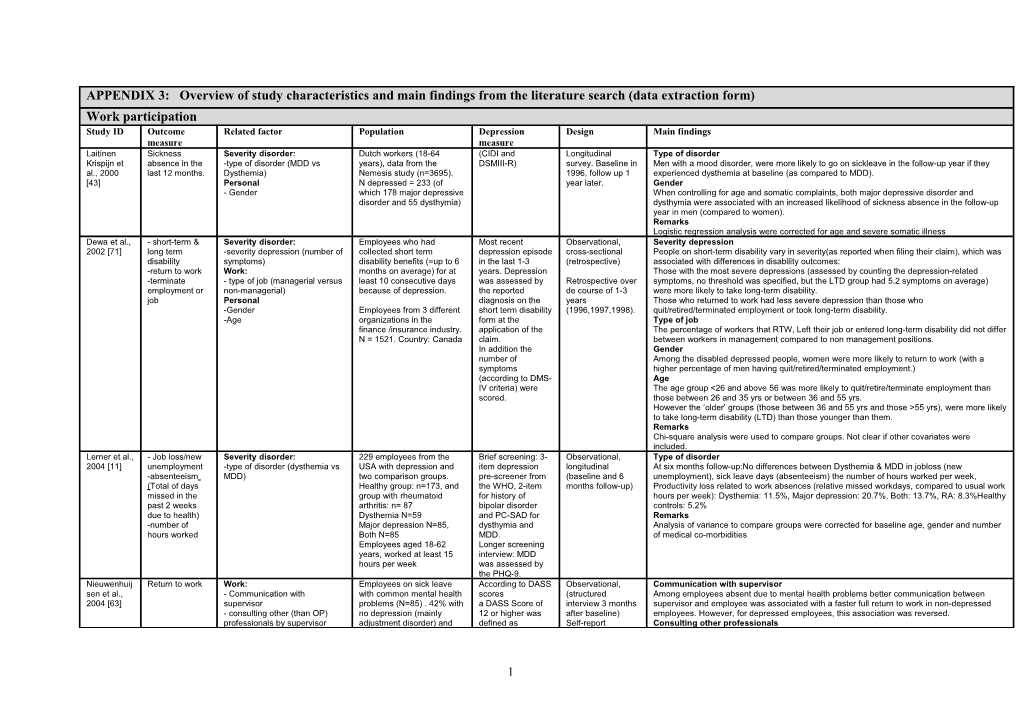
APPENDIX 3: Overview of study characteristics and main findings from the literature search (data extraction form) Work participation Study ID Outcome Related factor Population Depression Design Main findings measure measure Laitinen Sickness Severity disorder: Dutch workers (18-64 (CIDI and Longitudinal Type of disorder Krispijn et absence in the -type of disorder (MDD vs years), data from the DSMIII-R) survey. Baseline in Men with a mood disorder, were more likely to go on sickleave in the follow-up year if they al., 2000 last 12 months. Dysthemia) Nemesis study (n=3695). 1996, follow up 1 experienced dysthemia at baseline (as compared to MDD). [43] Personal N depressed = 233 (of year later. Gender - Gender which 178 major depressive When controlling for age and somatic complaints, both major depressive disorder and disorder and 55 dysthymia) dysthymia were associated with an increased likelihood of sickness absence in the follow-up year in men (compared to women). Remarks Logistic regression analysis were corrected for age and severe somatic illness Dewa et al., - short-term & Severity disorder: Employees who had Most recent Observational, Severity depression 2002 [71] long term -severity depression (number of collected short term depression episode cross-sectional People on short-term disability vary in severity(as reported when filing their claim), which was disability symptoms) disability benefits (=up to 6 in the last 1-3 (retrospective) associated with differences in disability outcomes: -return to work Work: months on average) for at years. Depression Those with the most severe depressions (assessed by counting the depression-related -terminate - type of job (managerial versus least 10 consecutive days was assessed by Retrospective over symptoms, no threshold was specified, but the LTD group had 5.2 symptoms on average) employment or non-managerial) because of depression. the reported de course of 1-3 were more likely to take long-term disability. job Personal diagnosis on the years Those who returned to work had less severe depression than those who -Gender Employees from 3 different short term disability (1996,1997,1998). quit/retired/terminated employment or took long-term disability. -Age organizations in the form at the Type of job finance /insurance industry. application of the The percentage of workers that RTW, Left their job or entered long-term disability did not differ N = 1521. Country: Canada claim. between workers in management compared to non management positions. In addition the Gender number of Among the disabled depressed people, women were more likely to return to work (with a symptoms higher percentage of men having quit/retired/terminated employment.) (according to DMS- Age IV criteria) were The age group <26 and above 56 was more likely to quit/retire/terminate employment than scored. those between 26 and 35 yrs or between 36 and 55 yrs. However the ‘older’ groups (those between 36 and 55 yrs and those >55 yrs), were more likely to take long-term disability (LTD) than those younger than them. Remarks Chi-square analysis were used to compare groups. Not clear if other covariates were included. Lerner et al., - Job loss/new Severity disorder: 229 employees from the Brief screening: 3- Observational, Type of disorder 2004 [11] unemployment -type of disorder (dysthemia vs USA with depression and item depression longitudinal At six months follow-up:No differences between Dysthemia & MDD in jobloss (new -absenteeism MDD) two comparison groups. pre-screener from (baseline and 6 unemployment), sick leave days (absenteeism) the number of hours worked per week, (Total of days Healthy group: n=173, and the WHO, 2-item months follow-up) Productivity loss related to work absences (relative missed workdays, compared to usual work missed in