Everything you need to know about Preferred One For Dental and/or Flex
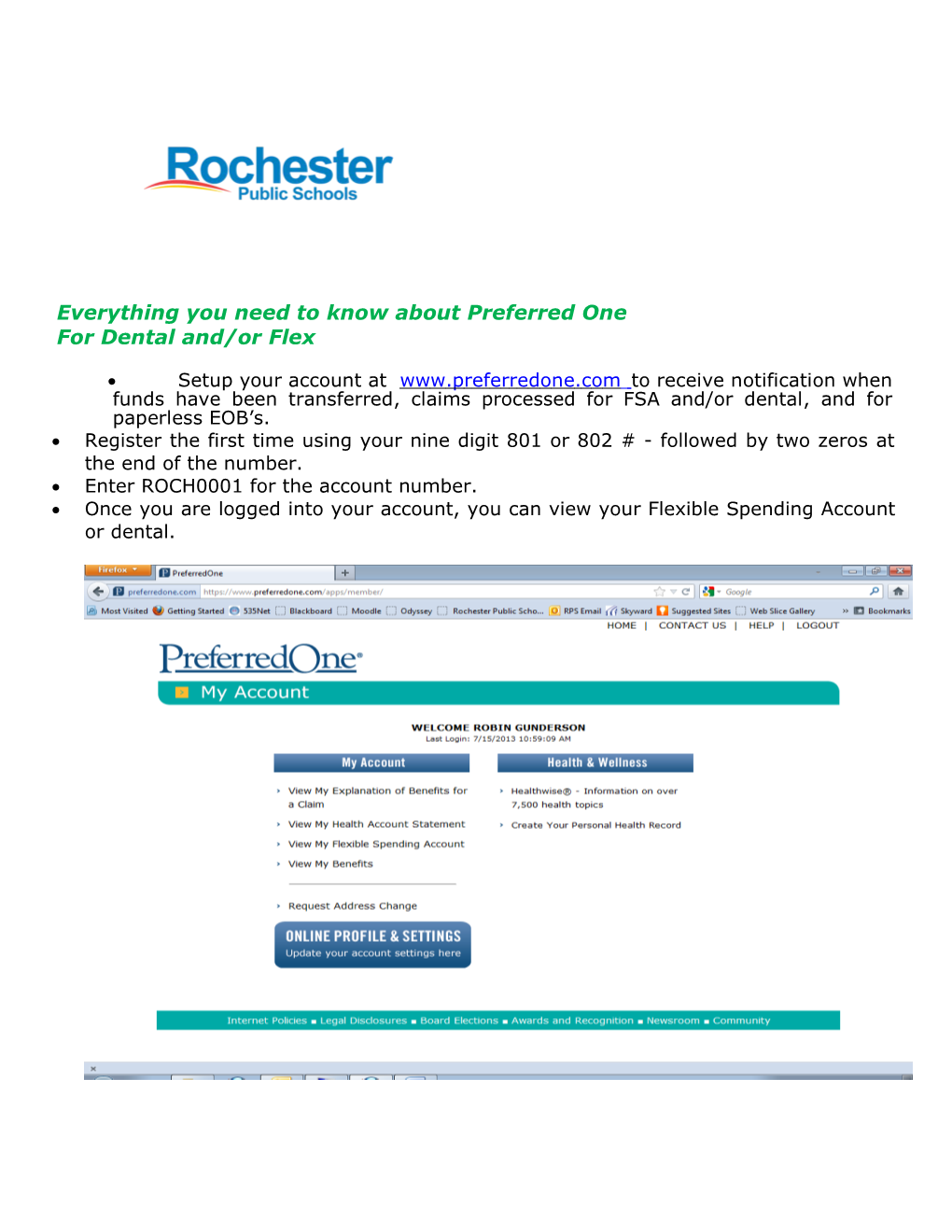
Setup your account at ww w .p r e f e r r e d o n e . c o m to receive notification when funds have been transferred, claims processed for FSA and/or dental, and for paperless EOB’s. Register the first time using your nine digit 801 or 802 # - followed by two zeros at the end of the number. Enter ROCH0001 for the account number. Once you are logged into your account, you can view your Flexible Spending Account or dental.
Go Paperless Paperless Explanation of Benefits - You will need to follow the steps below in order to receive the paperless Explanation of Benefits for Dental and/or Flex. You will be notified by e-mail when you can view your dental or Flex claims. Click – Online Profile & Settings
Select – Change E-Mail Address/EOB Delivery Settings. Please select the first option to receive EOB notifications by e-mail when a claim has been processed. You will receive e-mail from our software vendor - Preferred One. Enter your e-mail address and submit the changes.
Direct Deposit Direct deposit for reimbursement from your Flexible Spending Account is mandatory. If your bank information is not on file with Insurance Services, please fill out the Direct Deposit Form found under the "Forms" button. If you do not have an 80# please call 328-4280. By receiving reimbursements via direct deposit, you will receive your money up to five days faster than waiting for a check to be mailed to your home address. Direct Deposit Enrollment Forms are available on the website at www.rochester.k12.mn.us/insurance. Your bank information stays on file unless you make changes or terminate.
Instructions for Flexible Spending Reimbursement Form Please fill in all employee information including your nine digit subscriber ID - it 80 and is the same as your dental number. begins with Expenses must be incurred in the Plan (calendar) year during your period of coverage. Health FSA Reimbursement Form. You must attach a copy of the Explanation of Benefits reflecting the amount of the expense and the date(s) the expense was incurred (a canceled check or statement is not sufficient). Prescription drugs must include your name, date, and co-pay amounts. Dependent Care Reimbursement Form. Your daycare provider must sign the form. Claims for future services are not eligible for reimbursement and will not be processed.
Submit your claim To be reimbursed you must mail, scan, fax, or email a completed claim form to: Rochester Public Schools District 535 Insurance Services, 10 SE 9 ½ St Rochester, MN 55904 Fax: 507-328-4213 Email: [email protected] Claims with missing or illegible information will be denied, pending re-submission of legible information. Employee must sign and date the form. Claims will be processed within 30 days. All claims must be received by the first or third Tuesday of the month to be eligible for payment by the second or fourth Monday of the month through (EFT) electronic fund transfer. Not all items on the Preferred One website may pertain to your benefits with Rochester Public Schools. Please reference your Summary Plan Document for benefit details at www.rochester.k12.mn.us/insurance o r c a l l 328-4280 .
What must I do to be reimbursed for my Dependent Care Account Plan (DCAP) A DCAP expense is incurred when the service that causes the expense is provided, not when the expense is paid. If you have paid for the expense but the services have not yet been rendered, then the expense has not been incurred. If you prepay on the first day of the month for dependent care that will be given during the rest of the month, then the expense is not incurred until the end of that month and cannot be reimbursed until after the end of that month. When you incur an expense that is eligible for payment, you must submit the Dependent Reimbursement Form. If there is enough money in your DCAP, then you will be reimbursed for your eligible DCAP expenses and the money will be direct deposited into your bank account. You will be reimbursed within 30 days after the date you submitted the Dependent Reimbursement Form. If a claim is for an amount larger than that remaining in your current DCAP balance, then the excess part of the claim will be carried over into the following months.
RPS Insurance Services – Telephone (507) 328-4280 – Fax (507) 328-4213
Updated 01/22/14