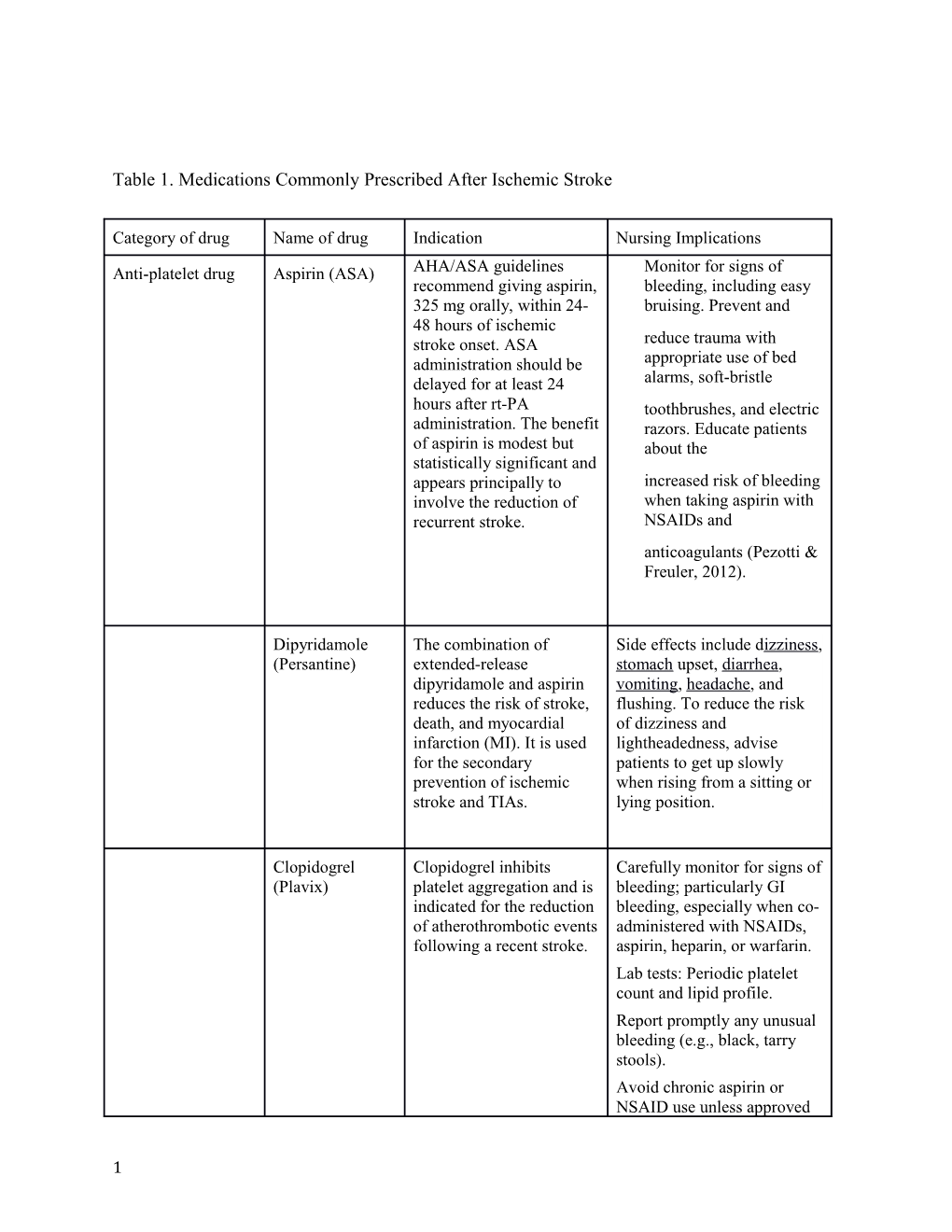
Table 1. Medications Commonly Prescribed After Ischemic Stroke
Category of drug Name of drug Indication Nursing Implications
Anti-platelet drug Aspirin (ASA) AHA/ASA guidelines Monitor for signs of recommend giving aspirin, bleeding, including easy 325 mg orally, within 24- bruising. Prevent and 48 hours of ischemic stroke onset. ASA reduce trauma with administration should be appropriate use of bed delayed for at least 24 alarms, soft-bristle hours after rt-PA toothbrushes, and electric administration. The benefit razors. Educate patients of aspirin is modest but about the statistically significant and appears principally to increased risk of bleeding involve the reduction of when taking aspirin with recurrent stroke. NSAIDs and anticoagulants (Pezotti & Freuler, 2012).