the group with rheumatoid for history of hours per week): Dysthemia: 11.5%, Major depression: 20.7%, Both: 13.7%, RA: 8.3%Healthy past 2 weeks arthritis: n= 87 bipolar disorder controls: 5.2% due to health) Dysthemia N=59 and PC-SAD for Remarks -number of Major depression N=85, dysthymia and Analysis of variance to compare groups were corrected for baseline age, gender and number hours worked Both N=85 MDD. of medical co-morbidities Employees aged 18-62 Longer screening years, worked at least 15 interview: MDD hours per week was assessed by the PHQ-9. Nieuwenhuij Return to work Work: Employees on sick leave According to DASS Observational, Communication with supervisor sen et al., - Communication with with common mental health scores (structured Among employees absent due to mental health problems better communication between 2004 [63] supervisor problems (N=85) . 42% with a DASS Score of interview 3 months supervisor and employee was associated with a faster full return to work in non-depressed - consulting other (than OP) no depression (mainly 12 or higher was after baseline) employees. However, for depressed employees, this association was reversed. professionals by supervisor adjustment disorder) and defined as Self-report Consulting other professionals
1 - promoting gradual RTW by 58% (N=49) with depression questionnaires, For employees with depression the duration of partial RTW was shorter (HR of 2.8) when supervisor depression longitudinal (follow their supervisor consulted other professionals (like a HR manager or a psychologist). up at 3, 6 and 12 Promoting gradual RTW months) This was unrelated to RTW. Remarks A multivariate Cox regression model was used, controlling for baseline depressive symptoms, age, gender, occupation and cause of mental health problems Buist- Work-loss Severity disorder: Netherlands Mental Health The Composite Observational data Co morbidity with Physical disorder Bouwman et Days unable to -comorbidity with Physical Survey and Incidence International (from the first wave Mood disorders are associated with an additive increase in work-loss days if they co-occur al., 2005 work in the disorder Study. This was a general Diagnostic of a prospective with a physical disorder. [70] previous 12 population study with 7076 Interview. study). Remarks months adults, aged between 18 Medically treated Linear regression analysis was used, controlled for sex, age and education. and 64 years of which 8.1% physical disorders (N=573) had a mood and work-loss were disorder at least 3500 were assessed using employed. self-reports. Druss et al., Annual sick Severity disorder Data from the health and depression, Observational, Physical condition 2000 [12] days -other physical health conditions employee files of 15,153 dysthymia or cross-sectional. Depressed employees that experienced an additional physical disorder (either diabetes, hart Personal employees of a major U.S. depressive disorder disease, hypertension or back problems) had more mean sick days than employees with only -age manufacturing corporation not otherwise Analyses a depression. who filed health claims in specified was compared the Age 1995 were examined. diagnosed mental health Depressed employees under the age of 40 years took 3.5 more annual sick days than those Of the 15.153 employees, (according to ICD- costs, medical 40 years old or older. 412 filed a health claim 9) during any costs, sick days, Remarks because of a depressive outpatient or and total health Regression models were used and controlled for : age, sex, race, income, geographic region, disorder. All employees inpatient treatment and disability costs education, salary, tenure with the corporation). received 1 or more episode associated with treatment sessions. depression and four other conditions: heart disease, diabetes, hypertension, and back problems.
