Tracking #:_____ Capital Requisition Form
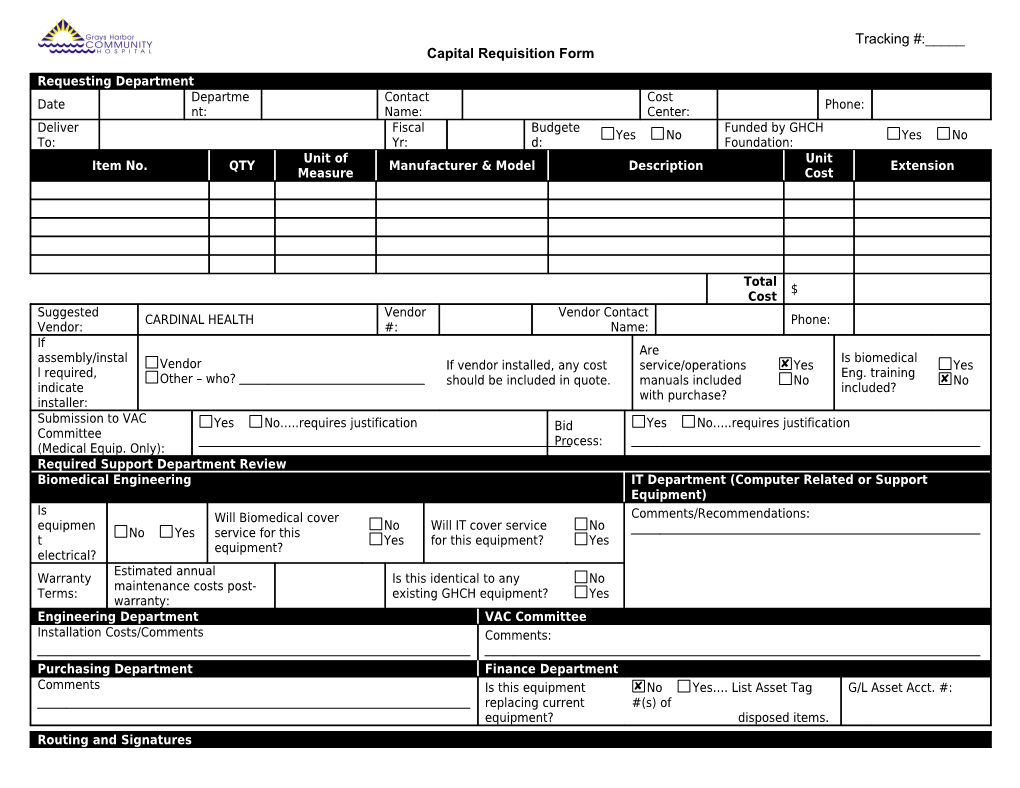
Requesting Department Departme Contact Cost Date Phone: nt: Name: Center: Deliver Fiscal Budgete Funded by GHCH Yes No Yes No To: Yr: d: Foundation: Unit of Unit Item No. QTY Manufacturer & Model Description Extension Measure Cost
Total $ Cost Suggested Vendor Vendor Contact CARDINAL HEALTH Phone: Vendor: #: Name: If Are assembly/instal Is biomedical Vendor If vendor installed, any cost service/operations Yes Yes l required, Eng. training Other – who? should be included in quote. manuals included No No indicate included? with purchase? installer: Submission to VAC Yes No…..requires justification Bid Yes No…..requires justification Committee Process: (Medical Equip. Only): Required Support Department Review Biomedical Engineering IT Department (Computer Related or Support Equipment) Is Will Biomedical cover Comments/Recommendations: equipmen No Will IT cover service No No Yes service for this t Yes for this equipment? Yes equipment? electrical? Estimated annual Warranty Is this identical to any No maintenance costs post- Terms: existing GHCH equipment? Yes warranty: Engineering Department VAC Committee Installation Costs/Comments Comments:
Purchasing Department Finance Department Comments Is this equipment No Yes…. List Asset Tag G/L Asset Acct. #: replacing current #(s) of equipment? disposed items. Routing and Signatures Requested by: Date: Biomedical Eng. Approval: Date: IT Approval: Date:
VAC Approval: Date: Engineering Approval: Date: Supply Chain Operations Date: Approval:
Quality Director Approval: Date: COO Approval: Date: CNO Approval: Date:
Executive Director HR Approval: Date: CFO Approval: Date: CEO Approval: Date:
For Purchasing Use Only Date Quote Review Date PO Buyer: Commen Receive Completed: PO No: Placed: ts: d: Yes