Title: Telotristat etiprate: a new option for the management of carcinoid syndrome
Authors: Angela Lamarca1,*, Jorge Barriuso1,2, Mairéad G McNamara1,3, Richard A Hubner1, Juan W Valle1,3
1 Department of Medical Oncology, The Christie NHS Foundation Trust, Manchester, United Kingdom.
2 Faculty of Medical, Biological and Human Sciences, University of Manchester, Manchester, United Kingdom.
3 Institute of Cancer Sciences, University of Manchester, Manchester, United Kingdom.
*Part-funded by SEOM (Spanish Society of Medical Oncology) Translational Fellowship Program.
Corresponding author:
Professor Juan W Valle, Department of Medical Oncology, The Christie NHS Foundation Trust, Wilmslow Road, Manchester, M20 4BX, UK. Phone: +44 161-446-8106; Fax +44 161-446-3468
Conflict of Interest
Authors have no conflict of interest related to this manuscript. A Lamarca and J Barriuso are part-funded by SEOM (Spanish Society of Medical Oncology) Translational Fellowship Grants.
JW Valle has received Honoraria and a Travel Grant from Ipsen.
Keywords:
Bowel movement, Carcinoid syndrome, diarrhoea, flushing, LX1606, neuroendocrine tumours, serotonin synthesis inhibitor, telotristat ethyl, tryptophan hydroxylase 1 (Tph1)
1 Abstract
Introduction: Many patients with neuroendocrine tumour-related carcinoid syndrome treated with somatostatin analogues (SSA) won’t achieve adequate symptom relief with the SSA alone; new treatment options are required. Telotristat ethyl is a tryptophan hydroxylase inhibitor, developed for the treatment of carcinoid syndrome.
Areas covered: This review summarises the evidence supporting the role of telotristat ethyl in the management of carcinoid syndrome. Rationale, pharmacodynamics, pharmacokinetics, metabolism, clinical experience, efficacy and toxicity profiles are covered.
Expert opinion: The efficacy of telotristat ethyl in producing a statistically-significant and clinically- meaningful reduction in daily bowel movements has been confirmed in phase III clinical trials. Two pivotal trials, TELESTAR and TELECAST, explored the role of telotristat ethyl in the management of patients with carcinoid syndrome refractory to SSAs focusing on patients with ≥4 and <4 daily bowel movements, respectively. In addition, benefit was confirmed in patient-reported outcomes. Based on activity and safe toxicity profile, telotristat ethyl is pending regulatory agencies evaluation and is likely to add to the armamentarium used to treat carcinoid syndrome. Long-term safety and efficacy data will be available from the ongoing TELEPATH study. The impact on carcinoid heart disease, mesenteric fibrosis and other long-term complications of carcinoid syndrome as well as its role earlier in patients’ pathways remain investigational.
2 Contents 2. List of abbreviations...... 4 3. Introduction...... 5 4. Market overview: carcinoid syndrome, an area of unmet need...... 6 5. Introduction to telotristat ethyl (LX1032/LX1606)...... 7 5.1 Mechanism of action...... 7 5.2 Chemistry...... 7 5.3 Pharmacodynamics...... 7 5.4 Pharmacokinetics and metabolism...... 8 6. Clinical efficacy...... 8 6.1 Phase I studies...... 8 6.2 Phase II studies...... 9 6.3 Phase III studies...... 10 7. Patient-reported outcomes...... 11 8. Safety and tolerability...... 11 9. Regulatory affairs...... 12 10. Conclusion...... 12 11. Expert opinion...... 13 12. Drug summary box...... 13 13. References...... 15 14. Figures and Tables...... 22 15. Declaration of Interest...... 31
3 1. List of abbreviations
14C-LX1606: 14C-labelled telotristat ethyl
5-HIAA: 5-hydroxyindoleacetic acid
95%CI: 95% confidence interval
AADC: aromatic amino acid decarboxylase
GI-NET: gastrointestinal neuroendocrine tumour
HR: hazard ratio
IC50: 50% inhibitory concentrations
IFN: interferon
LAR: long acting release
NET: neuroendocrine tumour
PFS: progression-free survival
PRRT: peptide receptor radionuclide therapy
QWBA: quantitative whole-body autoradiography
SSA: somatostatin analogue
T1/2: half life tid: three times a day
Tmax: time to maximum concentration (Cmax)
TPH: tryptophan hydroxylase
TPH1: tryptophan hydroxylase 1
TPH 2: tryptophan hydroxylase 2
Wd-NETs: well-differentiated neuroendocrine tumours
4 2. Introduction Despite the increasing incidence of neuroendocrine tumours (NET), in part due to increased awareness, they are still considered rare malignancies [1]. Neuroendocrine tumours are classified according to morphology and proliferation index [2;3] into well- or poorly-differentiated neoplasms. Well-differentiated NETs (Wd-NETs, which may be sub-divided into grade (G)1 or G2 tumours) may, in some specific circumstances present with systemic symptoms related to hormone secretion (functional tumours) (20-30%), the most frequent one being carcinoid syndrome [4]. It is not usual for poorly-differentiated (G3) carcinomas to exhibit this syndrome.
Carcinoid syndrome
Carcinoid syndrome covers a spectrum of symptoms such as diarrhoea, flushing, wheezing and valvular heart disease and appears typically in the presence of liver metastases [5]. Carcinoid syndrome most frequently develops in patients with Wd-NETs originating in the small bowel (GI- NETs) (affecting 40% of patients with Wd GI-NETs [6]) it may also develop on a background of NETs from other primary sites (e.g. 5-10% of patients with lung NETs [7]). Carcinoid syndrome is a reflection of an alteration of tryptophan metabolism, resulting in an elevation of serum serotonin levels and its urinary metabolite: 5-hydroxyindoleacetic acid (5-HIAA) [8], however other peptides have also been described to be involved in the development of such symptoms, such as substance P, bradykinin, histamine and tachykinins (such as neurokinin A, neurokinin B, neuropeptide K, eledoisin) [9-12]. Carcinoid syndrome symptoms may be triggered by specific foods (such as chocolate or cheese), alcohol, and emotional events amongst other triggers. Carcinoid crisis is an acute life- threatening manifestation of carcinoid syndrome, associated with wide blood pressure fluctuations with a predominance of hypotension, and may be triggered by tumour manipulation, e.g. during surgery or anaesthesia [13].
