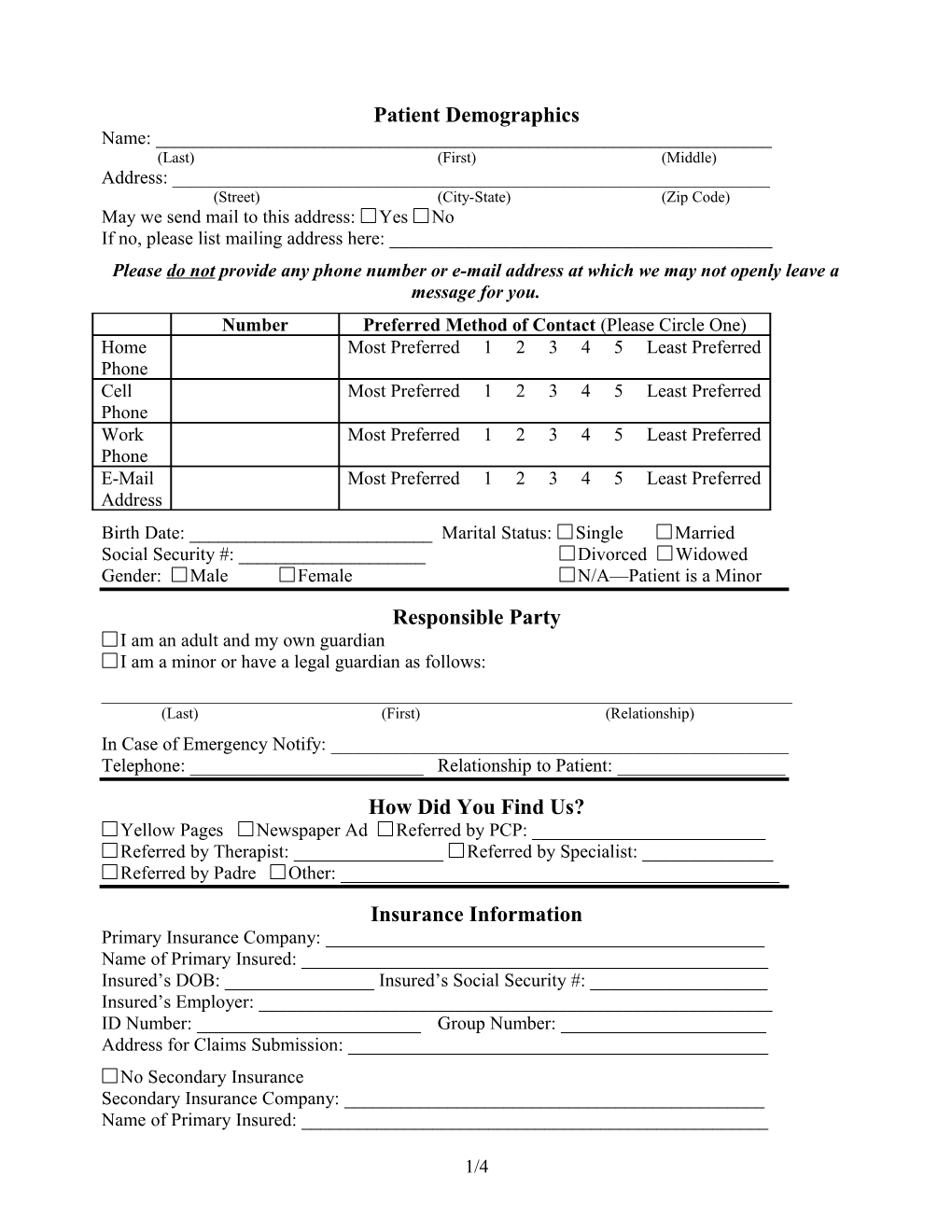
Patient Demographics Name: ______(Last) (First) (Middle) Address: ______(Street) (City-State) (Zip Code) May we send mail to this address: Yes No If no, please list mailing address here: ______Please do not provide any phone number or e-mail address at which we may not openly leave a message for you. Number Preferred Method of Contact (Please Circle One) Home Most Preferred 1 2 3 4 5 Least Preferred Phone Cell Most Preferred 1 2 3 4 5 Least Preferred Phone Work Most Preferred 1 2 3 4 5 Least Preferred Phone E-Mail Most Preferred 1 2 3 4 5 Least Preferred Address Birth Date: ______Marital Status: Single Married Social Security #: ______Divorced Widowed Gender: Male Female N/A—Patient is a Minor Responsible Party I am an adult and my own guardian I am a minor or have a legal guardian as follows: ______(Last) (First) (Relationship) In Case of Emergency Notify: ______Telephone: ______Relationship to Patient: ______How Did You Find Us? Yellow Pages Newspaper Ad Referred by PCP: ______Referred by Therapist: ______Referred by Specialist: ______Referred by Padre Other: ______Insurance Information Primary Insurance Company: ______Name of Primary Insured: ______Insured’s DOB: ______Insured’s Social Security #: ______Insured’s Employer: ______ID Number: ______Group Number: ______Address for Claims Submission: ______No Secondary Insurance Secondary Insurance Company: ______Name of Primary Insured: ______
1/4 Insured’s DOB: ______Insured’s Social Security #: ______Insured’s Employer: ______ID Number: ______Group Number: ______Address for Claims Submission: ______
Authorizations/Guarantee of Payment for Treatment Rendered Signatures by patient (parent/guardian for minors) on all of the following are required for treatment at this office. I hereby authorize the release of any medical information necessary for the processing of insurance claims. I hereby assign all medical benefits for services rendered by Michael Hernandez, MD, including major benefits to which I am entitled, to Michael Hernandez, MD. This assignment will remain in effect