Dipyridamole The combination of Side effects include dizziness, (Persantine) extended-release stomach upset, diarrhea, dipyridamole and aspirin vomiting, headache, and reduces the risk of stroke, flushing. To reduce the risk death, and myocardial of dizziness and infarction (MI). It is used lightheadedness, advise for the secondary patients to get up slowly prevention of ischemic when rising from a sitting or stroke and TIAs. lying position.
Clopidogrel Clopidogrel inhibits Carefully monitor for signs of (Plavix) platelet aggregation and is bleeding; particularly GI indicated for the reduction bleeding, especially when co- of atherothrombotic events administered with NSAIDs, following a recent stroke. aspirin, heparin, or warfarin. Lab tests: Periodic platelet count and lipid profile. Report promptly any unusual bleeding (e.g., black, tarry stools). Avoid chronic aspirin or NSAID use unless approved
1 by physician. Do not breast feed while taking this drug.
Anti-coagulants Warfarin Warfarin is a Vitamin K Monitor for signs of occult (Coumadin) antagonist used to reduce and frank bleeding. Monitor the risk of death, recurrent vital signs and level of MI, and thromboembolic consciousness. Institute events such as stroke or precautions to prevent systemic embolization trauma, including bed alarms. after MI. Monitor PT/INR. Administer vitamin K/fresh frozen plasma/clotting factors as ordered. Educate patients concerning consistent intake of green leafy vegetables and importance of frequent laboratory monitoring (McCarron, 2010).
Dabigatran Dabigatran is an inhibitor Monitor for signs of occult (Pradaxa) of thrombin that prevents and frank bleeding. Monitor clot formation. It may be vital signs and level of used as an alternative to consciousness. Monitor CBC. warfarin for the prevention Institute precautions of stroke and systemic such as bed alarms to thromboembolism in prevent trauma. Educate patients with atrial patients about the fibrillation and risk factors for stroke. increased risk of bleeding when taken with aspirin, NSAIDs, and other anticoagulants (Pezzotti & Freuler, 2012).
Rivaroxaban Rivaroxaban, apixaban Same as above (Xarelto), and edoxaban are Factor Apixaban Xa inhibitors indicated to (Eliquis), reduce the risk of stroke Edoxaban and systemic embolism in (Savaysa) patients with nonvalvular atrial fibrillation.
2 Anti-hypertensives ACE inhibitors, Various anti- Monitor pulse; hold Angiotensin hypertensives, such as medication if bradycardia or receptor blockers, ACE inhibitors, beta- hypotension present. Monitor Beta-blockers, or blockers or calcium BP and observe for postural Calcium antagonists may be used hypotension. Monitor K+ antagonists for patients with systolic level. Avoid use of salt blood pressure higher than substitute (principal 220 mm Hg or diastolic ingredient: potassium salt) blood pressure above 120 and potassium supplements mm Hg. In those patients, because of the potential for a reasonable goal is to hyperkalemia. Notify lower blood pressure by physician of a persistent 15% during the first 24 nonproductive cough, hours after onset of stroke. especially at night, Care must be taken to not accompanied by nasal lower blood pressure too congestion. Stop drug quickly or aggressively, promptly if swelling of face, since this could worsen eyelids, tongue, lips, or perfusion in the penumbra. extremities occurs.
Anti-lipidemia “Statins” (eg. HMG-CoA reductase Periodically monitor Atorvastatin, inhibitors limit synthesis cholesterol (including HDL, Simvastatin) of cholesterol by the liver. LDL, and total cholesterol levels), triglycerides, creatine kinase, and other hepatic enzymes. Risk of hepatotoxicity is increased with concurrent use of acetaminophen or alcohol.
Monitor for signs of statin- induced rhabdomyolysis, such as dark colored urine, muscle pain, and elevated hepatic enzymes. Patient should avoid grapefruit.
Table adapted from Jauch, Saver, Adams, et al (2013). American Heart Association / American Stroke
Association Guidelines for the Early Management of Patients With Acute Ischemic Stroke.
Stroke, 44, p. 870-947. Available at: http://stroke.ahajournals.org/content/44/3/870
3