Due to the slow growth of GI-NETs, patients are likely to live many years (with a median between 2 and 5 years) even if diagnosed in advanced stages [1]. Hence, maintenance of quality of life through good symptom control is one of the cornerstones of management, especially in patients with carcinoid syndrome which is likely to interfere with daily activities (i.e. frequent, troublesome diarrhoea associated with urgency, incontinence and night-time episodes) if treated sub-optimally [14].
Current options for systemic therapy of carcinoid syndrome
There are two main approaches in the management of carcinoid syndrome: direct inhibition of hormonal secretion; and control of tumour burden, thereby reducing the disease volume accountable for hormonal production (Table 1). The first approach, historically represented by the use of short- and long-acting somatostatin analogues (SSAs), achieves rapid symptom relief [6;15-22]. In contrast, approaches aimed at controlling tumour growth (or “debulking”) such as chemotherapy [23], interferon (IFN) [24], peptide receptor radionuclide therapy (PRRT) [25] or liver-directed therapies [26;27],
5 provide a more delayed mode of action in symptom control of carcinoid syndrome (with the possible exception of liver-directed therapies).
3. Market overview: carcinoid syndrome, an area of unmet need Currently, SSAs such as depot octreotide and lanreotide injections are considered the first-line treatment options for the management of carcinoid syndrome in patients when rapid symptom control is required [28]. In addition to control of hormone-secretion [28;29], SSAs have been shown to also control tumour growth evident by improved progression-free survival in phase III trials [6;15;30] (Table 1).
Around 40% and 5-10% of patients diagnosed with Wd-NETs originating from the small bowel [6] or lung [7], respectively, are expected to have a degree of carcinoid syndrome. Of these, 80% will have diarrhoea as a feature [50]; diarrhoea has been classified as moderate / extreme in around 35% of patients in retrospective studies assessing patient-reported symptoms and quality of life [51]. Although SSAs achieve a reasonably high rate of clinical benefit in patients with carcinoid syndrome (in terms of control of symptoms associated with the syndrome), up to 20% of patients fail to have a satisfactory response [18;20] (Table 2) and this percentage increases up to 50% when patients with “highly- functional” carcinoid syndrome are selected [17]. Therefore, even though SSAs have been considered the standard of care for the control of carcinoid syndrome for decades, there is room for improvement, mainly in such patients with highly-functional syndrome.
Due to the significant prevalence of diarrhoea in patients with carcinoid syndrome, interest has primarily focused on carcinoid-related diarrhoea, and clinical trials have been designed with improvement in this symptom as a primary end-point. However, it is important to note that a number of other features of carcinoid syndrome also need to be assessed and treated depending on individual patients. These include other serotonin- (and other mediator-) related symptoms (such flushing and wheezing) as well as long-term desmoplastic complications including carcinoid heart disease [52;53] and mesenteric fibrosis [54-56].
Unfortunately, alternatives to SSAs are lacking: the use of high-dose SSAs (above recommended treatment dose) have been explored [32;59-63]. A recent meta-analysis reviewed the evidence for high-dose octreotide (doses ranging from 40 mg every 4 weeks or 30 mg every 3 weeks up to 120 mg every 4 weeks) in patients with NETs. This meta-analysis included 17 studies and a mixture of patients, including patients on SSA due to carcinoid syndrome, but also patients in whom the SSA was given for tumour-control purposes only. Results suggested that increased doses may be effective for symptom control, however further prospective evaluation of safety and efficacy is required [64]. Other alternatives include the addition of IFN [65], or to try a therapeutic switch SSA (octreotide to lanreotide or vice versa) [29].
None of the above strategies has confirmed clinically-meaningful activity and therefore, refractory carcinoid syndrome despite currently-available supportive measures remains an area of unmet need.
6 The development of treatments targeting serotonin production, such as telotristat ethyl, aims to meet this need.
4. Introduction to telotristat ethyl (LX1032/LX1606) Carcinoid syndrome is the clinical manifestation of high levels of serotonin, which plays a critical role in regulating several major physiological processes of the gastrointestinal tract, including secretion, motility and inflammation. Other peptides may also be involved, such as substance P, bradykinin, histamine and tachykinins. Telotristat ethyl is a tryptophan hydroxylase (TPH) inhibitor which results in a reduction in serotonin production (measured as urine reduction of the serotonin metabolite, 5-HIAA) and has shown activity in controlling carcinoid syndrome refractory to SSAs.
