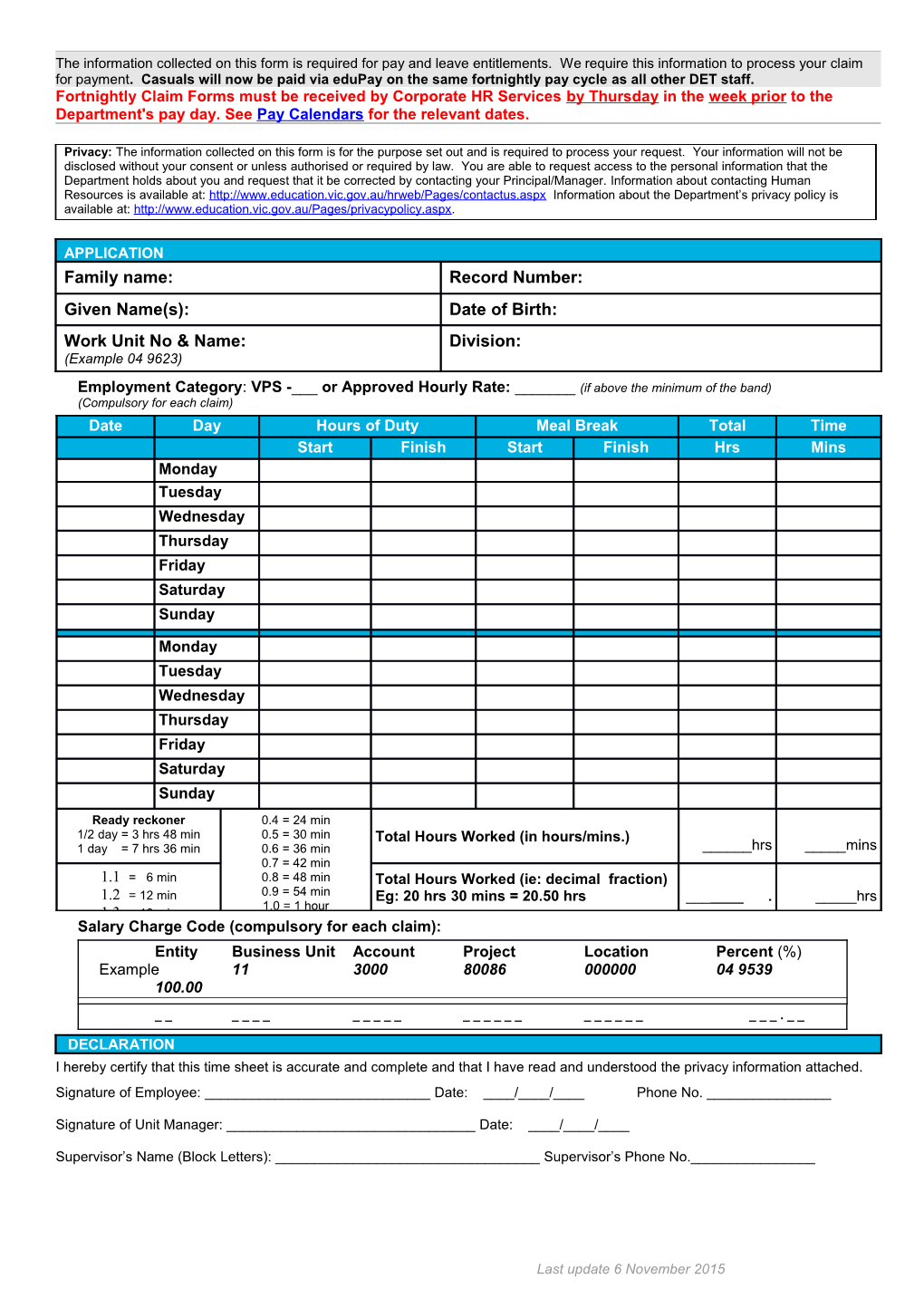
The information collected on this form is required for pay and leave entitlements. We require this information to process your claim for payment. Casuals will now be paid via eduPay on the same fortnightly pay cycle as all other DET staff. Fortnightly Claim Forms must be received by Corporate HR Services by Thursday in the week prior to the Department's pay day. See Pay Calendars for the relevant dates.
Privacy: The information collected on this form is for the purpose set out and is required to process your request. Your information will not be disclosed without your consent or unless authorised or required by law. You are able to request access to the personal information that the Department holds about you and request that it be corrected by contacting your Principal/Manager. Information about contacting Human Resources is available at: http://www.education.vic.gov.au/hrweb/Pages/contactus.aspx Information about the Department’s privacy policy is available at: http://www.education.vic.gov.au/Pages/privacypolicy.aspx.
APPLICATION Family name: Record Number: Given Name(s): Date of Birth: Work Unit No & Name: Division: (Example 04 9623)
Employment Category: VPS -___ or Approved Hourly Rate: ______(if above the minimum of the band) (Compulsory for each claim) Date Day Hours of Duty Meal Break Total Time StartHours of DutyFinish StartMeal BreakFinish Hrs Mins Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Ready reckoner 0.4 = 24 min 1/2 day = 3 hrs 48 min 0.5 = 30 min Total Hours Worked (in hours/mins.) 1 day = 7 hrs 36 min 0.6 = 36 min ______hrs _____mins 0.7 = 42 min 1.1 = 6 min 0.8 = 48 min Total Hours Worked (ie: decimal fraction) 1.2 = 12 min 0.9 = 54 min Eg: 20 hrs 30 mins = 20.50 hrs ______. _____hrs 1.0 = 1 hour 1.3 = 18 min Salary Charge Code (compulsory for each claim): Entity Business Unit Account Project Location Percent (%) Example 11 3000 80086 000000 04 9539 100.00
______. _ _
DECLARATION I hereby certify that this time sheet is accurate and complete and that I have read and understood the privacy information attached. Signature of Employee: ______Date: ____/____/____ Phone No. ______
Signature of Unit Manager: ______Date: ____/____/____
Supervisor’s Name (Block Letters): ______Supervisor’s Phone No.______
Last update 6 November 2015