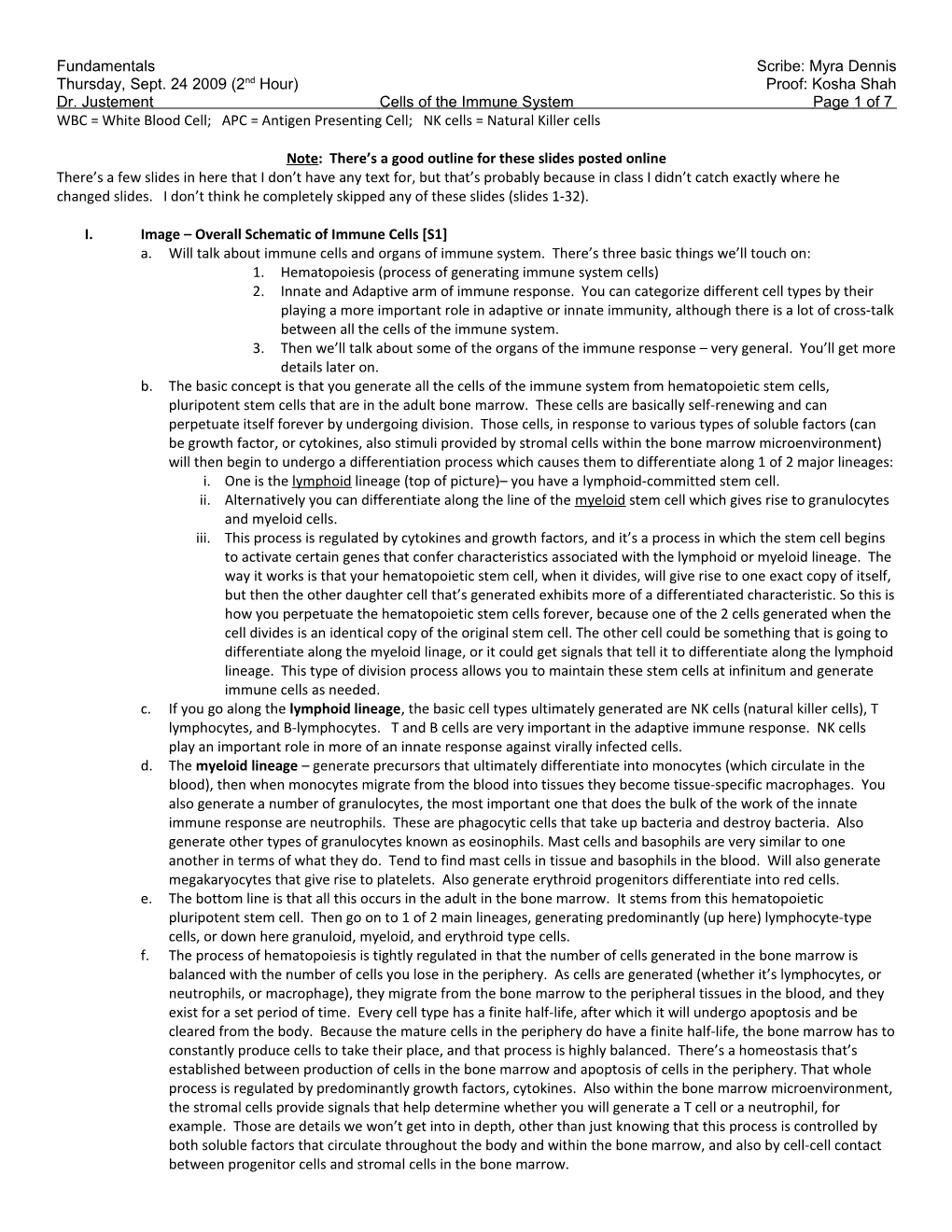
I. Image – Overall Schematic of Immune Cells [S1] a. Will talk about immune cells and organs of immune system. There’s three basic things we’ll touch on: 1. Hematopoiesis (process of generating immune system cells) 2. Innate and Adaptive arm of immune response. You can categorize different cell types by their playing a more important role in adaptive or innate immunity, although there is a lot of cross-talk between all the cells of the immune system. 3. Then we’ll talk about some of the organs of the immune response – very general. You’ll get more details later on. b. The basic concept is that you generate all the cells of the immune system from hematopoietic stem cells, pluripotent stem cells that are in the adult bone marrow. These cells are basically self-renewing and can perpetuate itself forever by undergoing division. Those cells, in response to various types of soluble factors (can be growth factor, or cytokines, also stimuli provided by stromal cells within the bone marrow microenvironment) will then begin to undergo a differentiation process which causes them to differentiate along 1 of 2 major lineages: i. One is the lymphoid lineage (top of picture)– you have a lymphoid-committed stem cell. ii. Alternatively you can differentiate along the line of the myeloid stem cell which gives rise to granulocytes and myeloid cells. iii. This process is regulated by cytokines and growth factors, and it’s a process in which the stem cell begins to activate certain genes that confer characteristics associated with the lymphoid or myeloid lineage. The way it works is that your hematopoietic stem cell, when it divides, will give rise to one exact copy of itself, but then the other daughter cell that’s generated exhibits more of a differentiated characteristic. So this is how you perpetuate the hematopoietic stem cells forever, because one of the 2 cells generated when the cell divides is an identical copy of the original stem cell. The other cell could be something that is going to differentiate along the myeloid linage, or it could get signals that tell it to differentiate along the lymphoid lineage. This type of division process allows you to maintain these stem cells at infinitum and generate immune cells as needed. c. If you go along the lymphoid lineage, the basic cell types ultimately generated are NK cells (natural killer cells), T lymphocytes, and B-lymphocytes. T and B cells are very important in the adaptive immune response. NK cells play an important role in more of an innate response against virally infected cells. d. The myeloid lineage – generate precursors that ultimately differentiate into monocytes (which circulate in the blood), then when monocytes migrate from the blood into tissues they become tissue-specific macrophages. You also generate a number of granulocytes, the most important one that does the bulk of the work of the innate immune response are neutrophils. These are phagocytic cells that take up bacteria and destroy bacteria. Also generate other types of granulocytes known as eosinophils. Mast cells and basophils are very similar to one another in terms of what they do. Tend to find mast cells in tissue and basophils in the blood. Will also generate megakaryocytes that give rise to platelets. Also generate erythroid progenitors differentiate into red cells. e. The bottom line is that all this occurs in the adult in the bone marrow. It stems from this hematopoietic pluripotent stem cell. Then go on to 1 of 2 main lineages, generating predominantly (up here) lymphocyte-type cells, or down here granuloid, myeloid, and erythroid type cells. f. The process of hematopoiesis is tightly regulated in that the number of cells generated in the bone marrow is balanced with the number of cells you lose in the periphery. As cells are generated (whether it’s lymphocytes, or neutrophils, or macrophage), they migrate from the bone marrow to the peripheral tissues in the blood, and they exist for a set period of time. Every cell type has a finite half-life, after which it will undergo apoptosis and be cleared from the body. Because the mature cells in the periphery