Souêtre et Absenteeism Severity disorder Depressive patients (N = Patients diagnosed Cross sectional Severity disorder al., 1997 (Absent or not -symptoms severity 345) for major design, comparing The strongest predictors of absenteeism from work were symptoms severity, past history of [76] at the day of -past history of depression who were employed at the depressive disorder 3 treatment groups depression and past history of absenteeism (number of days missed in the past 3 months due measurement) -medial or psychiatric co- beginning of the current (MDD) as (2 with anti to illness). morbitiy depressive episode were assessed by the depressants and 1 Work Work: included. DSM III-R criteria no Wage (vs fees), full time employment (vs parttime) and having a non managerial position -Employee (vs management Subjects were sampled using the SCID and treatment group). increased the risk for absenteeism. position) were representative of the Hamilton Other factors -wage (vs fees) French population and Depression Rating No relationships with the other factors were found significant in the multivariate model. -full time employment contacted via the scale (HAM-D) Remarks -History of absenteeism ambulatory care setting. score higher than Multivariate logistic regression was used (controlling for demographics, co-morbidity, clinical, -type of company (private, Patients in the treatment 12 at the time of therapeutic and psycho-social aspects: see list of factors. administration or self-employed) group (n=268) were treated observation were Personal: with antidepressants for at selected. -Gender least 1 week and the non -Age (above 50) treated group (n=67) had -Martial status not received -living area antidepressants for at least -income level 1 month. Rytsälä et Long term work Severity disorder N=186 depressed Finnish The WHO Observational, Severity disorder al., 2007 disability -more time depressed within 18 patients,all belonging to the Schedules for longitudinal The risk of entering long term disability benefits within 18 months increased with:
2 [74] months labour force (but 29% was Clinical (patients were - time spent in major depressive episodes -severity of symptoms on sickleave at baseline) Assessment in assessed at Work - previous episodes Neuropsychiatry baseline, 6 and 18 The risk of entering long term disability benefits within 18 months increased with: -comorbid personality disorder In Finland then, all (SCAN) version 2.0 months). Baseline - being on sick leave at baseline (strongest predictor) Work: employed subjects were interview was used in 1997. - lower vocational education -occupational functioning insured by the Social to assess patients Personal -being on sick leave Insurance Institution, which had a current DSM The risk of entering long term disability benefits within 18 months increased with: Personal pays sickness allowance for IV major - higher age -Social functioning those who are temporarily depressive - being male -age incapacitated according to a disorder. Remarks -gender physicians evaluation. Severity of the Multivariate logistic regression was used (controlling for all factors listed) -hopeless depression - education symptoms was - marital status measured with the -alcoholism BDI and HAM-D - social adjustment -social support Kruijshaar et Sick leave in Severity disorder: Total NEMESIS Dutch The CIDI interview Observational, Severity of MD: al.. 2003 past 12 months -Mild, moderate, severe MD, population is n=7076, of was used to cross sectional. Mild and moderate MD differ significantly in number of absence days (Moderate more days), [42] (measured in severe with psychotic features which 6.2% (N=439) had a establish No significant difference between moderate and severe MD in absences. number of days) -Recurrent or single episode MD major depression in the last diagnoses of major Data from the first Type of MD: and “in the past year. At least 3500 were depression and to wave (1996) of Recurrent MD was not found to be associated with more absence days than single episode month” (5 employed. classify the type NEMESIS are used MD. classes: 0 days, 33.7% in people with an MD (recurrent, single) (on individuals Remarks 1-3 days, 4-7 had 1 or more absence and severity based diagnosed with MD Differences between groups were analysed with anova, correcting for confounders, but days, > 1 week days in the last year, and on the DSM-III-R. in 1996). unclear which. & <1 month, the 17.6% had been absent in whole time) the last month.
