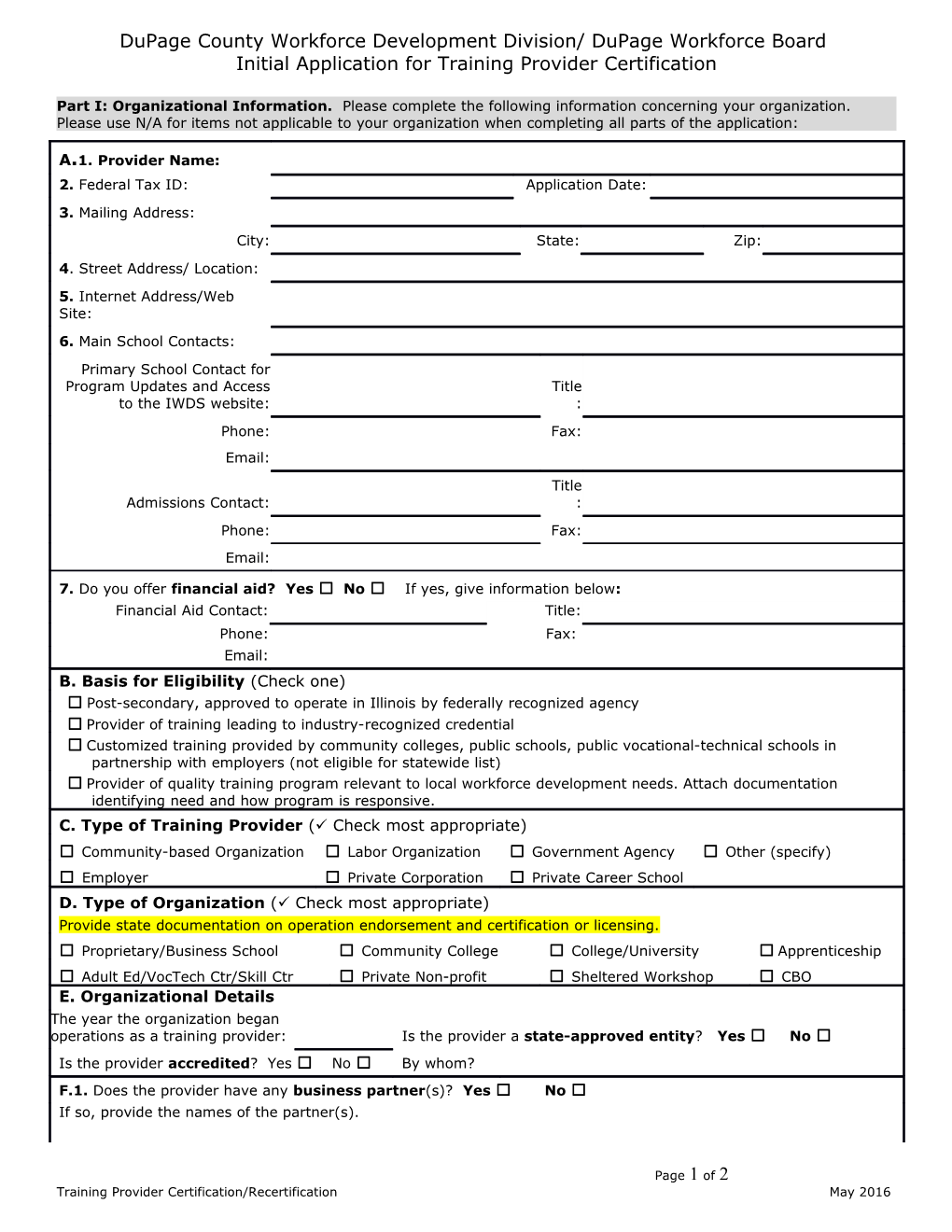
DuPage County Workforce Development Division/ DuPage Workforce Board Initial Application for Training Provider Certification
Part I: Organizational Information. Please complete the following information concerning your organization. Please use N/A for items not applicable to your organization when completing all parts of the application:
A.1. Provider Name: 2. Federal Tax ID: Application Date: 3. Mailing Address: City: State: Zip: 4. Street Address/ Location: 5. Internet Address/Web Site: 6. Main School Contacts: Primary School Contact for Program Updates and Access Title to the IWDS website: : Phone: Fax: Email: Title Admissions Contact: : Phone: Fax: Email:
7. Do you offer financial aid? Yes ☐ No ☐ If yes, give information below: Financial Aid Contact: Title: Phone: Fax: Email: B. Basis for Eligibility (Check one) ☐ Post-secondary, approved to operate in Illinois by federally recognized agency ☐ Provider of training leading to industry-recognized credential ☐ Customized training provided by community colleges, public schools, public vocational-technical schools in partnership with employers (not eligible for statewide list) ☐ Provider of quality training program relevant to local workforce development needs. Attach documentation identifying need and how program is responsive. C. Type of Training Provider ( Check most appropriate) ☐ Community-based Organization ☐ Labor Organization ☐ Government Agency ☐ Other (specify) ☐ Employer ☐ Private Corporation ☐ Private Career School D. Type of Organization ( Check most appropriate) Provide state documentation on operation endorsement and certification or licensing. ☐ Proprietary/Business School ☐ Community College ☐ College/University ☐ Apprenticeship ☐ Adult Ed/VocTech Ctr/Skill Ctr ☐ Private Non-profit ☐ Sheltered Workshop ☐ CBO E. Organizational Details The year the organization began operations as a training provider: Is the provider a state-approved entity? Yes ☐ No ☐ Is the provider accredited? Yes ☐ No ☐ By whom? F.1. Does the provider have any business partner(s)? Yes ☐ No ☐ If so, provide the names of the partner(s).
Page 1 of 2 Training Provider Certification/Recertification May 2016 2. Are all facilities ADA compliant? Yes ☐ No ☐ 3. Does the organization have a written EO/Non-Discrimination Statement? Yes No Please attach copy. 4. Attach copy of organization’s program/class cancellation and refund policies. 5. If you operate in other Local Workforce Innovation Areas (LWIAs) besides DuPage County/LWIA 06, please note which one(s):
G. List the name of all programs of study for which you are applying for certification. For purposes of this application, "program" is defined as involving multiple courses and leading to certification or licensure or completion of a degree or certificate. Attach additional pages as necessary. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10.
Supporting information to be submitted with this application: 1) Course Catalog 2) Verification of program costs 3) Program/class cancellation and refund policies 4) Provide documentation of state certification or licensing, and documentation of any other accreditation, authorization or recognition the provider has received from any accrediting body or industry-recognized entity which sets the standards for the training programs and/or career field 5) Specific prerequisites for programs 6) Information regarding internships (if applicable) 7) Detailed description of the provider’s business partnerships and job search or placement assistance provided to students 8) Any other data that supports your request to be added to the Illinois Workforce Development System.
Please note: Collection of data to determine performance is required by law. By signing this application, the training provider agrees to supply this information at the conclusion as requested.
Training Provider Authorization Name: Title:
Signature Date: :
Submit completed application with original signature and supporting documents to: Technical Services Unit DuPage County Workforce Development Division 2525 Cabot Drive, Suite 302 Lisle, IL 60532 Or, via email to: [email protected]
Useful Information: CIP Codes - http://nces.ed.gov/ipeds/cipcode/search.aspx?y=55 - http://nces.ed.gov/pubs2002/cip2000/ SOC Codes - http://www.onetonline.org/ - http://stats.bls.gov/soc/home.htm
Page 2 of 2 Training Provider Certification/Recertification May 2016