do have a finite half-life, the bone marrow has to constantly produce cells to take their place, and that process is highly balanced. There’s a homeostasis that’s established between production of cells in the bone marrow and apoptosis of cells in the periphery. That whole process is regulated by predominantly growth factors, cytokines. Also within the bone marrow microenvironment, the stromal cells provide signals that help determine whether you will generate a T cell or a neutrophil, for example. Those are details we won’t get into in depth, other than just knowing that this process is controlled by both soluble factors that circulate throughout the body and within the bone marrow, and also by cell-cell contact between progenitor cells and stromal cells in the bone marrow. Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 2 of 7 g. This process of hematopoiesis can be modulated or up regulated. During inflammation, for example, an inflammatory response will generate cytokines, such as IL-1, IL-6, TNF-. When the cytokines are elevated in the body, they will have an affect on hematopoiesis in the bone marrow. A common thing seen during a bacterial infection is a great increase in white blood cell count. Because of that bacterial infection, cytokines are being produced which feed on the bone marrow and the hematopoietic process, causing it to be up regulated, so you generate much greater numbers of neutrophils, for example, which enter the blood and quickly play a role in dealing with the bacterial infection. There is a lot of cross-talk between the bone marrow microenvironment and the rest of the body, which can when necessary up regulate process of hematopoiesis to generate more white cells to respond to an infection. II. Table - Normal Adult Blood-Cell Counts [S2] a. Table of relative representation of cell types in adult human blood. b. White blood cells in terms of leukocytes – 7.3 x 103 cells/mm. Can see the breakdown of the different types of leukocytes. Neutrophils represent the largest proportion of white blood cells in the blood, followed by lymphocytes, and then a much smaller number of monocytes (which migrate into tissues and turn into macrophage). And eosinophil and basophil in the blood are a very small representation of white blood cell count. III. Image – Neutrophils, Eosinophils, Basophils [S3] a. Cells important for the innate immune response – first quick response of immune system to infection. Most important cell types are granulocytes, phagocytic cells (mainly include neutrophils and macrophage). Cells generally important for innate immunity are the granulocytic cells (3 types: neutrophils, eosinophils, and basophils). You can distinguish the cell types based on the morphology of their nuclei. If do a blood smear and look at cells under a microscope, you can distinguish them based on the shape of their nuclei. Can also use basic and acidic dyes – will stain granules of eosinophils and basophils differently so you can distinguish one from the other. b. Neutrophils are the highest percentage of cells in the blood in terms of the WBCs. They’re multi-lobed, phagocytic cells. They play an important role in responding very quickly to bacterial infection in terms of engulfing and destroying bacteria. Have a number of granules that contain hydrolytic enzymes, antibacterial peptides, etc that destroy the bacteria once it’s engulfed. Very quick to respond to infection. Accumulate in sites of infection in response to a number of different stimuli, including complement components, components of the blood clotting system, and a number of different cytokines that attract them to sites of infection. They are designed to come in and phagocytize bacteria and destroy them. Neutrophils are generally very short-lived. They really don’t have any other significant functions other than to come in and function as antimicrobials – they’re not long-lived. Don’t really play a role in driving the overall immune response beyond phagocizing and destroying bacteria. IV. Image – Infection [S4] a. When you have an infection – generally set up an inflammatory response, this causes vasodialtion, increased capillary