Gallagher Bassett Services, GALLAGHER BASSET SERVICES, INC. Inc.
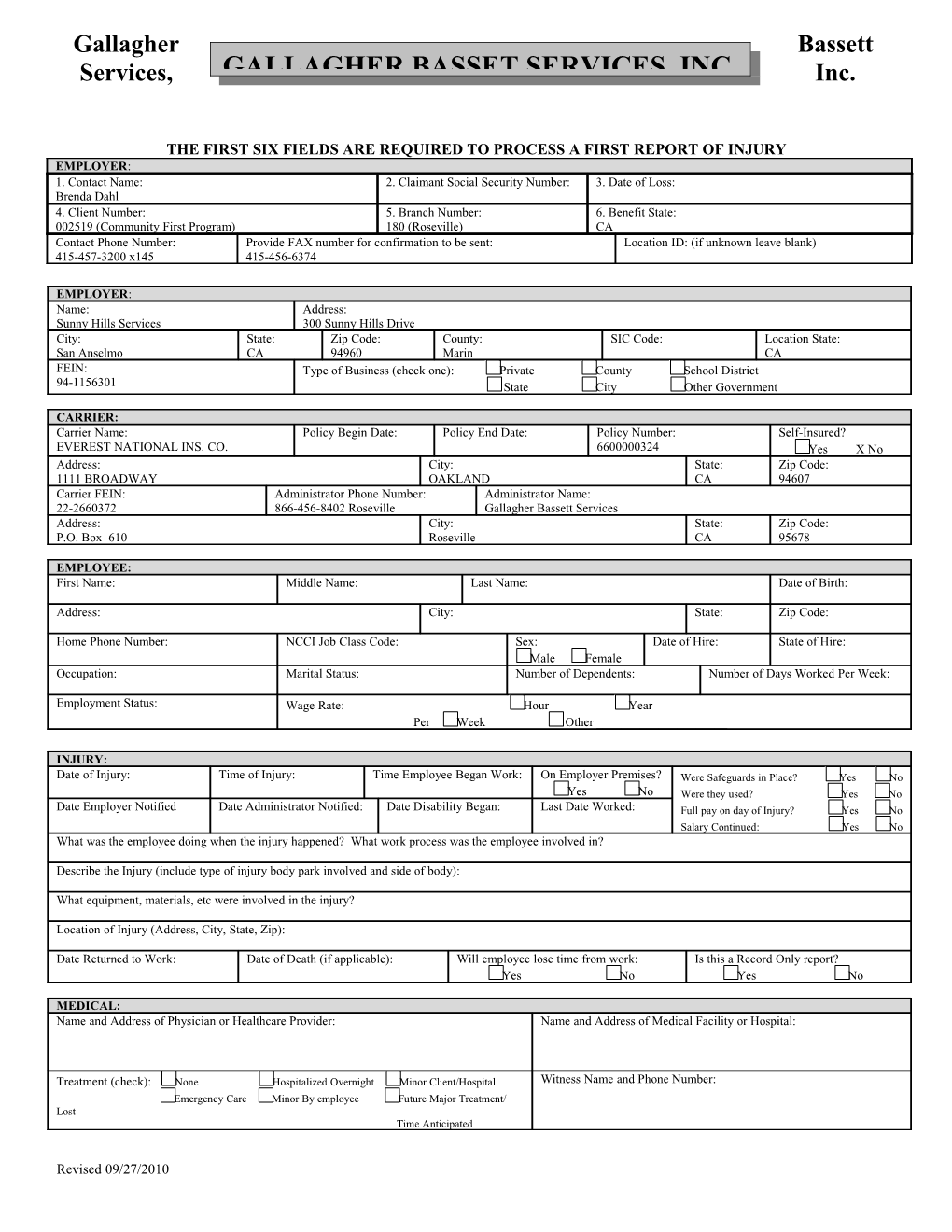
THE FIRST SIX FIELDS ARE REQUIRED TO PROCESS A FIRST REPORT OF INJURY EMPLOYER: 1. Contact Name: 2. Claimant Social Security Number: 3. Date of Loss: Brenda Dahl 4. Client Number: 5. Branch Number: 6. Benefit State: 002519 (Community First Program) 180 (Roseville) CA Contact Phone Number: Provide FAX number for confirmation to be sent: Location ID: (if unknown leave blank) 415-457-3200 x145 415-456-6374
EMPLOYER: Name: Address: Sunny Hills Services 300 Sunny Hills Drive City: State: Zip Code: County: SIC Code: Location State: San Anselmo CA 94960 Marin CA FEIN: Type of Business (check one): Private County School District 94-1156301 State City Other Government
CARRIER: Carrier Name: Policy Begin Date: Policy End Date: Policy Number: Self-Insured? EVEREST NATIONAL INS. CO. 6600000324 Yes X No Address: City: State: Zip Code: 1111 BROADWAY OAKLAND CA 94607 Carrier FEIN: Administrator Phone Number: Administrator Name: 22-2660372 866-456-8402 Roseville Gallagher Bassett Services Address: City: State: Zip Code: P.O. Box 610 Roseville CA 95678
EMPLOYEE: First Name: Middle Name: Last Name: Date of Birth:
Address: City: State: Zip Code:
Home Phone Number: NCCI Job Class Code: Sex: Date of Hire: State of Hire: Male Female Occupation: Marital Status: Number of Dependents: Number of Days Worked Per Week:
Employment Status: Wage Rate: Hour Year Per Week Other ______
INJURY: Date of Injury: Time of Injury: Time Employee Began Work: On Employer Premises? Were Safeguards in Place? Yes No Yes No Were they used? Yes No Date Employer Notified Date Administrator Notified: Date Disability Began: Last Date Worked: Full pay on day of Injury? Yes No Salary Continued: Yes No What was the employee doing when the injury happened? What work process was the employee involved in?
Describe the Injury (include type of injury body park involved and side of body):
What equipment, materials, etc were involved in the injury?
Location of Injury (Address, City, State, Zip):
Date Returned to Work: Date of Death (if applicable): Will employee lose time from work: Is this a Record Only report? Yes No Yes No
MEDICAL: Name and Address of Physician or Healthcare Provider: Name and Address of Medical Facility or Hospital:
Treatment (check): None Hospitalized Overnight Minor Client/Hospital Witness Name and Phone Number: Emergency Care Minor By employee Future Major Treatment/ Lost Time Anticipated
Revised 09/27/2010 ______Employer’s Signature Report Prepared By (Name & Title) Date Prepared
Revised 09/27/2010