Rytsälä et Sick leave Severity disorder N=269 (Finish patients Diagnosis of Observational, Within the group that was employed at baseline independent predictors of being sick leave al., 2005 -severity depression diagnosed with DSM-IV depression cross-sectional. were [73] -number episodes MDD). assessed with face Baseline findings Severity disorder - comorbid somatic disease 157 were employed at to face interview (1997) of a - severe to psychotic depression (compared to mild&moderate), - comorbid personality disorder baseline, of which 68 (43%) using the WHO prospective cohort - more severe depressive symptoms (HAM-D) Personal were on sick leave. Schedules for study are - more previous of episodes of depression. -female In Finland then, all Clinical presented in this For the employed age group above 40 a somatic disease (and receiving medical treatment) -age employed subjects were Assessment in article. increased the risk of being on sick leave. -substance abuse insured by the Social Neuropsychiatry Personal Insurance Institution, which (SCAN), version - female sex, pays sickness allowance for 2.0. - age (above 50), those who are temporarily Substance abuse as well as personality disorders did not have a significant impact on the incapacitated according to a Severity of likelihood of sick leave. physicians evaluation. depression is Remarks assessed via the Multivariate logistic regression was used, controlling for sex, age, depression score and 17-item Hamilton number of previous episodes. Rating Scale for Depression (Ham- D) and the 21-item Beck Depression Inventory. Birnbaum et work absence Personal: N= 5295 Medical or disability Observational, Gender al., 2003 (prevalence & Gender Employed depressed claim with a longitudinal: Claim Employed women with depression have a 58% prevalence of rate of work absence compared [69] duration) subsample of administrative diagnosis of MDD data database to a 43% rate for comparable men. illness related claim data from an US (ICD-9 codes gathered between The duration of using disability benefits did not differ by gender. work absence insurance company with beginning with 1996 & 1998. Remarks (up to 5 days, over 100.000 beneficiaries 296.2 296.3 300.4 Unclear what statistical method was used and whether confounders were controlled for.
3 paid by the 309.0 309.1 311) employer) and disability claims paid by the employer (for 6 or more days).
Claassen et Work hours Severity N= 4037 17-item Hamilton Cross-sectional Prior suicide attempts al., 2007 missed Prior suicide attempts Baseline data from the Rating Scale for (baseline) data Patients with prior suicide attempts showed more work hours missed (26.2% vs 18.2%) due to [77] STAR*D trial in . Depression. ≥ 14. from multi-center health problems and fewer total hours actually worked (73.8% vs. 81.8%) in the week prior to Outpatients with MDD clinical trial. enrolment. treated in primary and Remarks specialty care settings in Bivariate logistic regression was used, with and without controlling for covariates of age, US. 58% was employed gender and severity of the depression. (n=2341). Druss et al., One or more Severity disorder N=1200. Depressed 12-item Short-Form Observational, Type of depression 2001 [68] days missed Type of depression: subgroup of employees Health Survey. < longitudinal (2 year The odds of sick days at the 2 year follow-up was 2.17 in Chronic depressed employees, in from work Chronic (1993+1995) vs. from three major US 43 on mental follow-up) comparison to 1.62 in the incident and 1.31 in the remitted group as compared to a non- because of Incident (1995 only) vs remitted corporations in 1993-1995. component depressed group. (not clear if these differences are significant) health problems (1993 only) Total Group N= 6239 summary Remarks in past 4 weeks Logistic regression analysis was used, controlling for age, gender, race, family income, education, number of chronic conditions, plan type and number of years enrolled in the plan. Sanderson absenteeism Severity disorder 436 call centre employees Patient Health Prospective (6 Severity et al., 2007 -severity (MDD vs Minor (response rate 53.4%) in Questionnaire month follow-up) Mean absenteeism days in the past 4 weeks at the 6 month follow-up were higher for [22] depression) Australia, of which 16% had - based on DSM- employees with MDD at baseline (compared to minor depression: 2.7 vs 1.3) -syndrome stability any depressive or anxiety IV, Syndrome stability syndrome Depressed employees that were depressed at baseline did not differ in their absence days at Minor depressive syndrome: follow-up dependent on their symptom recovery (people with remitted depression as well as n= 24, 5.6% with persisted depression did not change in their mean absence