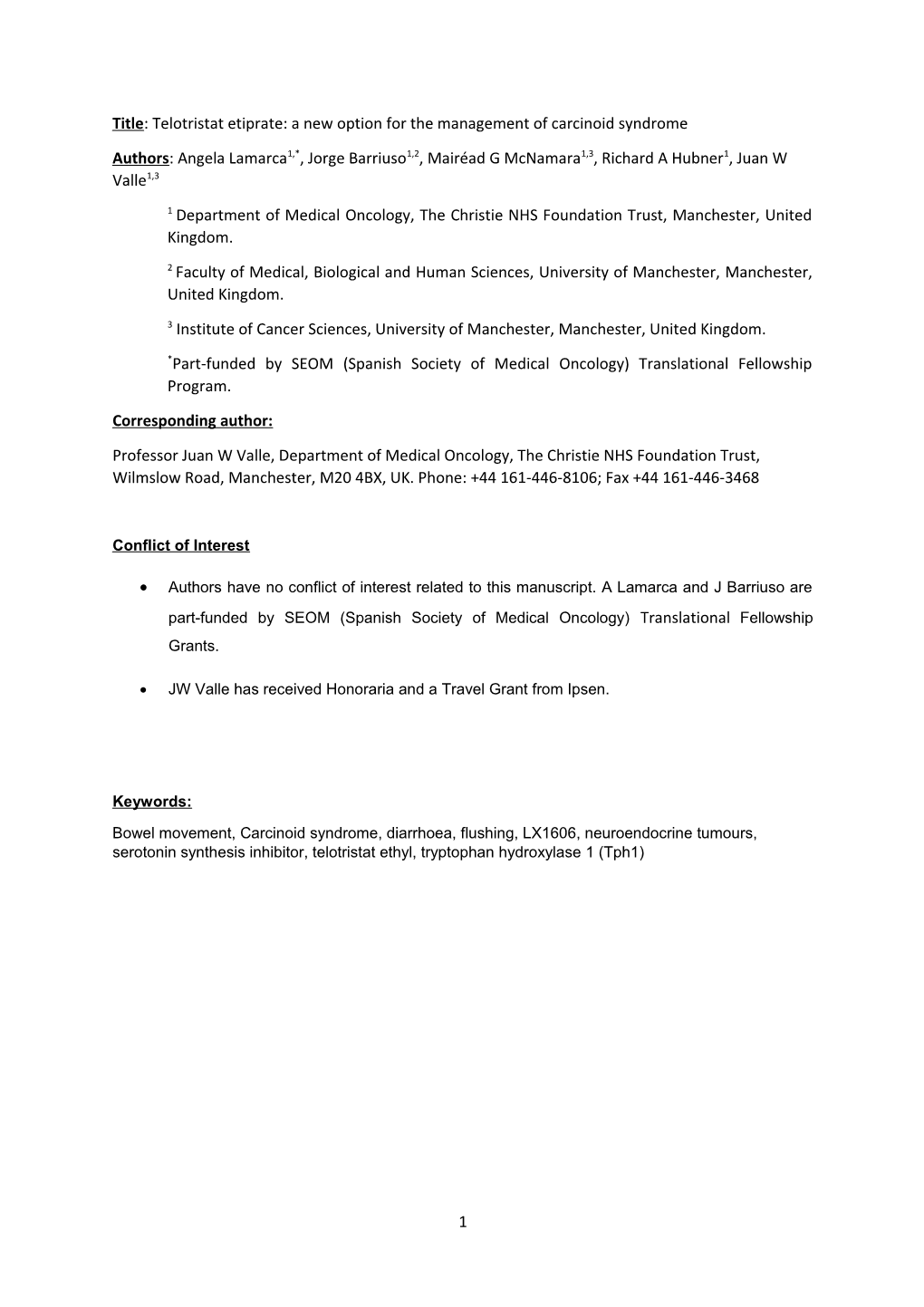
5.1 Mechanism of action Serotonin is synthesised from L-tryptophan by the sequential action of two enzymes: TPH and aromatic amino acid decarboxylase (AADC) (Figure 1b), with TPH being the rate-limiting enzyme in the pathway. By inhibition of TPH, telotristat ethyl reduces production of serotonin [66;67], improving carcinoid syndrome-related symptoms [68].
Tryptophan hydroxylase is encoded by two genes: TPH1 (expressed in the pineal gland and the enterochromaffin cells of the gastrointestinal tract) and TPH2 (expressed in neurons of the raphe nuclei and of the myenteric plexus) [69]. This organ-specific expression accounts for the distribution of serotonin in humans in both the gastrointestinal tract (90% of the total) and the central nervous system (10%) [70].
5.2 Chemistry Telotristat ethyl is an ethyl ester prodrug (Figure 1a). The drug substance salt form is telotristat etiprate (LX1606 hippurate), which is an orally-delivered small molecule with high molecular weight (754.1 g/mol) [72]. Telotristat ethyl is supplied in a white coated oval tablet formulation containing 250 mg of LX1606, known to have long-term stability and can be stored at room temperature [71]. Although the name “telotristat etiprate” was previously used in the literature, recent guidance from the US Food and Drug Administration recommends using the name of the neutral form “telotristat ethyl” rather than the salt “telotristat etiprate”; hence, telotristat ethyl is used.
5.3 Pharmacodynamics Following administration, telotristat ethyl is rapidly hydrolysed to its active form: telotristat (LP- 778902), which blocks the activity of TPH. In vitro assessments of LP-778902 have shown preferential activity against TPH1 and it is considered a selective [67;73] and potent inhibitor of TPH1 with an in vivo IC50 (50% inhibitory concentrations) of 0.028 µM [71].
In vivo activity of telotristat ethyl was evaluated by determining levels of serotonin in mice, rats, dogs and monkeys after drug administration [66;73]. In an in vivo study where telotristat ethyl was used to treat animal models of intestinal inflammation, telotristat ethyl showed a significant reduction in serum
7 serotonin after 4-5 days of treatment, with a subsequent impact on gastrointestinal motility and generation of immune responses [66]. In humans, reduction in blood serotonin and urinary 5-HIAA levels of 25-40% were achieved following 2 weeks of treatment with oral telotristat ethyl at a dose of 500 mg administered three times a day (tid) [71].
Both telotristat ethyl and LP-778902 have not shown significant cross-reactivity when analysed against 75 pharmacologically-relevant receptors, enzymes, and ion channels. In addition, its effect in the brain and cardiovascular system seems to be minimal, with an excellent safety profile [67;71].
5.4 Pharmacokinetics and metabolism
In all species studied, circulating levels of telotristat ethyl are extremely low compared to those of LP- 778902 due to rapid hydrolysis of telotristat ethyl into LP-778902 [71]. In humans, the median time to maximum concentration in blood (Tmax) ranged between 2-4 hours, with a half-life (T1/2) between 4 and 12 hours, consistent with the proposed 8-hourly administration [74]. There was no accumulation of LP-778902 with multiple dose administration over 14 days.
A quantitative whole-body autoradiography (QWBA) study performed in rats showed a predominant distribution of 14C-labelled telotristat ethyl (14C-LX1606) within the gastrointestinal tract, with limited distribution in the hepatic and renal systems; no brain distribution was identified. In the first 24 hours following administration, 14C-LX1606-derived radioactivity was excreted following oral administration, mainly through faeces due to liver metabolism (90%), and minimally through the urine (<10%) [71]. The safety of telotristat ethyl in patients with mild, moderate and severe hepatic insufficiency is currently been explored in an ongoing clinical trial (NCT02683577) [75].