until revoked by me in writing. A photocopy of this assignment is to be considered as valid as an original. Signature: ______I understand that responsibility for payment is mine. Michael Hernandez, MD, will bill my insurance company as a courtesy if applicable, but I agree that if my insurance company does not remit payment to Michael Hernandez, MD, within 60 days or if I am a self-pay patient, I will pay my account. Cash, check (payable to Michael Hernandez), Visa and MasterCard are accepted. Signature: ______I realize that understanding my insurance policy is my responsibility. It is likewise my responsibility to know whether I have a deductible and whether or not that deductible has been met. While this office will attempt pre-certification on my insurance prior to the visit if the needed information has been provided by me, it is ultimately my responsibility to pay any balances left by claims denied due to unmet deductibles and/or lack of pre-certification caused by my not providing the needed information to this office at least 48 business hours before my new patient evaluation and/or before my follow up visit if my insurance has changed. Signature: ______
Policies Please read each policy and then sign below (parent/guardian must sign for minor) to indicate acceptance of this office’s policies. I understand that: 1. To schedule or reschedule an appointment, I should call 906-0166 during normal business hours (9 am-12 pm; 2 pm-4 pm). 2. It is my responsibility to notify this office of any changes in my address, phone and/or insurance and that if I do not provide this updated information I will be responsible for any charges incurred. 3. This office has a policy that I will be responsible for attending on time any appointment scheduled with my knowledge. Patients arriving more than 5 minutes late for an appointment will be rescheduled at the next available time slot, which is often 1-2 months for follow up visits. Patients missing a new patient or hospital follow up appointment will not be rescheduled. Repeated tardiness is grounds for termination of care.