days over the past 4 weeks) Major depressive syndrome: Remarks n=25, 5.8% Linear regressions were used controlling for gender, age, and chronic physical health conditions. Stewart et Excess lost Severity disorder Employed individuals who Primary Care Observational, Severity al., 2003 productive time -severity (MDD/dysthemia, MDD participated in the American Evaluation of cross-sectional, Mean absenteeism hours per week differs between the 3 depression groups. On average 1.5 [21] (LPT) (self partial in remission). Productivity Audit . Mental Disorders data gathered in days for MDD partial in remission, 1.2 days for MDD and .05 days for Dysthymia (not clear if reported - comorbidity physical symptom Non depressed employees (PRIME-MD). 2001/2002 this difference is significant). absenteeism in cluster (N=908) were compared to Total LPT ( absenteeism & presenteeism together) shows the highest mean days per week for the past 2 219 clinically depressed MDD (8.4), followed by MDD partial in remission (5.3) and Dysthymia (3.3). (again no weeks and employees (87 with MDD, significances are presented) presenteeism) 74 with Dystemia, 58 with Comorbidity MDD partial in remission) Among participants with MDD a co-occurring physical symptom cluster was associated with more LPT. Remarks Multiple linear regressions were used, unclear whether confounders were controlled for. Sorvaniemi Granted Severity disorder 213 patients with first time Not mentioned. It Retrospective case The following factors showed to predictive of disability pensions: et al., 2003 disability -co morbid documented major were psychiatric note study Severity [75] pension due to major somatic disorder depression. outpatients with follow-up at 3 -co morbidity (more pensions when a major somatic disease was also present MDD -self-esteem (symptom) They all sought treatment at DSM-III-R major months (after first Personal -duration or severity of the a psychiatric policlinic in the depression time documented -Age (above 43, more pensions),), lowered self-esteem (lower, more pensions). current episode year, 1989, 1992 and 1995. (probably assessed MDD,) and 30 No other socio-demographic, clinical or treatment factors revealed any statistically significant Personal: Age between 18-64 (and in the outpatient months (for the association with being granted disability pension due to a major depression -Age non retired) clinics) granted pensions Remarks -Self esteem Country: Finland. information) Multivariate Cox’s regression analysis was used, controlling for marital status, gender, -Marial status 87% employed at baseline duration/severity current episode, treating professional, type of job, treating professional and -Educational level (N=185) adequacy levels of pharmacological treatment)
4 Work -type of job (entrepreneur, management employee, manual workers Simon et al., Absenteeism: Severity disorder: -Included: 290 patients who - depression Observational, Clinical improvement 2000 [40] -days missed -Severity/ had a major depressive module of the SCID longitudinal report. The mean number of days missed from work during the entire follow up (24 months) and the -maintain Clinical improvement episode at baseline AND - 17-item version of (data on work probability of paid employment were strongly related to clinical outcome at 12 months: employement who completed the 12- the Hamilton outcomes for over After adjustment for depression severity and medical co morbidity at baseline, - typical hours month follow-up. Depression Rating 24 months were patients with greater clinical improvement..: worked per -According to the 12 month Scale. compared with - missed fewer days from work (P<.001). week follow up patients were clinical outcome at - were more likely to maintain paid employment (P=.007) classified into 3 groups: 12 month follow Clinical improvement was unrelated to typical hours worked per week. 1) persistent depression up). Remarks 2) improved but not remitted Analyses: mixed model analysis of covariance, adjusted for age, sex, baseline depressive 3) remitted Data were symptoms, duration of depressive episode, baseline chronic disease, and baseline of outcome -At baseline, 229 of the 290 collected as part of measure participants were employed. a randomized -Analyses of days missed controlled trial from work were limited to comparing those working at each time (cost)effectiveness point (= 229 at baseline, of fluoxetine and 235 at 12 months and 211 tricyclic at 24 months). antidepressants in Country: USA primary care. Lépine, Days of lost Severity disorder A total of 13359 adults were Depression Structured Severity 1997 [41] work due to MDD vs Minor and depressive identified as suffering from diagnosis interviews, cross- The number of days of work lost in