permeability. You have leakage of plasma into the tissue, and that contains a number of factors that will recruit and attract neutrophils. You have up regulation of adhesion molecules on the endothelial lining. That enhances the rolling and migration of neutrophils from the blood into the tissue. This is what allows accumulation of the neutrophils at site of infection and enhances their ability to actively phagocytize the bacteria. V. Image - Neutrophils, Eosinophils, Basophils [S5] a. The other 2 types of granulocytes are eosinophils and basophils. Eosinophils are bi-lobed; have a granulated cytoplasm that stains with acidic dye (Eosin red). Relatively small component of blood leukocytes (1-3%). They are mobile, phagocytic cells. Can migrate from the blood into the tissue. Generally thought to play a role in fighting parasitic infections, also very true for basophils, at least from an evolutionary standpoint. These 2 cell types are thought to be important for fighting parasitic infections. VI. Image – Allergens [S6] a. Basophils and mast cells (similar to basophils cells in terms of function). Basophils are found mainly in blood. Mast cells are found mainly in tissue. Basophils are non-phagocytic, do not phagocytize particulate matter unlike neutrophils and eosinophils. b. What’s important about both basophils and mast cells is that they express the receptors that bind to the FC portion of IgE, the antibody isotype IgE. The FC receptors, which are expressed on surface of basophils and mast cells, will bind to IgE isotype antibodies. These cells come preloaded with IgE antibodies. If encounter an antigen that that antibody is specific for – for example you’re familiar with the role this plays in allergic responses. If you are allergic to something (like pollen), if you have mast cells and basophils that are preloaded with IgE in your body, and you’re exposed to that antigen/allergen, it will bind to the IgE on the surface of the cell and it will cross- link the antibody molecules, which causes the receptors in the membrane of the mast cell and basophil to become cross-linked themselves to relocalize in the membrane. This leads to a signaling cascade that causes both mast Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 3 of 7 cells and basophils to degranulate. They then release histamines and vasoactive factors that cause the allergic response VII. Image – Allergen Binding Diagram [S7] a. This is shown here in a more global schematic. Within the course of time, as you’re exposed to an allergen (pollen, food allergen, cat dander, etc.), you’re T and B cells respond to that. You have T and B cells that are specific for that allergic antigen. The B cells respond and make allergen-specific IgE. This IgE will then coat the surface of mast cells and basophils, and they become sensitized - preloaded with IgE antibody. Then when you are exposed to allergen, it will cause degranulation by cross-linking the receptors on the surface of the cell, driving a signal which causes the release of granules. The factors released cause smooth muscle cell contractions, small blood vessel dialation - all kinds of unpleasant, possibly deadly, in terms of allergic response. VIII. Image – Monocytes and Macrophages [S8] a. Monocytes differentiate into macrophage in tissues. These cells are very important in the innate immune response because play an important role in phagocytizing bacteria. But beyond the fact that it can take up bacteria and destroy them in lysozyme compartments, or phaglysomal compartments, macrophages are really important because they have the ability to carry out functions that begin to link the innate response with the adaptive immune response. Macrophages are one cell type that is very important in bridging the innate and adaptive immune responses. b. Monocytes are much smaller, much more rounded morphology. Single-lobed nucleus. They have relatively few granules in them that you can see. When they migrate in tissue, they undergo a differentiation process where they increase the number of pseudophods that they extend out. You see an increase in granules, increase in a lot of activity, activation markers of the