George Michael Humphrey Birchenough
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Identification of BIRC6 As a Novel Intervention Target For
Lamers et al. BMC Cancer 2012, 12:285 http://www.biomedcentral.com/1471-2407/12/285 RESEARCH ARTICLE Open Access Identification of BIRC6 as a novel intervention target for neuroblastoma therapy Fieke Lamers1, Linda Schild1, Jan Koster1, Frank Speleman2, Ingrid ra3, Ellen M Westerhout1, Peter van Sluis1, Rogier Versteeg1, Huib N Caron4 and Jan J Molenaar1,5* Abstract Background: Neuroblastoma are pediatric tumors of the sympathetic nervous system with a poor prognosis. Apoptosis is often deregulated in cancer cells, but only a few defects in apoptotic routes have been identified in neuroblastoma. Methods: Here we investigated genomic aberrations affecting genes of the intrinsic apoptotic pathway in neuroblastoma. We analyzed DNA profiling data (CGH and SNP arrays) and mRNA expression data of 31 genes of the intrinsic apoptotic pathway in a dataset of 88 neuroblastoma tumors using the R2 bioinformatic platform (http://r2.amc.nl). BIRC6 was selected for further analysis as a tumor driving gene. Knockdown experiments were performed using BIRC6 lentiviral shRNA and phenotype responses were analyzed by Western blot and MTT-assays. In addition, DIABLO levels and interactions were investigated with immunofluorescence and co-immunoprecipitation. Results: We observed frequent gain of the BIRC6 gene on chromosome 2, which resulted in increased mRNA expression. BIRC6 is an inhibitor of apoptosis protein (IAP), that can bind and degrade the cytoplasmic fraction of the pro-apoptotic protein DIABLO. DIABLO mRNA expression was exceptionally high in neuroblastoma but the protein was only detected in the mitochondria. Upon silencing of BIRC6 by shRNA, DIABLO protein levels increased and cells went into apoptosis. Co-immunoprecipitation confirmed direct interaction between DIABLO and BIRC6 in neuroblastoma cell lines. -
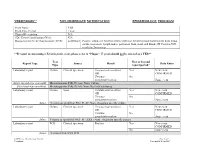
Yersiniosis** Non-Immediate Notification Epidemiology Program
YERSINIOSIS** NON-IMMEDIATE NOTIFICATION EPIDEMIOLOGY PROGRAM Event Name: YER Event Time Period: 1 year Clinical Description: N/A CDC Event Classification (N/A): N/A Massachusetts Event Classification (2015): Confirmed Positive culture of Yersinia enterocolitica or Yersinia pseudotuberculosis from throat swabs, mesenteric lymph nodes, peritoneal fluid, stool, and blood, OR Positive PCR result for Yersinia sp **If report is concerning a Yersinia pestis event, please refer to “Plague”. Y. pestis should not be entered as a YER** Test New or beyond Report Type Source Result Data Entry Type report period? Laboratory report Culture Clinical specimen Yersinia enterocolitica Yes New event OR CONFIRMED Yersinia No pseudotuberculosis Same event Select (no sub-type specified): Microorganism: PrId: Pt: xxx: Nom: Culture Select (sub-type specified): Microorganism: PrId: Pt: Islt: Nom: Bacterial subtyping Laboratory report Culture Stool Yersinia enterocolitica Yes New event OR CONFIRMED Yersinia No pseudotuberculosis Same event Select: Yersinia sp identified: Prld: Pt: Stl: Nom: Organism specific culture Laboratory report Culture Clinical specimen Yersinia enterocolitica Yes New event OR CONFIRMED Yersinia No pseudotuberculosis Same event Select: Yersinia sp identified: Prld : Pt : XXX : Nom : Organism specific culture Laboratory report PCR Clinical specimen Positive Yes New event CONFIRMED No Same event Select: Yersinia DNA XXX PCR MDPH Case Classification Manual Page 1 of 2 Yersiniosis Last modified: Jan 2017 Test New or beyond Report Type Source Result Data Entry Type report period? Laboratory report PCR Stool Detected Yes New event CONFIRMED No Same event Select: Y enterocol DNA: Stl: Ql: Non-probe: PCR Laboratory report PCR Stool Yersinia enterocolitica Yes New event CONFIRMED No Same event Select: GI path DNA+RNA: Pnl: Stl: Non-probe PCR We do not accept: Yersinia aldovae, Y. -

Annual Conference Abstracts
