WASHINGTON ASSOCIATION MEDICAL STAFF SERVICES Speaker Expense Reimbursement Report
Name Date Address City, State, Zip Telephone Purpose of trip: Travel To and From:
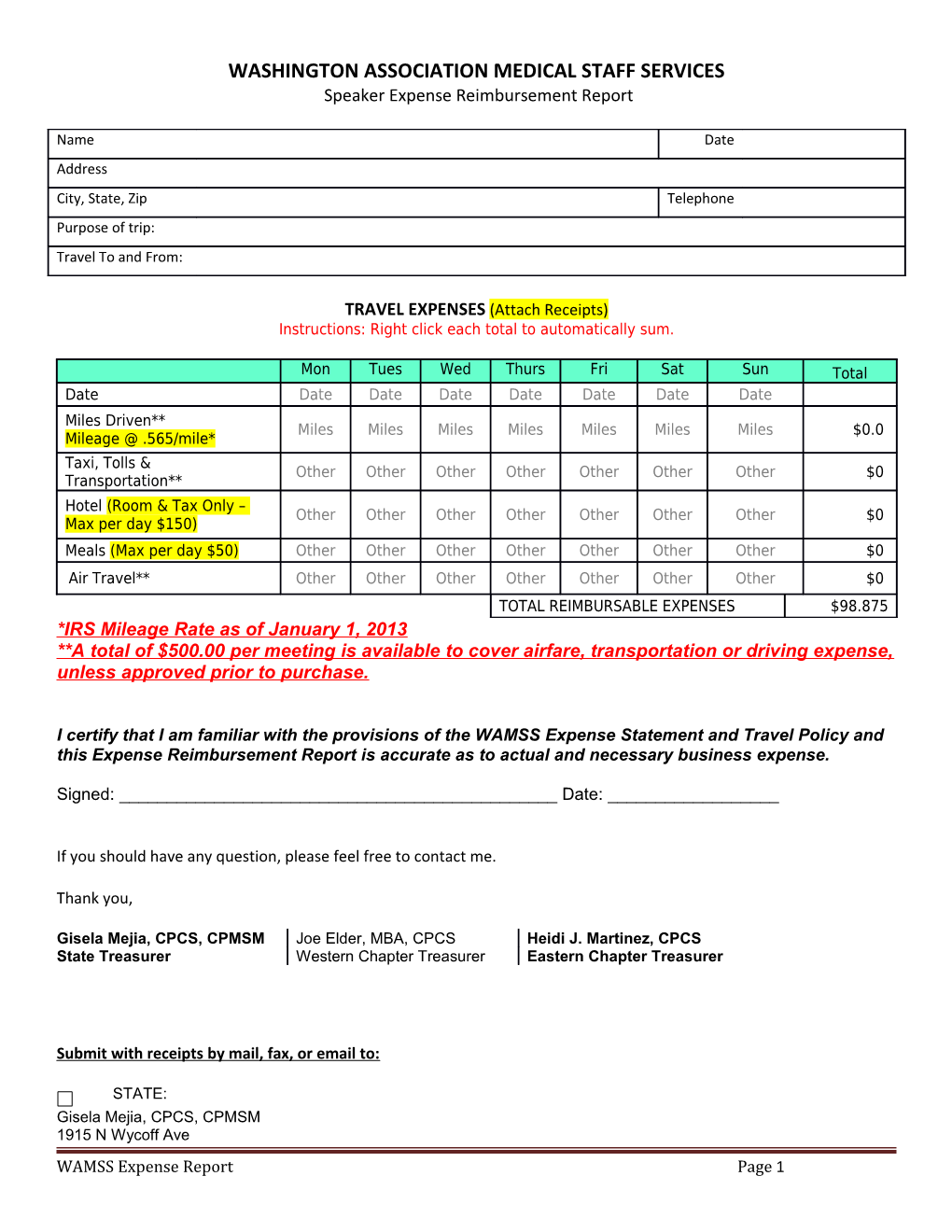
TRAVEL EXPENSES (Attach Receipts) Instructions: Right click each total to automatically sum.
Mon Tues Wed Thurs Fri Sat Sun Total Date Date Date Date Date Date Date Date Miles Driven** Miles Miles Miles Miles Miles Miles Miles $0.0 Mileage @ .565/mile* Taxi, Tolls & Other Other Other Other Other Other Other $0 Transportation** Hotel (Room & Tax Only – Other Other Other Other Other Other Other $0 Max per day $150) Meals (Max per day $50) Other Other Other Other Other Other Other $0 Air Travel** Other Other Other Other Other Other Other $0 TOTAL REIMBURSABLE EXPENSES $98.875 *IRS Mileage Rate as of January 1, 2013 **A total of $500.00 per meeting is available to cover airfare, transportation or driving expense, unless approved prior to purchase.
I certify that I am familiar with the provisions of the WAMSS Expense Statement and Travel Policy and this Expense Reimbursement Report is accurate as to actual and necessary business expense.
Signed: ______Date: ______
If you should have any question, please feel free to contact me.
Thank you,
Gisela Mejia, CPCS, CPMSM Joe Elder, MBA, CPCS Heidi J. Martinez, CPCS State Treasurer Western Chapter Treasurer Eastern Chapter Treasurer
Submit with receipts by mail, fax, or email to:
STATE: Gisela Mejia, CPCS, CPMSM 1915 N Wycoff Ave WAMSS Expense Report Page 1 WASHINGTON ASSOCIATION MEDICAL STAFF SERVICES Speaker Expense Reimbursement Report Bremerton, WA 98310 Phone 360-744-1848 Fax 360-744-8530 [email protected]
WESTERN CHAPTER: EASTERN CHAPTER: Joe Elder, MBA, CPCS Heidi Martinez, CPCS 747 Broadway 1806 W. Lincoln Ave Seattle, WA 98122 Yakima, WA 98902 Direct 206-386-2780 Phone: 509.574.6175 Fax 206-386-3570 Fax: 509-457-3989 [email protected] [email protected]
FOR OFFICE USE ONLY
Check # ______Date Paid : ______Account(s): ______
WAMSS Expense Report Page 2