cell. Can be further activated in response to inflammatory stimuli, like cytokines, complement factors, serum components associated with acute phase response. The macrophage really are localized in the tissue and are there to respond to any infectious organism (mainly bacteria) that they encounter. c. Macrophage have a lot of different names depending on the type of tissue you find them in. Don’t have to memorize the name for every tissue macrophage, but just be aware of these. i. In the connective tissue, they’re called histiocytes ii. Lung – Alveolar macrophage iii. Liver – Kupffer cells iv. Kidney – Mesangial cells v. Brain – Microglia cells vi. These are all macrophage in principle; they have more or less the same function. The key is that when macrophages are activated in response to inflammatory factors they up regulate reactive oxygen species, increase production of cytokines important for fighting infection, up regulation expression of defensins, or antibacterial peptides, they increase granule content which has hydrolytic enzymes. Also, they up regulate expression of receptions, important for enhancing their ability to take up bacteria. You can up regulate complement receptors, FC receptors, things that are important for binding to bacteria that have been opsonized by these different components of the immune response. IX. Image – Activation of Complement and Phagocytosis [S9] a. What’s really important about this is the idea of opsonization and the role this plays in enhancing bacterial uptake, via both neutrophils and macrophage. b. Opsonization – have a bacterium that can be coated with serum factors like mannose-binding protein, C reactive protein. Or it can be coated with complement components. Another example of something that can opsonize a bacterium are what are called natural antibodies that are produced all the time in your body that bind to polysaccrides in bacterial capsule. All of these agents will coat the surface of the bacterium. That enhances the ability of macrophages and neutrophils to engulf these bacteria or phagocytize them because neutrophils and macrophages express on their surface receptors for complement components, and express FC receptors that bind to the FC part of molecules bound to the bacteria. Or they express receptors for things like mannose-binding protein, C reactive protein. Any time the bacteria become coated, or opsonized, it enhances the ability of the phagocytic cells to take them up. This is really important, for example, if have an infection with a pneumococcus. Strepneumonia is highly encapsulated, which renders the bacterium relatively resistant to being phagcytized unless you can somehow opsonize it with one or more of these proteins to allow it to be bound more efficiently to macrophages and neutrophils. X. Image – Macrophage [S10] a. Important: When macrophage take up bacteria they have ability to begin to interface with cells of the adaptive immune response so we can move the process from the innate response to the adaptive response. Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 4 of 7 b. How this works: Bacteria are taken up in phagosomes. These phagosomes fuse with lysosomes, which contain hydrolytic enzymes. This generates the phagolysosome. You destroy the bacteria and generate peptides. These peptides are then loaded onto MHC Class II, and that peptide bound to MHC Class II is then expressed on the surface of the macrophage. This allows the macrophage to act as an APC (antigen presenting cell) which can then interact with a T cell. It can then present that bacterial peptide to the right T cell, and cause the T cell to become activated. That T-cell will then make cytokines, which are important both for driving both the innate immune response and initiating the adaptive immune response. It allows those activated T cells to interact with B cells. B cells become activated and can differentiate into antibody producing cells, which is one of the main functions of the adaptive immune response. Macrophage are very important for playing a role in the innate response, and in bridging the innate and adaptive immune response by their ability to present