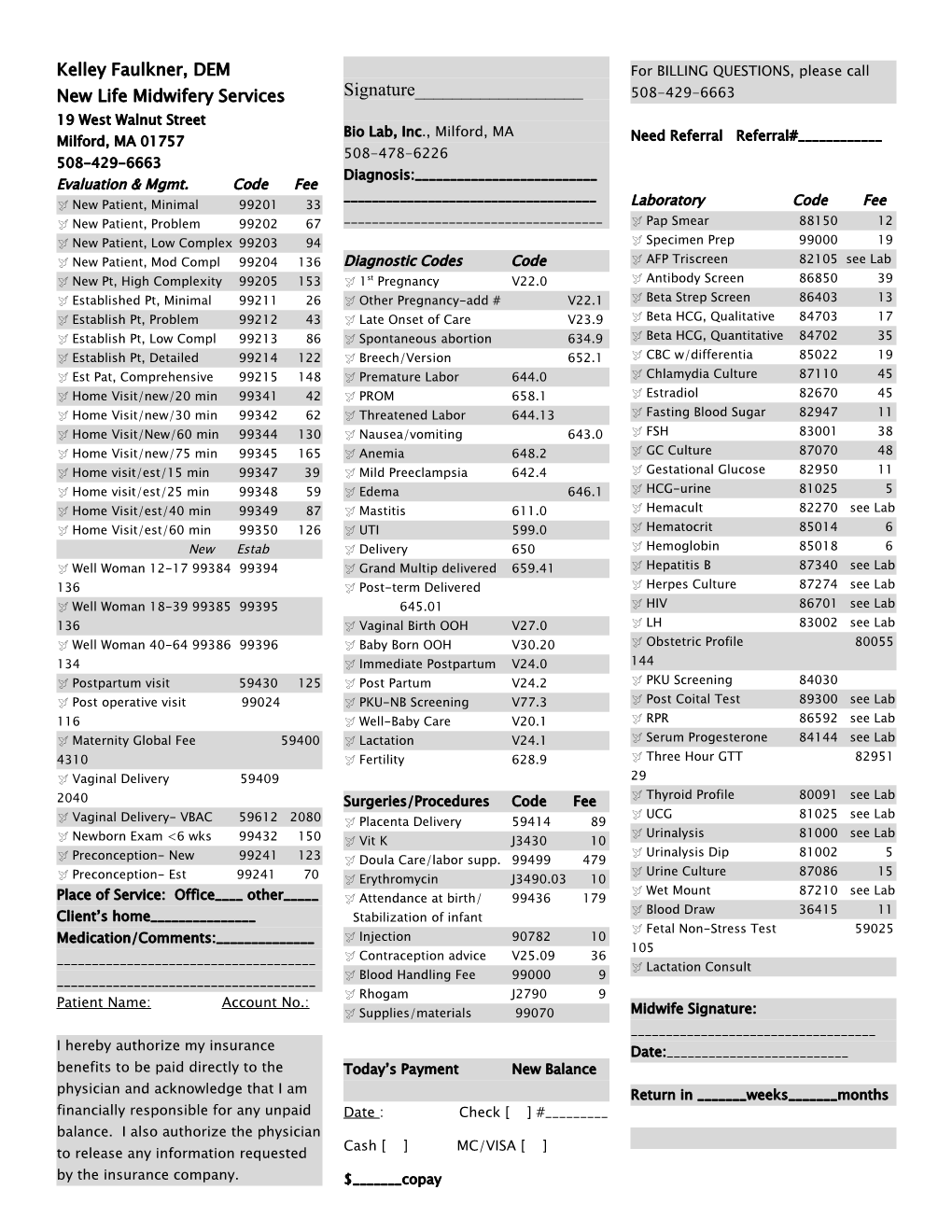
Kelley Faulkner, DEM For BILLING QUESTIONS, please call Signature______New Life Midwifery Services 508-429-6663 19 West Walnut Street Bio Lab, Inc., Milford, MA Milford, MA 01757 Need Referral Referral#______508-478-6226 508-429-6663 Diagnosis:______Evaluation & Mgmt. Code Fee ______ New Patient, Minimal 99201 33 Laboratory Code Fee New Patient, Problem 99202 67 ______Pap Smear 88150 12 New Patient, Low Complex 99203 94 Specimen Prep 99000 19 New Patient, Mod Compl 99204 136 Diagnostic Codes Code AFP Triscreen 82105 see Lab st New Pt, High Complexity 99205 153 1 Pregnancy V22.0 Antibody Screen 86850 39 Established Pt, Minimal 99211 26 Other Pregnancy-add # V22.1 Beta Strep Screen 86403 13 Establish Pt, Problem 99212 43 Late Onset of Care V23.9 Beta HCG, Qualitative 84703 17 Establish Pt, Low Compl 99213 86 Spontaneous abortion 634.9 Beta HCG, Quantitative 84702 35 Establish Pt, Detailed 99214 122 Breech/Version 652.1 CBC w/differentia 85022 19 Est Pat, Comprehensive 99215 148 Premature Labor 644.0 Chlamydia Culture 87110 45 Home Visit/new/20 min 99341 42 PROM 658.1 Estradiol 82670 45 Home Visit/new/30 min 99342 62 Threatened Labor 644.13 Fasting Blood Sugar 82947 11 Home Visit/New/60 min 99344 130 Nausea/vomiting 643.0 FSH 83001 38 Home Visit/new/75 min 99345 165 Anemia 648.2 GC Culture 87070 48 Home visit/est/15 min 99347 39 Mild Preeclampsia 642.4 Gestational Glucose 82950 11 Home visit/est/25 min 99348 59 Edema 646.1 HCG-urine 81025 5 Home Visit/est/40 min 99349 87 Mastitis 611.0 Hemacult 82270 see Lab Home Visit/est/60 min 99350 126 UTI 599.0 Hematocrit 85014 6 New Estab Delivery 650 Hemoglobin 85018 6 Well Woman 12-17 99384 99394 Grand Multip delivered 659.41 Hepatitis B 87340 see Lab 136 Post-term Delivered Herpes Culture 87274 see Lab Well Woman 18-39 