______
Student: Medical Diagnosis: Date: Client Initials: Date of Admission:
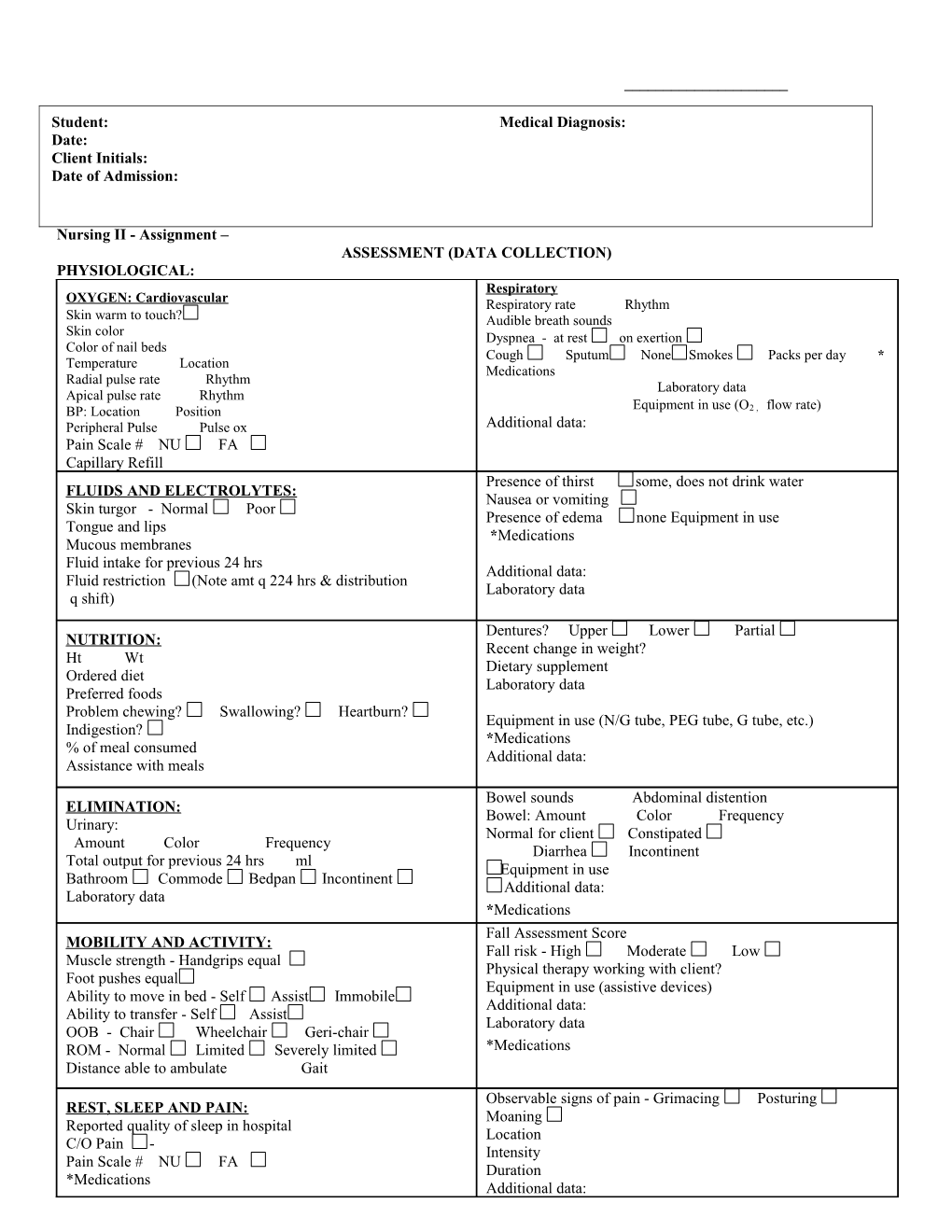
Nursing II - Assignment – ASSESSMENT (DATA COLLECTION) PHYSIOLOGICAL: Respiratory OXYGEN: Cardiovascular Respiratory rate Rhythm Skin warm to touch? Audible breath sounds Skin color Dyspnea - at rest on exertion Color of nail beds Cough Sputum None Smokes Packs per day * Temperature Location Medications Radial pulse rate Rhythm Laboratory data Apical pulse rate Rhythm BP: Location Position Equipment in use (O2 , flow rate) Peripheral Pulse Pulse ox Additional data: Pain Scale # NU FA Capillary Refill Presence of thirst some, does not drink water FLUIDS AND ELECTROLYTES: Nausea or vomiting Skin turgor - Normal Poor Presence of edema none Equipment in use Tongue and lips *Medications Mucous membranes Fluid intake for previous 24 hrs Additional data: Fluid restriction (Note amt q 224 hrs & distribution Laboratory data q shift)
Dentures? Upper Lower Partial NUTRITION: Recent change in weight? Ht Wt Dietary supplement Ordered diet Laboratory data Preferred foods
Problem chewing? Swallowing? Heartburn? Equipment in use (N/G tube, PEG tube, G tube, etc.) Indigestion? *Medications % of meal consumed Additional data: Assistance with meals
Bowel sounds Abdominal distention ELIMINATION: Bowel: Amount Color Frequency Urinary: Normal for client Constipated Amount Color Frequency Diarrhea Incontinent Total output for previous 24 hrs ml Equipment in use Bathroom Commode Bedpan Incontinent Additional data: Laboratory data *Medications Fall Assessment Score MOBILITY AND ACTIVITY: Fall risk - High Moderate Low Muscle strength - Handgrips equal Physical therapy working with client? Foot pushes equal Equipment in use (assistive devices) Ability to move in bed - Self Assist Immobile Additional data: Ability to transfer - Self Assist Laboratory data OOB - Chair Wheelchair Geri-chair ROM - Normal Limited Severely limited *Medications Distance able to ambulate Gait Observable signs of pain - Grimacing Posturing REST, SLEEP AND PAIN: Moaning Reported quality of sleep in hospital Location C/O Pain - Intensity Pain Scale # NU FA Duration *Medications Additional data:
SAFETY AND SECURITY: Speech: Vision: Clear Garbled Incomprehensible Able to see without glasses Needs glasses Allergies Able to read own menu Watches TV from ft Laboratory data *Medications Mental status: Skin integrity: Alert Lethargic Unresponsive Intact Reddened Location Oriented to - Person Time Place Blancing erythema Non-blancing erythema *Medications Incision/Lesion/Wound Location Environment: Appearance Approx. size in cms Physical surroundings Treatment (dressings) *Medications *Medications Additional data: Hearing: Responds to normal voice tones Hearing aid Deaf Braden/Norton Score # Risk: High Moderate Low
LOVE AND BELONGING: Indicators - Cards Flowers Family pictures Client report of family/friends Additional data: Next of kin (chart) Religious affiliation
SELF-ESTEEM: Occupation Family role Additional data: Grooming equipment at bedside: Brush/comb Toothbrush Toothpaste Interest in appearance Other personal toiletries
SELF-ACTUALIZATION: Independence Client report of satisfaction with life Creativity Additional data:
ERIKSON=S STAGE OF DEVELOPMENT: The client is at the following developmental stage and explain why:
*Always include name of medication, dose, route and time. assessment NSG II Spring 08