Measles & Rubella Case Based Reporting Form
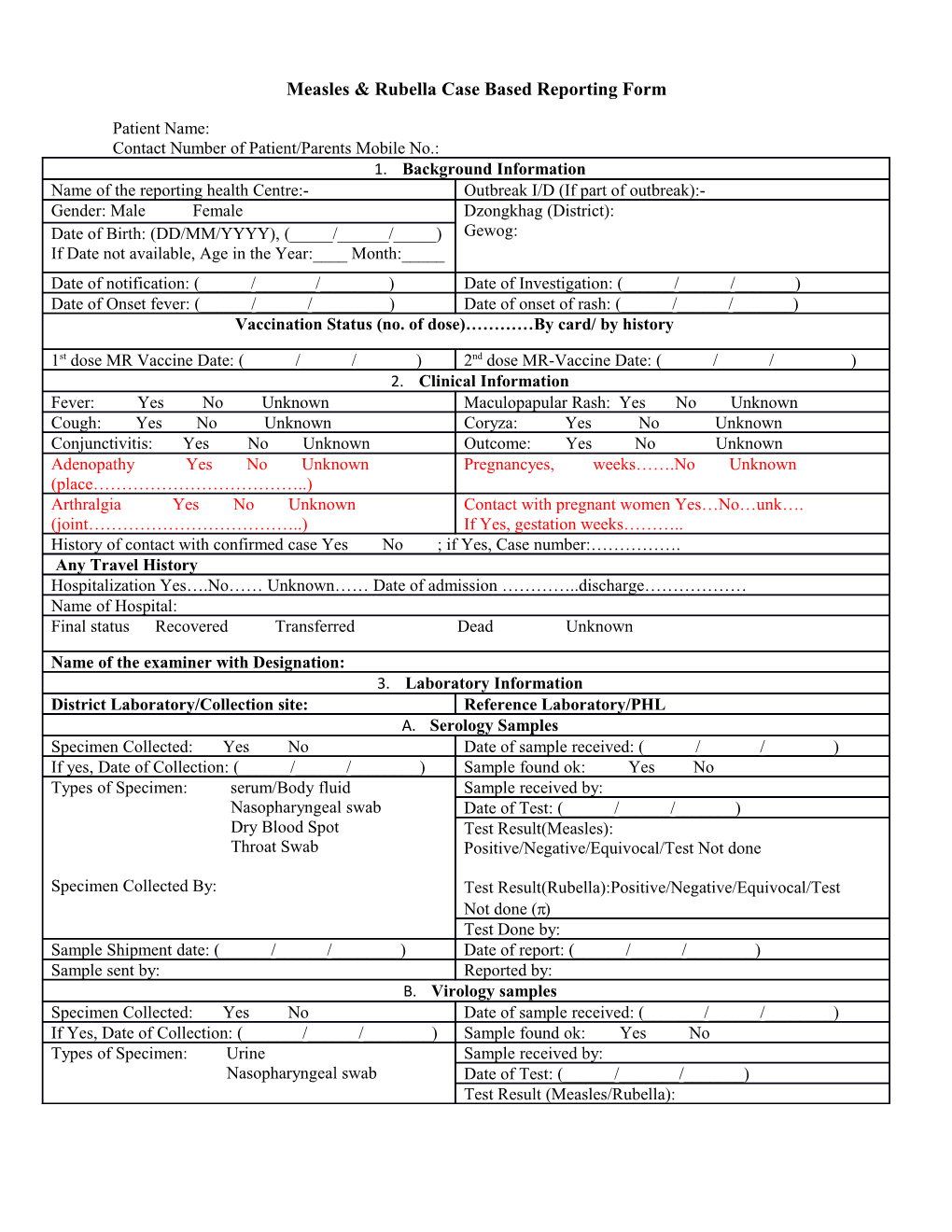
Patient Name: Contact Number of Patient/Parents Mobile No.: 1. Background Information Name of the reporting health Centre:- Outbreak I/D (If part of outbreak):- Gender: Male Female Dzongkhag (District): Date of Birth: (DD/MM/YYYY), (_____/______/_____) Gewog: If Date not available, Age in the Year:____ Month:_____ Date of notification: (______/______/______) Date of Investigation: (______/______/______) Date of Onset fever: (______/______/______) Date of onset of rash: (______/______/______) Vaccination Status (no. of dose)…………By card/ by history
1st dose MR Vaccine Date: (______/______/______) 2nd dose MR-Vaccine Date: (______/______/______) 2. Clinical Information Fever: Yes No Unknown Maculopapular Rash: Yes No Unknown Cough: Yes No Unknown Coryza: Yes No Unknown Conjunctivitis: Yes No Unknown Outcome: Yes No Unknown Adenopathy Yes No Unknown Pregnancyes, weeks…….No Unknown (place………………………………..) Arthralgia Yes No Unknown Contact with pregnant women Yes…No…unk…. (joint………………………………..) If Yes, gestation weeks……….. History of contact with confirmed case Yes No ; if Yes, Case number:……………. Any Travel History Hospitalization Yes….No…… Unknown…… Date of admission …………..discharge……………… Name of Hospital: Final status Recovered Transferred Dead Unknown
Name of the examiner with Designation: 3. Laboratory Information District Laboratory/Collection site: Reference Laboratory/PHL A. Serology Samples Specimen Collected: Yes No Date of sample received: (______/______/______) If yes, Date of Collection: (______/______/______) Sample found ok: Yes No Types of Specimen: serum/Body fluid Sample received by: Nasopharyngeal swab Date of Test: (______/______/______) Dry Blood Spot Test Result(Measles): Throat Swab Positive/Negative/Equivocal/Test Not done
Specimen Collected By: Test Result(Rubella):Positive/Negative/Equivocal/Test Not done () Test Done by: Sample Shipment date: (______/______/______) Date of report: (______/______/______) Sample sent by: Reported by: B. Virology samples Specimen Collected: Yes No Date of sample received: (______/______/______) If Yes, Date of Collection: (______/______/______) Sample found ok: Yes No Types of Specimen: Urine Sample received by: Nasopharyngeal swab Date of Test: (______/______/______) Test Result (Measles/Rubella): Specimen Collected by: Positive/Negative/Equivocal/Test Not done ( )
Test Done by: Sample Shipment date: (______/______/______) Date of report: (______/______/______) Sample sent by: Reported by: (______/______/______) 4. Investigation Active case search from this suspected case done … Yes Cases found in active search Yes, How many?.... No Unknown No….Unknown Travel aboard 7-21 days before the onset of rash, Yes….No…..Unknown.. If Yes, Country name………….. Date travel started DD/MM/YYYY…………………Date travel ended DD/MM/YYYY 5. Classification Final Classification Confirmed Measles Confirmed Rubella Discarded Basis for classification Laboratory Epidemiological Linked Clinical For confirmed cases, Source of infection Imported Import-related Unknown source For discarded, Reason for discarding……………………………………….
Investigator Name Institution Telephone Date