99385 99395 645.01 HIV 86701 see Lab 136 Vaginal Birth OOH V27.0 LH 83002 see Lab Well Woman 40-64 99386 99396 Baby Born OOH V30.20 Obstetric Profile 80055 134 Immediate Postpartum V24.0 144 Postpartum visit 59430 125 Post Partum V24.2 PKU Screening 84030 Post operative visit 99024 PKU-NB Screening V77.3 Post Coital Test 89300 see Lab 116 Well-Baby Care V20.1 RPR 86592 see Lab Maternity Global Fee 59400 Lactation V24.1 Serum Progesterone 84144 see Lab 4310 Fertility 628.9 Three Hour GTT 82951 Vaginal Delivery 59409 29 Thyroid Profile 80091 see Lab 2040 Surgeries/Procedures Code Fee UCG 81025 see Lab Vaginal Delivery- VBAC 59612 2080 Placenta Delivery 59414 89 Urinalysis 81000 see Lab Newborn Exam <6 wks 99432 150 Vit K J3430 10 Urinalysis Dip 81002 5 Preconception- New 99241 123 Doula Care/labor supp. 99499 479 Urine Culture 87086 15 Preconception- Est 99241 70 Erythromycin J3490.03 10 Wet Mount 87210 see Lab Place of Service: Office____ other_____ Attendance at birth/ 99436 179 Blood Draw 36415 11 Client’s home______Stabilization of infant Fetal Non-Stress Test 59025 Medication/Comments:______ Injection 90782 10 105 Contraception advice V25.09 36 ______ Lactation Consult ______Blood Handling Fee 99000 9 Rhogam J2790 9 Patient Name: Account No.: Supplies/materials 99070 Midwife Signature: ______I hereby authorize my insurance Date:______benefits to be paid directly to the Today’s Payment New Balance physician and acknowledge that I am Return in ______weeks______months financially responsible for any unpaid Date : Check [ ] #______balance. I also authorize the physician Cash [ ] MC/VISA [ ] to release any information requested by the insurance company. $______copay Next Appointment______, 200__ At ______AM/PM
Birthwithlove Midwifery Services
Total Page:16
File Type:pdf, Size:1020Kb
Recommended publications