antigens to T cells. XI. Image – NK Cells [S11] a. NK cells (Natural Killer cells) - They are important for destroying, generally, virally infected cells. They do this in a way that is analogous to an innate immune response, because NK cells are more or less capable of recognizing what might be a virally-infected cell and killing it straight off without any long, ramping up time. This can act very quickly in an innate-type manner. b. NK cells have 2 types of receptors on their surface: activating receptors and inhibitory receptors. c. How NK cells work: Generally, the inhibitory receptors on NK cells bind to MHC Class I (or MHC Class I associated molecules) on the surface of tissues. This is important because generally every cell in your body normally expresses MHC Class I. Under normal conditions, NK cells will recognize MHC Class I by their inhibitory receptor and be kept turned off - they don’t kill. The signal to an inhibitory receptor will override – it’s dominate over the signal via the activating receptors. As long as the inhibitory receptor is engaging Class I, the NK cell doesn’t kill. In many cases when you have viral infections, it leads to down regulation of MHC Class I. Now, in a virally infected cell, you have no MHC Class I. The inhibitory receptor gets no signal. And now the activating receptor can drive the necessary signal to tell the NK cell to kill that target cell. They can be important for destroying cancer cells we think, because often when cells are transformed they will down regulate Class I. XII. Image – Continued diagram from Slide 11 [S12] XIII. Image – B and T Cells [S13] a. 2 main types of adaptive immune cells: T cells and B cells (T lymphocytes and B lymphocytes). These are the cell types critical for adaptive immunity. Generally can break down adaptive immune response into humoral response and cell-mediated response. b. Humoral immunity depends on B lymphocytes. In response to the right type of stimulus (right type of antigen), B cells will become activated and will expand in number. Those B cells that have ability to recognize a particular antigen will expand in number, and in response to the right type of signal, will ultimately differentiate into a plasma cell. Plasma cells will then secrete soluble antibodies, or soluble immunoglobulin. The soluble antibody secreted by a plasma cell is the exact same molecule that was originally expressed on the surface of the B cell as an antigen receptor. So it’s important to understand that for both T and B cells, each cell that circulates in your body, expresses a unique antigen receptor which confers upon that cell the ability to specifically recognize a particular antigen. In the case of B-cells that can be almost anything (a protein, nucleic acid, lipid, carbohydrate). If and when a particular B cell encounters the antigen that it is specific for, and it gets the right signals, it will undergo clonal expansion, differentiation, and then have generation of plasma cells that produce a soluble form of that same antigen receptor that was on the initial cell. c. T cells also express antigen receptors on their surface. Antigen receptors on T cells generally (particularly for alpha beta T cells) recognize peptides, small 8-12 amino acid peptides. They can only recognize peptides presented to them MHC Class I or II by APCs. When a T cell encounters the peptide it is specific for by its unique antigen receptor, it will undergo activation, clonal expansion, and differentiation. d. 2 main subclasses of T cells: i. T helper subclass – These are CD4 positive T cells. You can use markers, antibodies that are conjugated to fluorescent labels, and can actually visualize these cells using fluorescence microscopy. You can distinguish CD4 positive T cells from CD8 positive T cells. CD4 positive t cells have an antigen receptor that recognizes peptide in the context of MHC Class II. They differentiate into helper cells. Helper cells secrete cytokines that help B cells undergo activation and differentiation, they secrete cytokines that feedback and promote macrophage and neutrophils activation, secrete cytokines that potentiate the activation and differentiation of cytolytic T cells. ii. Other main is a cytotoxic T cell. These are CD8 positive. Express a receptor that recognizes peptide in the context of MHC Class I. When they see the appropriate antigen, they differentiate into cytolytic T cells. Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 5 of 7 Those t-cells are designed to lyse cells in your body that are infected with viruses or intracellular bacteria. This is called the cell-mediated response. Dependent on the CD8 positive cytolytic T cells. XIV. Image – Humoral and Cell-Mediated Response [S14] a. [Wasn’t sure when he changed slides, so I put slides 13 and 14 together] XV. Image [S15] a. Antigen receptors on B-cells express membrane immunoglobulin. (There’s only 1 associated heterodimer – error on slide). On the surface of a B cell that’s circulating in your blood or through lymph nodes or spleen, these cells express on their surface when they’re newly generated B cells. Express membrane IgM and IgD on their surface. These are 2 different isotypes, but both have the exact same antigen specificity. This is the antigen receptor, membrane immunoglobulin, sometimes called the B cell receptor. It has ability to bind 2 different antigenic epitopes. Terminates in a very short amino acid, 3 amino acid cytoplasmic tail. This antigen recognition structure is associated with a heterodimer called Ig-alpha Ig-beta. (Will get this all again later.) This is very important because this heterodimers is what transduces signal that leads to B cell activation. XVI. Image – Resting B Cell [S16] a. You have a resting B cell, it expresses this antigen receptor, membrane IgM, membrane IgD. If and when it encounters an antigen it is specific for, those receptors will be cross-linked, that will drive a signaling to the B cell. In response to that and other necessary signals, that cell will ultimately undergo expansion and differentiate into an anti-body secreting plasma cell. You are generating an adaptive immune response that is specific for the antigen you are challenged with. This is important to minimize autoimmune disease. XVII. Image – Maturation of B cells [S17] a. Important to note: Many different B cells, each with a different antigen receptor. The way it’s supposed to work is that only those cells that are specific for a particular antigen will respond, will undergo differentiation. Adaptive response specific for antigen XVIII. Image [S18]
XIX. Image [S19] a. On a T cell, have 2 types: alpha beta T cells, and gamma delta T cells. In either case, the antigen receptor itself is a heterodimer. Here’s an alpha-beta T cell receptor, you see you have a heterodimer, it’s disulfide bonded. Again, it ends in a very short cytoplasmic tail. This amino terminus will bind to a peptide presented either in context of MHC Class II or MHC Class I, depending on whether it’s a CD4 positive or CD8 positive T cell. This receptor is associated with a number of different polypeptides that are transmembrane polypeptides. This is CD3 complex here. These are very important for transducing signals leading to T cell activation. XX. Image [S20] XXI. Image – MHC Class I and II bind to CD8 and CD4 [S21] a. CD4 positive helper T cells. Cells that ultimately generate cytokines. The antigen receptor on a CD4 positive T cell binds to peptide that is presented on MHC Class II. CD4 will then bind to MHC Class II, helps stablize interaction between the T cell and the APC. A CD8 positive cytolytic T cell has an antigen receptor that binds to peptide presented by MHC Class I. On CD8 positive T cells, the CD8 molecule will bind to MHC Class I and help stabilize that interaction, allowing activation of T cells. XXII. Image – Summary of Adaptive Immune Cells [S22] a. Summary for basics of adaptive immune cells. B cells generate plasma cells that produce soluble antibody. T cells (CD4 positive helper) can produce cytokines. If CD8 positive cytolytic cells, they kill virally infected targets. XXIII. Image – Organs of Immune System [S23] b. Now we’ll talk about organs of immune system – will keep this fairly general. There are some simple discriminators with the organs of the immune system. One is primary