previous 6 months due to illness increased with the illness in symptoms. depression (5413 with according to MINI sectional severity of depression. Major depression had most impact work days lost (mean 12.7 days). previous 6 MDD, 1412 with minor (Sheehan et al, retrospective data For minor depression and depressive symptoms these mean work loss days were 10.2 and months depression and 6512 with 1994) and all had (over a course of 6 4.1 respectively across countries. These differences were not statistically tested (not depressive symptoms) consulted a months) gathered presented). healthcare in 1995. Remarks Between 35-53% (varying specialist about Statistical methods (and controlling for confounders) are unclear. across countries) was their symptoms in employed at baseline. the previous 6 months. 6 European countries: Belgium, France, Germany, In order to be Netherlands, Spain, UK. classified with MDD or minor depression a substantial impairment (either social or in work life) had to be present. Dewa et al., Probability to Severity disorder Claimants with depression- To reflect the Observational Severity 2003 [72] RTW Number of symptoms related absences from work number of using The probability to RTW was associated with: Co-morbidity (other mental and for at least 10 consecutive symptoms reported administrative data - less symptoms (The larger the number of symptoms, the smaller the odds ratio Duration until or physical disorder) days prior to their disability by the claimants, for claims in 1996- (OR¼0.83, 95% CI 0.78–0.89, P50.0001). RTW (length of Personal leave AND who have used they created a 1998 Personal disability for Age their prescription drug count of the The probability to RTW was associated with: those who Gender benefits at least once during number of - younger age (higher age: OR¼0.98, 95% CI 0.97–0.9998, P50.047). resumed their Work the study period for any depression-related The duration until RTW was shorter for those with less symptoms and was related to the work) Company effects (not specified) type of prescription AND symptoms company the participants were employed (overall workplace characteristics, not further who had no more than 1 recorded on the specified short-term disability episode short term disability Probability to RTW was unrelated to gender, company effects and co morbidity. Duration until
5 within the previous 12 application form. RTW was not associated with gender, age or co morbidity. months. Information was Remarks N=1281 for the probability abstracted from Mulitvariate logistic regression analysis included anti-depressant medication use, gender, age, analysis and N=997 for the occupational health co morbidity and ‘company fixed effects’. duration analysis. records using a Data were used from 3 checklist covering financial and insurance the major DSM IV sector companies which self depressive funded and self symptom administered their short- categories term disability benefits. Country: Canada Work functioning Study ID Outcome Related factor Population Depression Design Main findings measure measure Adler et al., Work Severity disorder: n=572 primary care Depressive Longitudinal Symptom level: 2006 [24] limitations / Job - Symptom level patients, 81 % women, symptom severity observational, Change in job performance deficits were correlated with symptom severity. Clinical performance - Recovery all working for at least 15 was based on the case-control. improvement of depression does not result in full recovery of job performance at 18 month i.e. deficits (assessed temporal changes in hours per week, USA weighted sum of Measurements at in comparison with healthy controls.) a) Mental- job performance Patient Health baseline, 6, 12, and Recovery: Interpersonal among depression group n=286 patients with Questionnaire- 9 18 months Between baseline and 6 months: in improved group and in same severity group significantly demands subjects defined as clinically DSM-IV major depressive symptoms (PHQ-9) declined job performance deficits. In worse group no significant changes. Between 6 and 18 b) Physical job improved, disorder (n=105) and/or month follow-up no significant changes in any group. demands the same, or worse). Dysthymia (n=72) and/or PHQ-9 item version Remarks c) Output double depression (n=109) gives depression All analyses are adjusted for age, gender and number of chronic medical conditions. demands were compared to n=93 severity score; d) Time individuals improvement, the management with rheumatoid arthritis same or worse demands (RA), a condition measured as associated with work differences disability, and n=193 between baseline depression-free healthy and 6 month follow- control subjects. up
Clinically improvement n=48 ; the same n=176 ; worse n=62.