5. Clinical efficacy Telotristat ethyl has demonstrated a reduction in serotonin production when administered to healthy volunteers [74]. Moreover, it has shown activity in controlling carcinoid syndrome-associated diarrhoea in two recently published phase II clinical trials [74;76], and efficacy has been confirmed in phase III clinical trials [77-79]. Clinically-significant reduction in bowel movements has been explored in these studies focused which included patient-reported outcomes; these are summarised later in this review.
6.1 Phase I studies Multiple phase I studies have assessed the pharmacokinetics of telotristat ethyl when administered to humans (NCT01932528) [71;75], including food-effect studies (NCT02157584) [75]. These phase I studies reported that telotristat ethyl was well tolerated up to a total daily dose of 1500 mg (500 mg tid) in healthy subjects when administered with food for 14 days, with no evidence of dose-limiting toxicity [71;80]. No change in QT-interval has been identified in phase I studies (NCT02155205) [75]. Additional studies have analysed potential interactions between telotristat ethyl and octreotide injections (NCT02195635) [75], midazolam (NCT02147808), [75] and fexofenadine (NCT02157558)
8 [75]. Most adverse events were mild, the most common being nausea; no severe adverse events were observed (Table 3).
6.2 Phase II studies Two phase II studies assessing the use of telotristat ethyl in patients with carcinoid syndrome have been reported [74;76].
The first phase II clinical trial was completed in 2012 by Pavel et al [76]. This single-arm multicentre clinical trial recruited 15 patients with carcinoid syndrome (defined as baseline of ≥4 daily bowel movements). Recruited patients were required to have good performance status (Karnofsky Performance Status ≥70), and biopsy-proven Wd-NET. Patients received oral telotristat ethyl at 150 mg tid for 2 weeks. Following the first 2 weeks of treatment, the dose was escalated to 250 mg tid for 2 weeks, followed by 350 mg tid for 2 weeks, then 500 mg tid for 2 weeks. Once the highest tolerated dose was achieved, patients continued treatment until week 12 from study entry. Out of the 15 enrolled patients, 14 completed the treatment period and 13 received a concomitant SSA (median duration of previous SSA therapy was 28 months (range 3-87)). Eighty percent of patients were escalated to the maximum dose of 500 mg tid with no dose-limiting toxicities; hence, this dose was the recommended dose for future clinical trials. All patients experienced reductions in daily bowel movements with an overall mean reduction of 43.5% compared to baseline (mean reduction of 2.6 daily bowel movements; p-value <0.001). Treatment with telotristat ethyl resulted in a reduction of urinary 5-HIAA of 74.2% (p-value <0.05); and the degree of 5-HIAA reduction correlated with reduction in bowel movements. Nine patients (75%) reported “adequate relief” of gastrointestinal symptoms at 12 weeks. Benefit was also shown in stool formation (19.5% reduction in the stool form scale compared to baseline; p-value <0.05)) and flushing (reduction of 27% on number of episodes per day compared to baseline; p-value 0.04)). The type of concomitant SSA did not affect the efficacy of telotristat ethyl.
A second phase II clinical trial by Kulke et al completed recruitment in 2014 [74]. Twenty-three patients were included in this randomised, double-blind, placebo-controlled, dose-escalating study which explored the use of telotristat ethyl in patients with refractory carcinoid syndrome (defined as baseline of ≥4 daily bowel movements despite SSA). Patients received an incremental dose of telotristat ethyl or matching placebo together with a stable-dose of long-acting SSA. The study was performed in two steps; the first step randomised 16 patients between telotristat ethyl or placebo (in a 3:1 ratio) assigning patients into 4 sequential cohorts evaluating the following daily doses: 150, 250, 350, or 500 mg tid over a 4-week course. The dose of 500 mg tid was identified as the dose for the expansion cohort. The second step included an expansion cohort of 7 patients randomised at a 3:1 ratio to telotristat ethyl or placebo. Clinical and biochemical response was defined as a minimum reduction of 30% in daily bowel movements for a minimum of 2 weeks or a reduction of at least 50% of urinary 5-HIAA, respectively. Clinical and biochemical responses were achieved in 28% and 56% of patients who received telotristat ethyl, respectively. No patients in the placebo arm experienced either
9 clinical or biochemical response. In addition, 46% of patients treated with telotristat ethyl had adequate relief after 4 weeks of treatment, compared to no patients in the placebo arm.
6.3 Phase III studies Three phase III clinical trials are exploring the role of telotristat ethyl in patients with carcinoid syndrome refractory to SSA. The TELESTAR clinical trial (NCT01677910, [75]) recruited patients with highly-functional carcinoid syndrome (defined as a baseline of ≥4 daily bowel movements) refractory to SSA; whereas the TELECAST trial (NCT02063659) [75] recruited patients with non-highly functional carcinoid syndrome (baseline of <4 daily bowel movements or flushing or abdominal pain as dominant symptom). The third phase III study, TELEPATH (NCT02026063) [75], is an open-label extension study of telotristat ethyl following completion of the study period in either the TELESTAR or TELECAST trials, with the aim of evaluating the long-term safety and tolerability of oral telotristat ethyl. Although all trials have completed recruitment, only data from the TELESTAR [77;81] and TELECAST [78] studies have been reported. Figure 2 summarises the trial design of these two main phase III studies, TELESTAR and TELECAST.
The TELESTAR study was designed as a three-arm randomised phase III study evaluating two doses of oral telotristat ethyl (250 mg tid or 500 mg tid) compared to matching placebo over a 12-week period. Patients were randomised in a 1:1:1 ratio. Following the 1-week dose titration period, followed by 12 weeks at the allocated dose of telotristat (placebo, 250 mg tid or 500 mg tid), telotristat ethyl was increased to 500 mg tid for all patients and treatment continued up to a 36-week open-label extension period. The primary end-point of this study was to assess the effect of telotristat ethyl on daily bowel moments at 12 weeks from randomisation.