2/4 4. While this office makes every effort to make confirmation phone calls the day before a scheduled appointment, it is my responsibility to make note of and attend any appointment scheduled for me with my knowledge. 5. If I miss a follow up appointment or cancel with less than 24 hours notice given I will be required to pay a “No Show” fee (except Medicaid patients) equal to my co-pay or 25% of the visit charges if I have no co-pay. I further understand that these charges cannot be billed to my insurance company and are my sole responsibility. No patient who currently owes a No Show fee will be rescheduled until the No Show fee has been paid. 6. This office has a two No-Show policy by which any patient missing two follow up appointments without properly giving notice of at least 24 hours may be terminated from treatment. Patients missing a new patient or hospital follow up appointment will not be rescheduled. 7. If I have an emergency situation outside of business hours, especially if experiencing suicidal or homicidal thoughts or significant adverse reactions to medications, I will need to call 911 or report to the nearest ER. Urgent messages may be left with the answering service and will be answered at the on-call doctor’s discretion or by the office staff during business hours if the doctor determines it is not urgent. It is highly recommended that I keep track of the medication I have on hand and call for refills during business hours (the earlier in the day, the better) as running out of medication under normal circumstances is not considered by this office to be an urgent message that will be responded to outside of business hours. I further understand that misrepresenting my situation to the answering service in order to be transferred to the doctor will be grounds for termination of treatment at this office. 8. Medication refill requests will not be honored unless it is time for the prescription to be refilled (i.e. medication has been taken in amounts prescribed by the doctor) and that the charge for a requested controlled substance prescription that is not picked up within 7 days of request is $5 (except for Medicaid patients who will be subject to termination after failing to claim 2 such prescriptions). 9. Prescription refill requests will not be honored if I have not seen the doctor within one month (unless the doctor has requested follow up beyond one month) as attendance at follow ups is as important to my treatment plan as medications. 10. Due to its potentially addictive nature and the availability of alternate treatment options, the doctor does not prescribe Xanax and that there are no exceptions to this policy. 11. The doctor does not prescribe pain medications and that all patients requiring such medications will be referred to a pain specialist. 12. There will be a fee for forms, reports and letters requested from the doctor (except Medicaid and Medicare patients) as follows: $25 for the first 25 pages and 15 cents per each additional page thereafter on records requests, $10 for short forms, $20 for long forms and recommendations. Patients requiring any of these services must come in and fill out a request form—no exceptions. Requests may take up to two weeks to fill depending on the number of requests received. 13. There is a $30 fee for phone calls to patients (except Medicaid and Medicare patients) that require a moderate level of complexity in medical decision making. This fee is due at the time of the next appointment or can be mailed if the appointment is not within the next four weeks. There is no fee for other phone calls including rescheduling appointments with 24 hour or greater notice, requesting sooner appointments or requesting medications/samples/refills. 14. The doctor reserves the right to terminate patient care upon verbal or written notice. Upon termination, the patient will be provided with urgent care and refills on recommended
3/4 medications only for a period of 30 days from notice of termination, allowing adequate time for me to seek establishment with another psychiatrist. Although termination is rare, reasons for termination include, but are not limited to, misrepresentation, misuse/abuse of medications, repeated noncompliance with doctor’s recommendations, threatening behavior, conflicts of interests, violation of this office’s policies and violation of the doctor-patient relationship.
______Signature of Patient Printed Name Date ______Signature of Parent/Guardian Printed Name Relationship Date
I witnessed that the patient understood the nature of this request/authorization and freely gave his or her consent, but was physically unable to provide a signature.
______Signature of Witness Printed Name Date Acknowledgement of Review of Privacy Practices I have reviewed this office’s Notice of Privacy Practices (posted in waiting room), which explains how my medical information will be used and disclosed. I understand that I am entitled to receive a copy of this document if I so desire (please request if this is the case).
______Signature of Patient Printed Name Date ______Signature of Parent/Guardian Printed Name Relationship Date
I witnessed that the patient understood the nature of this request/authorization and freely gave his or her consent, but was physically unable to provide a signature. ______Signature of Witness Printed Name Date
Complaints about physicians, as well as other licensees and registrants of the Texas Board of Medical Examiners, including Physician’s Assistants, may be reported to 333 Guadalupe, Tower 3, Suite 610, PO Box 2018, Austin, TX 78701. For assistance call 1-800-201-9351. A Note on the Remaining Forms in this Packet Please fill out these forms to the best of your knowledge and sign them. Leave blank questions you do not understand. The goal is to provide well-organized, important information in an efficient manner, allowing more time to focus on the present matters at hand while in session. The first form is a mood questionnaire to be completed by the patient. Please make note of the person completing the form if the patient is incapable of doing so. The following two forms obtain patient’s consent for sharing information with other physicians (optional) and for the doctor to treat the patient. The remaining forms attempt to gather a medical and psychological history of the patient and may be completed for a minor by a guardian or parent. Please return this completed packet along with photo identification, any insurance cards and your payment if applicable to the receptionist upon completion.
4/4