Participants were employed and did not plan to stop working, and had no major medical co-morbidities Lerner et al., Work limitations Severity disorder: Sample (n=389) Office-based Observational, Severity of depression: 2004 [81] a) Mental- - Symptom level consists of 246 employees screener (incl. 3 Cross-sectional In workers with either dysthymia, MDD, or Double Depression: number of symptoms was Interpersonal (Number/severity of with depression item depression significantly related to more work limitations measured with the WLQ, all four subscales. demands symptoms) (dysthymia= 64; MDD= pre-screener based Type of occupation: b) Physical job Work: 89; Dysthymia + MDD =93) on CIDI and new In workers with either dysthymia, MDD, or both: sales, service, or support occupation was demands Type of job and 143 healthy developed significantly related to more work limitations measured with the WLQ, subscales Mental- c) Output controls. Female: 88% depression Interpersonal and Physical job demands (not WLQ Output and WLQ Time), compared to demands Subjects recruited screener for production, construction, repairs, transport occupations. d) Time between Feb 2001 -Feb primary care), Remarks management 2003 from primary care physician checklist, Analyses were adjusted for age and gender. demands physicians’ offices in and in-depth Massachusetts (USA). interview to determine eligibility
6 Lerner et al., Severity disorder: N=229 employees from Brief screening: 3- Observational, Type of depression: 2004 [11] Presenteeism, - Type of USA with depression item depression longitudinal Presenteeism results in the three depression groups, at baseline: work limitations (mental– a) Mental- depression( dysthymia vs. - Dysthymia N=59 pre-screener from interpersonal and output demands) significantly differed from each other. The dysthymia group Interpersonal MDD or Dysthymia + MDD) - MDD N=85 the WHO, 2-item had lowest depression severity and also the lowest level of work limitations. Physical and time demands - Dysthymia + MDD N=85 for history of management demands did not differ between the groups. b) Physical job bipolar disorder At follow-up: only time management significantly differed between the three depression groups demands Two comparison groups: and PC-SAD for with the dysthymia group showing the lowest level of work limitations. No differences were c) Output healthy group: n=173, and dysthymia and found for physical, mental/interpersonal and outpt demands between the groups. demands group with RA: n= 87 MDD. Remarks d) Time Longer screening Analyses were adjusted for baseline age, gender and number of physician-diagnosed medical management interview: MDD co-morbidities. demands assessed with PHQ-9. Sanderson et - Presenteeism, Severity disorder: Staff in ten call centres Patient Health Longitudinal At baseline: work limitations (time management, mental/interpersonal, and output demands but al., 2007 [22] (number of days - symptom level (minor vs. including a Questionnaire observational (6 not the physical demands) were related to severity of depression. Presenteeism days but not attending work major depression based on total of 817 Australian call - based on DSM- months follow-up) inefficiency days were related to severity of depression. unwell) number of symptoms) centre employees invited IV, diagnostic The association between presenteeism and depression severity was examined in subgroup - inefficiency (response n=436, 53.4%) variables include on=49 depressed workers at baseline. days major depressive Remarks - Work PHQ diagnoses in baseline syndrome, minor Analyses were adjusted for age, gender, presence of chronic physical health condition limitations population (n=432): depressice Minor depressive syndrome: syndrome, panis n= 24, 5.6% syndrome, othet Major depressive syndrome: anxiety syndrome n=25, 5.8% Panic syndrome: n=27, 6.3% Other anxiety syndrome: N=16, 3.7% Any depressive syndrome: n=69, 16.0% Stewart et al., Health-related Severity : depression Employed individuals from Primary Care Observational, Severity of depression 2003 [21] lost productive - Type of depression (MDD vs. the USA who participated in Evaluation of cross-sectional Presenteeism (in hours per worker per week): any depression 4.6, major depression 7.2, time (LPT) Dysthymia) the American Productivity Mental Disorders dysthymia 2.7 partial remission or recurrence of major depression 3.8, expected mean LPT in - Recovery (recurrence, partial Audit were eligible for the (PRIME-MD). absence of depression 1.1 remission, absence of Depressive Disorder Study. depression) n=692 responded affirmatively to two depression screening questions, 435 where randomly selected (1:4) who responded negatively. Of those, 219 were clinically depressed (206 from positive screen group and 13 from negative screen group) and compared to N=908 with no depression
Any depression N=219 of which: Major depression N= 87; Dysthymia N=74; Partial remission or recurrence of major depression N=58