A total of 135 patients were randomised in TELESTAR [77]; 45 patients to each arm. The study met its primary end-point: patients in both telotristat ethyl arms showed an improvement in diarrhoea compared to placebo at week 12 (p<0.001). At week 12, the highest reduction in bowel movement frequency was achieved in the arm treated with highest dose of telotristat ethyl: 17%, 29%, and 35% on placebo, 250 mg and 500 mg tid arms, respectively. The telotristat ethyl-treated patients had durable clinical responses (defined as ≥30% reduction in bowel movements for ≥50%of the double blind-study period (12 weeks)): 44% and 42% for 250 mg and 500 mg tid arms, respectively, compared to placebo (20%) (p-value <0.04 for both treatment arms compared to placebo), together with significant biochemical responses (p-value<0.001 for both treatment arms compared to placebo). However it is worth highlighting that the trial was not powered to assess other symptoms of carcinoid syndrome symptoms; and reductions in flushing and abdominal pain were not statistically significant.
Additional data regarding results of the extension period when all patients crossed over to telotristat ethyl 500 mg tid were reported in 2016 [81]. The extension period included a total of 115 patients, and demonstrated that the reduction in mean bowel movements was sustained through the full duration of the study (up to 35 weeks of follow-up), together with an improvement on urinary 5HIAA (reduction of 40.1% (p-value <0.001) and 57.7% (p-value <0.001) compared to baseline for patients on telotristat ethyl 250 mg tid and 500 mg tid, respectively), confirming the proof-of-principle. It is worth highlighting
10 that the clinical implications of such reduction in 5-HIAA, beyond improvement in diarrhoea, remain unclear, particularly in terms of preventing some of the long-term complications of carcinoid syndrome, including carcinoid heart disease and mesenteric fibrosis. Although animal models exist for research into this scenario [53;82], only few studies have explored the implications of serotonin inhibition on carcinoid heart disease [52] and no data with telotristat ethyl is available as yet.
Provisional data from the TELECAST clinical trial were released in the form of a press release in December 2015 [78] and presented in NANETS conference on 2016 [79]. The TELECAST clinical trial had an identical trial design to the TELESTAR trial [77], with the exception of including patients with <4 daily bowel movements and other carcinoid syndrome symptoms (such as flushing and abdominal pain). Seventy-six patients were randomised into this trial. Results of this study confirmed an improvement in urinary 5-HIAA (p-value <0.001 for both telotristat ethyl arms compared to placebo) and reduction in daily bowel movements (p-value of 0.004 and <0.001 for the 250 and 500 mg tid arm compared to placebo) at week 12 [77]. Full results of this study are pending.
6. Patient-reported outcomes Due to the difficulties in assessing the clinical impact of reduction in bowel movements identified in the above mention clinical studies, quality of life and other patient-reported outcomes have been extensively explored in telotristat ethyl-treated patients.
Patient-reported outcomes (including quality of life questionnaires, electronic diaries and face-to-face interviews) were collected during a number of clinical trials utilising telotristat ethyl: 80% of patients reported having “adequate symptom relief” at the end of the 12-week period in the study by Pavel et al [76]. In addition, the second phase II clinical trial [74] performed one-to-one interviews with 11 patients to explore, in detail, symptom improvement from a patient perspective [83]. All patients identified diarrhoea as one of the main symptoms of carcinoid syndrome at study entry and 82% of patients described an improvement in diarrhoea. Based on these results, further studies were developed using diarrhoea improvement as the primary end-point [77]. Patient-reported outcome data from the phase III studies is pending, which will clarify whether the statistically significant reduction in absolute and relative number of bowel movements shows an impact on patients’ quality of life in order to assess clinical impact.
7. Safety and tolerability Safety data for telotristat ethyl is available for patients with carcinoid syndrome from phase I [71], phase II [74;76] and phase III [77] clinical trials. Table 3 summarises the adverse events reported to be related to telotristat ethyl.
Within phase I clinical trials, adverse events were mainly related to the gastrointestinal tract [71]. A similar toxicity profile was shown in the phase II studies. Adverse events were mostly gastrointestinal (67%), consistent with underlying illness. Three serious adverse events (abdominal pain, diarrhoea
11 and gastroenteritis) were reported by Pavel et al, which were not considered related to telotristat ethyl [76]. Kulke et al reported [74] one severe adverse event, nausea, which was classified as possibly related to study drug which occurred in the 350 mg tid dose group.
In the phase III TELESTAR clinical trial [77], telotristat ethyl was safe and well tolerated. However, events of depression were reported, most were mild or moderate and resolved while continuing therapy. There were no imbalances regarding toxicity between treatments arms. Similar findings were observed in the TELECAST study [78;79]. The concern regarding the potential implication in mood and depression from long-term serotonin synthesis inhibition has been address by the telotristat studies [68], in which such adverse-events have been defined as “adverse-events of special interest” and are been prospectively assess in the ongoing studies (Table 3). It is worth noting, however, that the molecular weight of telotristat is high and it is therefore not expected to cross the blood-brain barrier [71;84]. Final results from the long-term dosing TELEPATH (NCT02026063) [75] are awaited and may clarify this issue further.
8. Regulatory affairs Based on the statistically-significant and clinically meaningful reductions in bowel movement frequency reported in the TELESTAR trial, telotristat ethyl has emerged as a new option in the treatment of patients with carcinoid syndrome refractory to treatment with SSA, representing a promising new class of treatment for these patients. These potentially practice-changing results have triggered priority review of telotristat ethyl by the Food and Drug Administration (FDA) to assess its new indication in the management of refractory carcinoid syndrome following failure of SSAs [85]. Telotristat ethyl is, as yet, a non-commercialised drug and therefore price and cost implications are still to be defined.
