Christopher Smith # 30858384 Peggy Gnegy
1) The research field is pharmacology and deals with the abuse of amphetamines.
2) Dr. Gnegy (or her assistants) hypothesized that repeated amphetamine exposure in the synapses of neurons in the dopamine reward circuit leads to altered dopamine release due to amphetamine- induced neuroadaptations.
3) This hypothesis is important to test because adaptations in the function of the brain’s neurons following drug use are a major reason for relapses after a drug abuser stops taking amphetamines. If the changes that occur in the brain following repeated amphetamine use can be found and targeted, then treatments that could help ease drug withdrawal could be developed.
4) (a) Dr. Gnegy and her assistants used cultured rat PC12 cells to test amphetamine-induced actions based on their natural release of dopamine into the extracellular environment. (b) They administered amphetamine to the cells for short periods of time for five consecutive days. (c) They then stopped giving amphetamine to the cells for a period of 10 days after the first five days. (d) Following the 10th day, the cells were perfused using high pressure liquid chromatography. (e) During perfusion, the cells were treated in separate tubes with Ca2+, KN93 CaM Kinase II, and PKC.
5) Dr. Gnegy was growing cells in a culture where amphetamines were introduced for short amount of time on a daily basis. This resembles how a real drug abuser might interact with amphetamines. Then she stopped giving amphetamines to the cells to simulate a drug abuser in withdrawal for the same amount of time. After perfusing the cells with or without different chemicals (i.e. Ca2+ etc.), it was tested whether DAT-regulated dopamine release does or does not require Ca2+, KN93 CaM Kinase II, and/or PKC after repeated amphetamine exposure. Should the cells release more dopamine with Ca2+, KN93 CaM Kinase II, and PKC perfusion than without, amphetamine could be proven to induce changes in the function of DAT-regulated dopamine release.
6) There are two distinct classes of possible results that could be found from these experimentations. One, the researchers could find that after repeated amphetamine exposure, the PC12 cells could not release dopamine from their transporters without the aid of Ca2+, KN93 CaM Kinase II, and PKC. So the transporter would have been altered such that they became dependent on each of these molecules to function correctly following amphetamine use. There is also the possibility that only one or two of the three molecules/elements under scrutiny becomes vital to DAT function after amphetamine abuse. Either way, if at least one of the three molecules/elements proves to become imperative to DAT function after repeated amphetamine use, then amphetamine can be shown to cause alterations in subsequent dopamine release. On the other hand, DAT function could have been found to remain independent of all three molecules/elements and functioned normally without their aid. This should lead the researchers to look elsewhere, either upstream or downstream of DAT regulated dopamine release, to find other possible chemical adaptations due to amphetamine. 7)
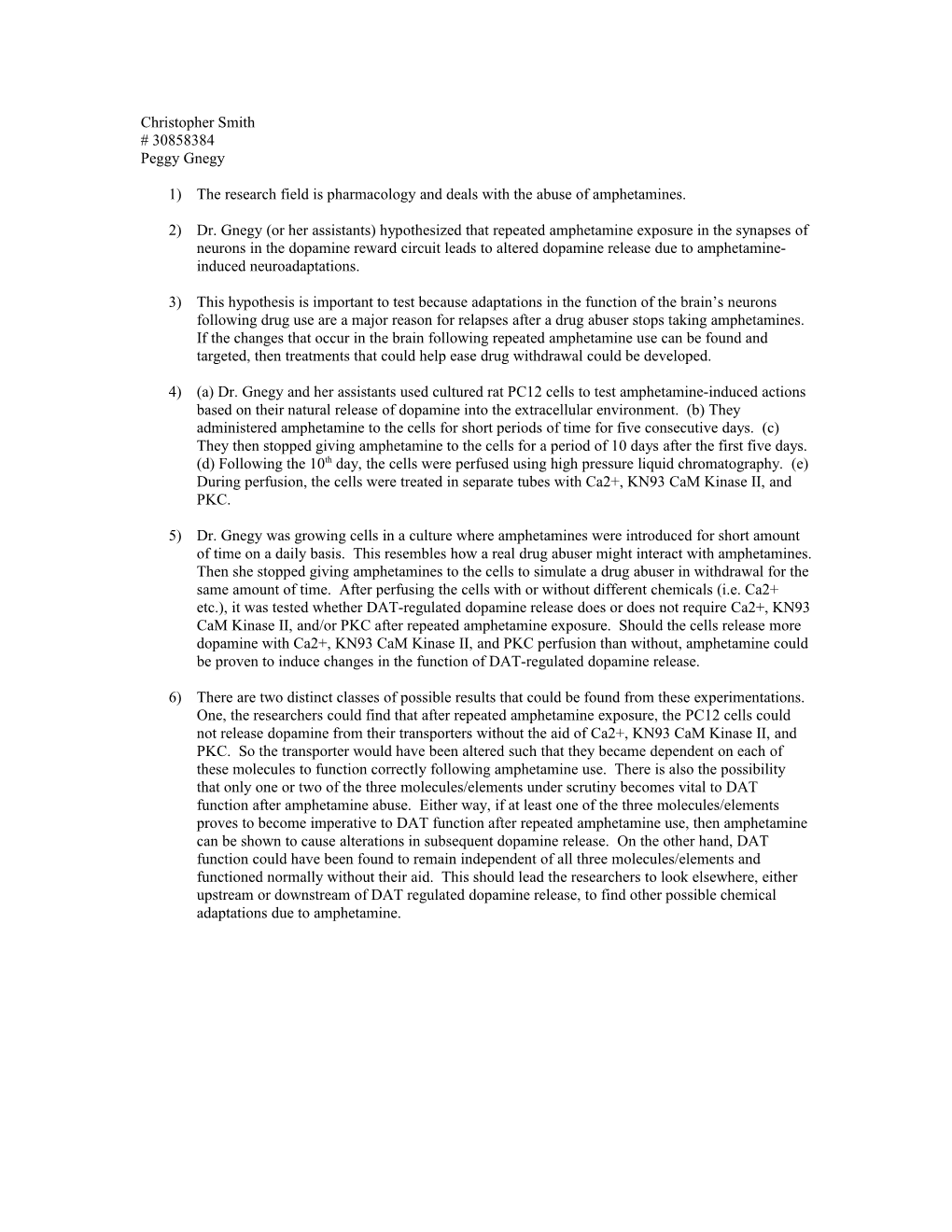
This diagram represents the pleasure a subject feels during the use of a drug and also when abstaining from drug use. While using the drug, the subject feels high levels of pleasure. But afterwards there is a clear drop in mood. And in the long term, this level of pleasure levels off at a level lower that what was begun with. This change in the pleasure “set point” leads to vulnerability to relapse for the subject. In this new set negative state, neurobiological changes occur to respond to the lack of drug use. These changes could include changes in the neurotransmission of dopamine and exaggeration of stress neurotransmission. The changes in neurotransmission that create negative emotional states during withdrawal would be factors in the development of an addiction and sequential relapses.
8) Q: When treating drug addicts, is it best to do so in a very stress free environment based on the research done which shows that animals exposed to repeated stressors reinstated themselves on drug self-administration? Do current clinical detoxification environments adhere to this?