vs. secondary lymphoid organs. c. Primary lymphoid organs - Organs in which hematopoiesis occurs. There are two primary organs: one is bone marrow (usually hip and sternum where hematopoiesis occurs, not the long bone like in this image) and thymus. d. Secondary lymphoid organs – spleen, lymph nodes, tonsils, intestine. The secondary lymphoid organs in general are very important because they provide discreet microenvironments within the body that allow T cells, B cells, and APCs to focus in a small region so that they are able to communicate with one another to mount the adaptive immune response. e. The Primary organs are important because for example in the bone marrow, this is where all the hematopoiesis occurs giving rise to all of the different cell types that are involved in the immune system, as well as platelets and red cells. f. Thymus – very important because where T cell development takes place. Thymic precursors are generated in the bone marrow, they migrate into the thymus and these thymic precursors then go through a developmental Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 6 of 7 process where you eliminate self-reactive thymacytes, and only allow those that respond to foreign antigens to survive so that you generate T cells in the periphery that are predominantly specific for foreign antigens as opposed self. XXIV. Image – Thymus [S24] a. Thymus is broken down into somewhat discrete regions. If look at a slice of thymus under the microscope, can visualize these different regions. Cortex, medulla. The thymic precursors migrate up into thymus, in the medulla, migrate up into the cortex where they undergo a selection process. Then they migrate back down into the medulla as they differentiate and mature into T cells. Then they leave the thymus and migrate into the periphery as mature T cells. So what we need to remember is that the thymus is important because it’s where thymic precursors migrate and undergo a process in which they mature and are selected to eliminate self reactive cells and to promote the survival and expansion of cells that react with foreign antigens. XXV. Image – Negative and Positive Selection in the Thymus [S25] a. In the thymus, have 2 processes: negative selection and positive selection. The idea is to generate CD4 positive and CD8 positive T cells that respond mainly to foreign antigens, foreign peptides, and not self-peptides. That’s the important role the thymus plays. XXVI. Image [S26] a. In bone marrow, in addition to hematopoiesis that generates all the cell types in the immune system, the other thing that occurs in the bone marrow that’s analogous to what happens in thymus with T cells is that B cells undergo a differentiation or developmental process in the bone marrow where they begin to rearrange the genes that encode the antigen receptor, then that is expressed on the surface and you have a process where self reactive B cells are eliminated and only those cells that respond to foreign antigen are expressed, or that express a receptor for a foreign antigen are allowed to migrate into the periphery. XXVII. Image – B Cell Development [S27] a. B cell development – goes through a number of steps. Don’t need to know details of this developmental process for this lecture. XXVIII. Image – Organs [S28] XXIX. Image – Lymphatic System [S29] a. The largest organs in terms of the immune system are the lymphatic vessels, ducts, and lymph nodes. Throughout your tissue you gave lymphatic capillaries that drain into lymphatic vessels. These lymphatic vessels bring lymph into regional lymph nodes. In the tissue where lymph comes from as blood circulates through the body and goes through the post-capillary venuoles, plasma leaks out to some degree into the tissue, some of it it reabsorbed into circulation. Some of that fluid is picked up by lymphatic system and become lymph. That lymph is what flows through the lymphatic vessels and carries both immune cells and antigens derived from the tissues. The flow of lymphatic is a passive process because within the lymphatic vessels you have one-way valves. Movement of lymph is all driven my muscle contraction, so lymph can only flow