9. Conclusion Around 20% of patients with carcinoid syndrome and around 50% of patients with highly-functional carcinoid syndrome (≥4 daily bowel movements) won’t achieve adequate symptom relief with SSAs alone. Telotristat ethyl inhibits serotonin production, evidenced by a reduction in the production of down-stream metabolites. In doing so, this novel agent achieves a statistically and clinically meaningful reduction of carcinoid syndrome symptoms in patients who are refractory to SSAs. Moreover, the safety profile is very favourable with very few adverse events, although data is still awaited on long-term dosing, as would be expected in these patients. Telotristat ethyl is pending regulatory agencies evaluation and is likely to change the standard treatment options for this population of patients in the future.
12 10. Expert opinion Diarrhoea secondary to refractory carcinoid syndrome impacts on patients’ daily activities and quality of life. Currently-available supportive measures including SSAs, loperamide and codeine may provide relief for the majority of patients, but there is a significant minority where diarrhoea remains troublesome. Telotristat ethyl can provide adequate symptom relief in patients with carcinoid syndrome-related diarrhoea who failed to respond satisfactorily to SSAs. In addition, its impact on patient-reported outcomes has been confirmed prospectively although results from the phase III studies are awaited. Therefore, upon approval by regulatory agencies, telotristat ethyl will provide a new line of treatment for patients with refractory carcinoid syndrome where alternative treatments to SSAs are lacking. Due to the favourable safety profile of telotristat ethyl, its patient-friendly formulation (oral administration), in addition to the reported benefit in patient’s symptom control, both physicians and patients, may seek to include telotristat ethyl into their management strategy. This is in keeping with the successful recruitment into all the clinical trials exploring this indication for telotristat ethyl. One of the limitations of this drug may be the fact that there are other mediators of the carcinoid syndrome other than serotonin, which may dilute the benefit from telotristat ethyl. Long-term safety and efficacy data are still required. These are expected to be provided by the ongoing TELEPATH study. Specifically, clarification on its impact on mood and depression is of interest. The effect of telotristat ethyl on other symptoms of carcinoid syndrome beyond diarrhoea, such as flushing and wheezing are awaiting results from ongoing studies. In addition, impact on development of carcinoid heart disease and mesenteric fibrosis remains unknown, since clinical trials have not been powered for this end-point. In addition, other aspects such as its addition earlier in the patients pathways should be explored in future research.
11. Drug summary box
Drug name Telotristat ethyl (LX1032/LX1606) Phase Phase III Indication Carcinoid syndrome refractory to somatostatin analogues. Pharmacology description/mechanism of Telotristat ethyl is an ethyl ester prodrug. action Telotristat ethyl is supplied in a white coated oval tablet formulation containing 250 mg. Following oral administration, telotristat ethyl is rapidly hydrolysed to its active form: telotristat (LP- 778902), which, by inhibition of tryptophan hydroxylase (TPH), reduces production of serotonin and improves carcinoid syndrome- related symptoms. Activity is mainly in the gastrointestinal tract, with minimal effects
13 reported on the brain and cardiovascular system, accompanied by an excellent safety profile.
Pharmacokinetic profile includes a Tmax of 2-4
hours and a half-life (T1/2) of 4-12 hours, supporting the 8-hourly administration [74]. Telotristat ethyl is mainly excreted in faeces, and is metabolised by the liver. No significant drug- drug interactions have been described. Route of administration Oral administration (three times daily). Pivotal trial(s) Two phase III clinical trials have confirmed its activity in patients with carcinoid syndrome refractory to SSA: TELESTAR [78] and TELECAST studies [77;81]. Both studies included a 12-week period with double-blind treatment. Patients were randomised into three arms: placebo, telotristat ethyl 250 mg three times daily or telotristat ethyl 500 mg three times daily. While the TELESTAR trial included patients with highly- functional carcinoid syndrome only (defined as ≥4 daily bowel movements), TELECAST included patients with <4 daily bowel movements. Both studies met their primary end-point, reporting a statistically significant and clinically meaningful reductions in bowel movements after 12-weeks of treatment. These results are in keeping with previous findings suggesting benefit reported in phase I and II studies as well as patient-reported evidence.
14 12. References
*Important reference
** Very important reference
*Cite 4 and 5: ENETs guidelines for Net management
*Cite 6 and 15: Phase III trials showing anti-tumour effect of SSAs
*Cite 35: Phase III trial showing activity of PRRT in midgut NETs
**Cite 49: Phase III trial showing activity of everolimus in non-secretory NETs
*Cite 63: Use of above-label doses of SSAs
*Cite 74 and 76: Phase II trials of Telotristat
**Cite 77 and 81: Data from the TELESTAR phase III trial
**Cite 79: Data from the TELECAST phase III trial
15 13. Figures and Tables
16 Control of hormone Control of Type of treatment Rationale supporting use in patients with GI-NETs secretion tumour growth
Somatostatin analogues Phase III clinical trials and previous experience have confirmed not only anti-secretory but also anti-proliferative effect of Yes (immediate) Yes (SSAs) SSAs [6;7;16-22]. The PROMID clinical trial [6] randomised patients with functional and non-functional tumours to octreotide LAR and placebo, achieving a median time to tumour progression in the octreotide LAR and placebo group of 14.3 and 6 months, respectively (HR 0.34 (95%CI 0.20-0.59); p-value 0.000072). The CLARINET clinical trial randomised patients with non-functional gastrointestinal NET to receive either lanreotide or placebo: lanreotide showed a prolonged PFS over placebo with HR of 0.47 (95%CI 0.30-0.73; p-value 0.0002) [15].
Pasireotide, may be an alternative to the above-mentioned SSAs; however its role as first-line option is unclear due to high rate of treatment-related hyperglycaemia [31]. In addition, its role as rescue strategy following failure of octreotide was not confirmed in a phase III randomised study when compared to increased dose of octreotide LAR (40 mg every 4 weekly) [32].
See Table 2 for further details regarding the anti-secretory effect of SSAs.
Interferon (IFN) Interferon (IFN) is thought to control the secretion of tumour products and to inhibit tumour growth by activation of the T-cell Possible (delayed) Yes response against the tumour and inhibition of angiogenesis. Interferon has been used and tested in many retrospective and prospective studies resulting in reduction of symptoms related to hormone secretion in 40-50% patients and a partial response rate of around 10% [24].
