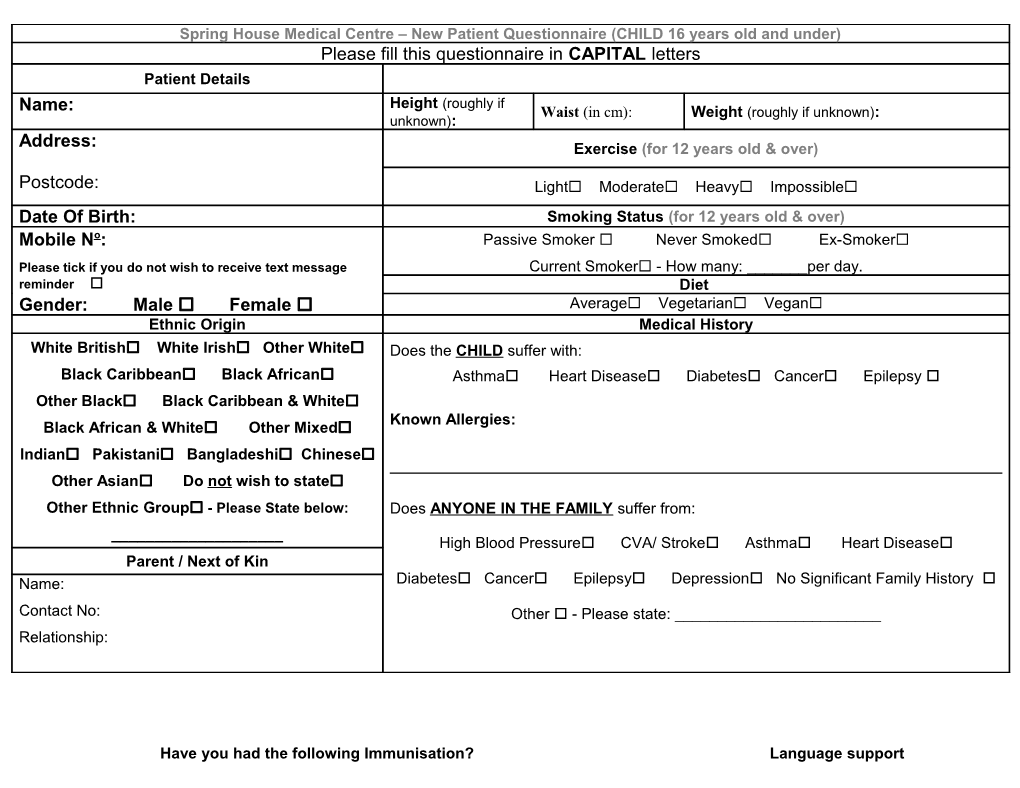
Spring House Medical Centre – New Patient Questionnaire (CHILD 16 years old and under) Please fill this questionnaire in CAPITAL letters Patient Details Height (roughly if Name: Waist (in cm): Weight (roughly if unknown): unknown): Address: Exercise (for 12 years old & over)
Postcode: Light Moderate Heavy Impossible Date Of Birth: Smoking Status (for 12 years old & over) Mobile No: Passive Smoker Never Smoked Ex-Smoker Please tick if you do not wish to receive text message Current Smoker - How many: ______per day. reminder Diet Gender: Male Female Average Vegetarian Vegan Ethnic Origin Medical History White British White Irish Other White Does the CHILD suffer with: Black Caribbean Black African Asthma Heart Disease Diabetes Cancer Epilepsy Other Black Black Caribbean & White Known Allergies: Black African & White Other Mixed Indian Pakistani Bangladeshi Chinese
Other Asian Do not wish to state Other Ethnic Group - Please State below: Does ANYONE IN THE FAMILY suffer from: ______High Blood Pressure CVA/ Stroke Asthma Heart Disease Parent / Next of Kin Name: Diabetes Cancer Epilepsy Depression No Significant Family History Contact No: Other - Please state: ______Relationship:
Have you had the following Immunisation? Language support Please add the date of each immunisation. What is your First Language:______DTP – Diphtheria, Tetanus, Polio Hib Meningitis C Pertussis 2 months Do you speak English:______3 months 4 months
MMR Hob Booster 12-18 months Do you use any of the following: 18 months – 4 years old Sign Language: Yes No
Pre-school Single Hearing aid: Yes No DTP Polio Booster MMR Boosters Meningitis C 3-4 years old Childs School details Diphtheria School Boosters BCG Tetanus Polio booster Name of school: Address:
Others – Please state: Contact number:
Protection Plan Foster care information Religion Christian Buddhist Hindu Is this child subject to a Do you consider the child to be a disabled person? child protection plan? Jewish Muslim Sikh Is this child in: No religion Yes No Foster care Private Foster If Yes, Social Worker Details None of the above No Name: Other – please state: Contact No: Yes - Please specify below: Do not wish to state ______