in one direction. Here it’s flowing from the tissue space towards the lymph node via the afferent lymphatic vessel. Lymph will then dump into the lymph node. Lymph can then leave the lymph node via the efferent lymphatic vessel. A one-way process. The important thing is that it’s designed to pick up cells and antigens from tissues and to bring those cells and antigens to regional lymph nodes where you have an aggregation of T and B cells in a defined region so that those cells, along with APCs, can respond to the antigen. XXX. Image [S30] a. Showing the same thing. You have resident immune cells in the epidermis, including Langerhan cells, which are dendritic cells. And also have intraepidermal lymphoctyes. In dermis have tissue macrophage, have lymphocytes that can migrate in from the blood to the dermis. But the lymphatics drain cells and antigens from the tissue and bring them to the lymph node. This is important because this is how your body controls, or samples, for foreign antigens. XXXI. Image – Lymph Node [S31] a. All of the secondary immune organs are divided into discrete regions. This is really important because it keeps T and B cells localized into the lymphatic organs but they don’t normally interact until an infection is ongoing. b. For example, this is schematic for a lymph node. Can see several discrete regions. You have the cortex, paracorex, and medulla - kinda like the thymus in a way. The outermost region of the cortex is where you find the B cells. This where you will see primary follicles and secondary follicles, called germinal centers. c. Interior region called the Paracortex – where T cells reside. B and T cells are kept restricted within these discrete regions of the lymph node because they express chemokine receptors on their surface. T cells express one kind of chemokine receptor, and B cells express a different kind. If look at gradient of chemokine that binds to those receptors, the B cell specific chemokines are very high in the cortex, which is why the B cells are retained in the Fundamentals Scribe: Myra Dennis Thursday, Sept. 24 2009 (2nd Hour) Proof: Kosha Shah Dr. Justement Cells of the Immune System Page 7 of 7 cortex. The T cell specific chemokines are higher in concentration in the paracortex, which keeps the T cells localized in the paracortex. Can watch these cells migrate within the lymph node and can see the T cells migrate up to the B cell zone and they turn around and migrate back down in. Because they’re responding to this chemokine, as long as its there it holds the T cell in a localized region. During an immune response, you have changes in the levels of chemokines and changes in expression of chemokine receptors. T and B cells can begin to migrate back and forth between these regions, which enables them to begin to talk to one another to mount the immune response. That’s fairly complex, but that’s generally how it happens. Lymphatics and lymph nodes are very important for sampling antigens from tissues. XXXII. Image - Spleen [S32] a. Spleen is also segregated, into red pulp and white pulp b. White pulp – surrounds periarterial lymphatic sheath (PALS). Within white pulp have segregation of B and T cells. T cells tend to line right long the PALS and the B cells are found in a region outside of the T cells. Kept segregated by chemokines and chemokine receptors. c. Important thing – spleen is there to sample antigens from the blood. The spleen does not pick up antigens from tissues, because there’s no lymphatic connection to the spleen. Blood comes in and percolates into marginal sinus (which is right in between red and white pulp). There are special cells there (macrophage and dendritic cells, APCs) that can pick up the antigens in the blood that percolates through the marginal sinus. Those special APCs will migrate into the T cell zone, where they can present those antigens to T cells and promote the activation process. Spleen samples blood antigens, lymphatic samples tissue antigens.
For mucosal sites, similar thing holds true. It’s the same segregation of T cells and B cells, but they’re there to provide a location in which these cells can interact.
(End 50 min.)