Peptide receptor Targeted radiotherapy using radiolabelled SSA can be used for patients with avid tracer uptake on somatostatin receptor Possible (delayed) Yes radionuclide therapy (PRRT) imaging (i.e. octreotide scan or gallium-PET). The most frequently used radionuclides include yttrium (90Y) and lutetium (177Lu) [33;34]. Confirmation of efficacy was reported in the phase III NETTER-1 clinical trial [35] which randomised 230 patients, with progressive disease to previous SSA, to 177Lu-DOTA0-Tyr3-Octreotate (Lutathera) or increased dose of SSA (Octreotide LAR 60 mg every 4-weeks). While the median PFS was not reached for Lutathera, it was 8.4 months with 60 mg Octreotide LAR (95%CI 5.8-11.0; p-value < 0.0001), achieving a HR of 0.21 (95%CI 0.13-0.34). Interestingly, rate of partial objective responses by RECIST v.1.1 [25] was one of the highest ever shown in this patient population (18.8%), even when compared to cytotoxic chemotherapy (estimated to be around 12%) [23]. In addition to the benefit in delaying progressive disease, PRRT has also shown improvement of carcinoid syndrome-related symptoms in a small study [36]; however this has not been confirmed in randomised studies.
Cytotoxic chemotherapy In selected cases chemotherapy can be useful for the treatment of GI-NETs. Although chemotherapy is thought to be Possible (delayed) Yes
17 particularly active in NETs of pancreatic origin [37-39], it can also be a treatment option for patients with GI-NETs with a high tumour burden [40;41]. One of the most used drugs is streptozocin, which is often combined with 5-fluorouracil, but perhaps less commonly employed now in comparison to the temozolomide/capecitabine combination. Currently no standard chemotherapy schedule is available for patients with NET and treatment selection is made depending on comorbidities or expected toxicity profile; overall response rate is expected to be around 12% [23]. Chemotherapy may be more effective in patients with a higher proliferative activity [42].
Liver-directed therapies For patients with liver-predominant metastases, local liver-directed therapies such as debulking surgery [26] or hepatic Possible (early) Yes arterial embolisation [27] may be of benefit. A secretory syndrome response is obtained in 52-86% of cases with a duration of response which may be even longer than 12 months [43;44]. Symptomatic response seems to be even higher when used as a first-line therapy (70% complete symptomatic response, 20% partial response) [45].
Targeted therapies Targeted therapies such as everolimus [46] and sunitinib [47] have shown activity in patients with pancreatic Wd-NETs. Possible (delayed) Yes, not effective Unfortunately, their development has not been straight forward in GI-NETs. The RADIANT-2 [48] phase III clinical trial in functional GI- reported no clear benefit to everolimus versus placebo in patients with functional GI-NETs. Everolimus did result in an NETs improved PFS for patients with non-syndromic small bowel and lung NETs in the RADIANT-4 clinical trial [49] (median PFS of 11.0 months (95%CI 9.2-13.3) vs. 3.9 (95%CI 3.6-7.4); HR 0.48 (95%CI 0.35-0.67); p-value <0.00001). Table 1: Summary of treatment options for management of advanced well-differentiated NETs arising from the small bowel (GI-NETs)
SSA: somatostatin analogue; Wd: well differentiated; GI: gastrointestinal; NET: neuroendocrine tumour; PFS: progression-free survival; LAR: long acting; HR: hazard ratio; 95%CI: 95% confidence interval; PET: positron emission tomography; RECIST: response evaluation criteria in solid tumours.
18 Study Number of patients (N) SSA, dose Carcinoid syndrome response Other details
Octreotide LAR** 30 PROMID trial [6] 42 mg / 4 weeks, Not reported intramuscular
Lanreotide depot** 120 CLARINET trial [15] 103 mg / 4 weeks, deep Non-functional patients included only subcutaneous
The odds ratio of full/partial treatment success The adjusted mean percentage days with rescue Lanreotide depot** 120 (defined as ≤3 days short-acting octreotide use octreotide use (primary endpoint) was significantly lower ELECT study[57] 59 mg every 4 weeks, between weeks 12-15) was significantly greater in the lanreotide (33.7%) compared to placebo (48.5%); deep subcutaneous with lanreotide than placebo (2.4 [95% CI: 1.1, p-value 0.017. 5.3]; p-value 0.036).
Almost all patients were receiving 4- weekly lanreotide 76% were 'completely' or 'rather' satisfied with depot** at standard 79% reported improvement in diarrhoea with lanreotide. diarrhoea control; the proportion of patients with SYMNET study[58] 273 doses of 60–120 mg: Satisfaction with flushing control amongst patients with 'mild', 'minimal', or 'no diarrhoea' increased from (60 mg, 28%; 90 mg, significant flushing at treatment initiation was 73%. 33% before treatment to 75% during treatment 35% and 120 mg, (93%); deep subcutaneous
Daily lanreotide* 13 (2250-9000 µg), Not reported intramuscular Anthony et al [16] Daily octreotide* 14 (1500-6000 µg), Not reported subcutaneous
The greatest improvement in symptoms was 55, highly syndromic patients 49% and 53.8% of patients had improved symptoms identified at 6 months following treatment were included (defined as Lanreotide depot** 30 (any) of at least 50% at 1 month and at end of treatment commencement. No changes in echo findings Wymenga et al [17] average ≥ 3 stools per day and / mg/2 weeks, deep visit, respectively. The rates of improvement were 36.8% or echo not done at 6 months. Clinical or 1.5 moderate or severe subcutaneous and 42.1% for diarrhoea and 40.8% and 47.6% for improvement was defined as symptom flushing per day) flushing, respectively. reduction in ≥ 50% compared to baseline.
19 Short-acting Flushing and diarrhoea associated with the carcinoid Kvols et al [18] 25 octreotide*, syndrome were promptly relieved in 22 out of the 25 subcutaneous patients (88%).