7 Kornstein et Work Personal 235 male and 400 female DSM-III-R chronic Subjects in this Gender al., 2000 [80] impairment, - gender outpatients with chronic major depression study are Men showed significantly greater work impairment when compared with women (p=0.016; (functional major depression or double or double participants in a mean (SD) 2.26 (0.65) vs 2.12 (0.59) on SAS-SR – Work impairment) depression, of which n=151 depression, plus large prospective Remarks men (66.5%) and n=239 HAM-D rating and multi-center study Analyses were adjusted for age, treatment group, depression type, and pooled investigator site. women (61.1%) are CGI comparing employees at baseline sertraline and (26% of the men are imipramine in the unemployed and 17.4% of treatment of the women) (N=390) chronic depression Setting:USA Michon et al., Impaired work Personal Data obtained from the first Mental disorders Data from Personal 2008 [82] functioning, - neuroticism, self-esteem, two waves (T0 and T1) of were assessed NEMESIS Higher neuroticism, more external locus of control and lower self-esteem at baseline were mastery NEMESIS using the CIDI to (prospective significantly associated with stronger impairment in WF 1 year later, irrespective of 11-months Setting: The Netherlands assign DSM-III-R epidemiological prevalence of common mental disorder diagnoses. Here 3 survey on the Relationship between the mental disorders and subsequent WF weakened once the influence Main analyses were carried main categories: mental health of of the personality factors was brought into the analyses, e.g., the weight of mood disorders in out in the subsample of - mood disorders, the Dutch adult explaining impaired WF was reduced by about half, i.e. no independent influence of CMD on N=3104 employees who anxiety disorders general population WF. were present at work at and substance aged 18 to 64 Remarks least partly in the two abuse. years Analyses were adjusted for: gender, age, education, physical illness at baseline, length of periods during which working week at follow-up, score on impaired work functioning at baseline impairments in work functioning were measured
Analyses based on 11- months prevalence between T0 and T1. Prevalence mood disorders (5.2% n=184) Hawthorne et Days limited in Severity disorder: N= 523. Depressed Prime-MD Observational, Type of depression al., 2003 [79] ability to work in Type of depression (Major subgroup of the 1988 South Interview cross-sectional Workers with major depression/or less sever depression were more likely than workers with no last 4 weeks due depression vs. other Australian Health Omnibus depression or less severe depression to have experienced either 3-5 or 6-28 days of limited to health. depression = dysthymia, minor Survey in the general ability to work (as compared to 0 days). depression and partial population. Total group n= Remarks remission of major depression) 3010 ANOVA or Kruskal Wallis (non-parametric test) were used
Major depression N=204 Other depression N= 319 None N=2486 Druss et al., Impact of health Severity disorder: N=1200 met the criteria for 12-item Short-Form Observational, Severity 2001 [68] on effectiveness Recovery (Chronic, incident, depressed symptoms in Health Survey. < longitudinal The odds of decreased effectiveness at work in 1995 was 7.20 higher for workers with chronic at work. 1-item, remitted) 1993; employees from three 43 on mental depressive symptoms, 4.55 higher for incident depressive symptoms, and 1.91 higher for score between major US corporations in component remitted depressive symptoms - all compared to non-depressed workers. 0=unable to 1993-1995. Total Group N= summary; Remarks accomplish 6239 depressive All analyses were adjusted for: age, gender, race, family income, education, number of medical anything symptoms conditions, plan type, and number of years enrolled in the plan. because of Chronic depressive (“clinically health and symptoms (in 1993 and significant”) 100= at best, 1995) N=501 with no health Incident depressive problems, symptoms (in 1995 only) N=652 Remitted depressive symptoms (in 1993 only) N=699
8 No depressive symptoms (in 1993 and 1995) N= 4387 Claassen et Work and Severity disorder N= 4037 17-item Hamilton Cross-sectional Severity al., 2007 [77] Productivity History of suicide attempts Baseline data from the Rating Scale for (baseline) data Patients with prior suicide attempts showed a less work-related productivity in the week prior to Impairment STAR*D trial in outpatients Depression. ≥ 14. from multi-centre enrolment compared to patients without suicide attempt (when adjusted for age, gender, and with MDD treated in primary clinical trial. baseline Hamilton score for depression). and specialty care settings Remarks in US. 58% was employed Analyses were adjusted for: age, gender, and baseline Hamilton score for depression (n=2341). 58% was employed among those without attempted suicide (N=3370), 53.7% was employed among those with attempted suicide (N=667).
Endicott et al. Work Severity disorder: N=35 patients with major DSM-III-R criteria Cross-sectional Severity 1997 [78] Productivity Symptom level depressive disorder at for major (baseline) data The EWPS scores were related to indexes of severity of illness (HAM-D score and Global Index intake; N=42 patients with depressive episode from clinical trial; of Severity, SCL-90 total). major depressive disorder also outcomes at Depressed patients had higher EWPS scores than the community sample did at both intake at endpoint (working endpoint (not and after placebo, although only the intake score was significantly different. patients of psychiatric described). outpatient facility in New York, US.) N=66 community (nonpatient) sample
9 10