Octreotide* 51 with carcinoid syndrome (39 Improvement in 57.7% of patients (any symptom); Clinical response was defined as improvement monotherapy 200 µg Arnold et al [19] patients with data for clinical flushing 83.3%, diarrhoea 57.9% and abdominal pain in ≥ 50% of tumour-related symptoms three times per day, response) 33.3%. compared to baseline. subcutaneous
Overall symptomatic response was achieved in 70% of Assessment of clinical benefit was defined as patients (65% of patients achieved complete response complete response if symptoms were 25 (no clear inclusion criteria), Lanreotide depot** 30 (defined as complete relief of all symptoms and 5%). completely relieved and partial response if Ricci et al [20] 17 were assessable for clinical mg/2 weeks, stable disease. The rate of complete clinical response there was a reduction of at least 50% in both response intramuscular was 6/11, 5/5 and 1/1 of patients with diarrhoea, the frequency and intensity of flushing and/or abdominal pain and flushing respectively. diarrhoea.
Lanreotide depot** 30 After six months of treatment, 54% and 56% of patients Rusznieski et al [21] 39 with carcinoid syndrome mg/2 weeks, had a reduction of at least 50% decrease in number of intramuscular episodes of flushing and bowel movements, respectively.
A reduction was also observed in urinary 18 patients; 10 with carcinoid Lanreotide* 30 mg/10 In patients with carcinoid tumours, lanreotide markedly Tomasetti et al [22] serotonin and urinary 5-hydroxyindoleacetic syndrome days, intramuscular reduced daily bowel movements and flushing episodes. acid, although it was not statistically significant.
Octreotide 40 mg/4 110 patients with SSA-refractory weeks**, intramuscular Forty-three patients in the pasireotide arm (20.9%) Study was interrupted following a planned carcinoid syndrome daily mean (57 patients) showed symptom control, compared 55 (26.7%) in the interim analysis, due to of a low predictive Wolin et al [32] of 4 or more bowel movements octreotide group (odds ratio, 0.73 (95% confidence probability of showing superiority of pasireotide over 2-week screen period or 5 Pasireotide 60 mg/4 interval 0.27-1.97; p-value 0.53) over octreotide for symptom control. or more flushes/day weeks**, intramuscular (53 patients)
Table 2: Details on carcinoid syndrome control with somatostatin analogues alone.*short-acting **long acting.
20 Phase II clinical trial Randomised Phase II Phase III clinical trial (TELESTAR) clinical trial Phase I clinical trials [71] (Pavel et al, 2015 (Kulke et al, 2015 [77;81]) [76]) (Kulke et al, 2014 [74])
Adverse Events (all Telotristat Telotristat grades) ethyl arm Telotristat Telotristat Placebo ethyl arm Placebo Placebo arm Telotristat ethyl arm (115 ethyl arm (88 ethyl arm arm (5 (90 patients, arm (45 (21 patients) (15 patients) patients, patients) (18 patients) patients) double blind patients [77]) extension period [77]) period [81]) Nausea 12.5% 9.5% 13.3% 27.8% 20% 22.2% 20% 11.1% Diarrhoea 10.2% 14.3% 20% 38.9% 40% NR NR NR Headache 8% 9.5% 26.7% 0% 20% NR NR NR Abdominal pain 6.8% 0% 46.7% 16.7% 0% NR NR NR Constipation 2.3% 9.5% - 5.6% 0% NR NR NR Vomiting 3.4% 0% 13.3% 5.6% 0% NR NR NR Abdominal NR distension / 2.3% 0% 13.3% 22.2% 20% NR NR Flatulence Dyspepsia 1.1% 4.8% NR NR NR NR NR NR Feeling cold 2.3% 0% NR NR NR NR NR NR Infusion site pain 2.3% 0% NR NR NR NR NR NR Pyuria 2.3% 0% NR NR NR NR NR NR
21 Upper respiratory NR 2.3% 0% NR NR NR NR NR infection Elevated hepatic NR enzymes (≤ x2 NR NR 6.7% 0% 20% NR NR upper limit of normal) Lethargy / Fatigue / NR NR NR 13.3% 22.2% 20% NR NR Asthenia Depression NR NR NR 5.6% 0% 17.7% 5.2% 6.7% Sleeping disorders NR NR NR 5.6% 0% NR NR NR Anxiety NR NR NR 5.6% 0% NR NR NR
Table 3: Summary of adverse events reported in clinical trials of telotristat ethyl. NR: not reported.
22 Figure1: 1a: 2D structure of telotristat ethyl salt , so called telotristat etiprate (2-benzamidoacetic acid;ethyl (2S)-2-amino-3-[4-[2-amino-6-[(1R)-1-[4-chloro-2- (3-methylpyrazol-1-yl)phenyl]-2,2,2-trifluoroethoxy]pyrimidin-4-yl]phenyl]propanoate) [72]; 1b: Tryptophan and serotonin pathway, including mechanism of action of telotristat ethyl (TPH inhibition) and SSA (inhibition of serotonin secretion). SSA: somatostatin analogue, TP: tryptophan hydroxylase, AADC: aromatic amino acid decarboxylase, 5-HIAA: 5-hydroxyindoleacetic acid, IFN: interferon.
NET cell
Tryptophan Inhibition Telotristat TPH Ethyl 5-hydroxytryptophan AADC Serotonin
Inhibition Serotonin SSAs/ IFN secretion Serotonin in blood
5-HIAA
5-HIAA filtered by kidney
5-HIAA in urine A B
23 Figure 2: Trial design of the two main phase III studies: TELESTAR [77;81] and TELECAST [78]. *Assessment of inclusion criteria based on electronic diary. R: randomisation; tid: three tmes daily; TE: telotristat ethyl.
24 14. Declaration of Interest Authors have no conflict of interest related to this manuscript. A Lamarca and J Barriuso are part-funded by SEOM (Spanish Society of Medical Oncology) Translational Fellowship Grants.
JW Valle has received Honoraria and a Travel Grant from Ipsen.
25