ANNUAL CONFERENCE 14-17 April 2014 Arena and Convention Centre, Liverpool ABSTRACTS SGM ANNUAL CONFERENCE APRIL 2014 ABSTRACTS (LI00Mo1210) – SGM Prize Medal Lecture (LI00Tu1210) – Marjory Stephenson Climate Change, Oceans, and Infectious Disease Prize Lecture Dr. Rita R. Colwell Understanding the basis of antibiotic resistance University of Maryland, College Park, MD, USA as a platform for early drug discovery During the mid-1980s, satellite sensors were developed to monitor Laura JV Piddock land and oceans for purposes of understanding climate, weather, School of Immunity & Infection and Institute of Microbiology and and vegetation distribution and seasonal variations. Subsequently Infection, University of Birmingham, UK inter-relationships of the environment and infectious diseases Antibiotic resistant bacteria are one of the greatest threats to human were investigated, both qualitatively and quantitatively, with health. Resistance can be mediated by numerous mechanisms documentation of the seasonality of diseases, notably malaria including mutations conferring changes to the genes encoding the and cholera by epidemiologists. The new research revealed a very target proteins as well as RND efflux pumps, which confer innate close interaction of the environment and many other infectious multi-drug resistance (MDR) to bacteria. The production of efflux diseases. With satellite sensors, these relationships were pumps can be increased, usually due to mutations in regulatory quantified and comparatively analyzed. More recent studies of genes, and this confers resistance to antibiotics that are often used epidemic diseases have provided models, both retrospective and to treat infections by Gram negative bacteria. RND MDR efflux prospective, for understanding and predicting disease epidemics, systems not only confer antibiotic resistance, but altered expression notably vector borne diseases. -

Exploring the Metastatic Role of the Inhibitor of Apoptosis BIRC6 in Breast Cancer
bioRxiv preprint doi: https://doi.org/10.1101/2021.04.08.438518; this version posted April 10, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 1 Exploring the metastatic role of the inhibitor of apoptosis BIRC6 in Breast 2 Cancer 3 Corresponding author: Matias Luis Pidre, Pringles 3010, Lanús, Buenos Aires, Argentina, CP 1824 4 [email protected], mobile: +54 9 221 364 6836 5 AUTHORS 6 Santiago M. Gómez Bergna1; Abril Marchesini1; Leslie C. Amorós Morales1; Paula N. Arrías1; Hernán 7 G. Farina2; Víctor Romanowski1; M. Florencia Gottardo2*; Matias L. Pidre1*. 8 *Both authors equally contributed to this work. 9 AUTHOR AFFILIATIONS 10 1Instituto de Biotecnología y biología molecular (IBBM-CONICET-UNLP) 11 2Center of Molecular & Translational Oncology, Department of Science and Technology, 12 National University of Quilmes, Buenos Aires, Argentina. 13 1 bioRxiv preprint doi: https://doi.org/10.1101/2021.04.08.438518; this version posted April 10, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 14 Abstract 15 Breast cancer is the most common cancer as well as the first cause of death by cancer in 16 women worldwide. BIRC6 (baculoviral IAP repeat-containing protein 6) is a member of the 17 inhibitors of apoptosis protein family thought to play an important role in the progression or 18 chemoresistance of many cancers. The aim of the present work was to investigate the role of 19 apoptosis inhibitor BIRC6 in breast cancer, focusing particularly on its involvement in the 20 metastatic cascade. -
2016 Joint Meeting Program
April 15 – 17, 2016 Fairmont Chicago Millennium Park • Chicago, Illinois The AAP/ASCI/APSA conference is jointly provided by Boston University School of Medicine and AAP/ASCI/APSA. Meeting Program and Abstracts www.jointmeeting.org www.jointmeeting.org Special Events at the 2016 AAP/ASCI/APSA Joint Meeting Friday, April 15 Saturday, April 16 ASCI President’s Reception ASCI Food and Science Evening 6:15 – 7:15 p.m. 6:30 – 9:00 p.m. Gold Room The Mid-America Club, Aon Center ASCI Dinner & New Member AAP Member Banquet Induction Ceremony (Ticketed guests only) (Ticketed guests only) 7:00 – 10:00 p.m. 7:30 – 9:45 p.m. Imperial Ballroom, Level B2 Rouge, Lobby Level How to Solve a Scientific Puzzle: Speaker: Clara D. Bloomfield, MD Clues from Stockholm and Broadway The Ohio State University Comprehensive Cancer Center Speaker: Joe Goldstein, MD APSA Welcome Reception & University of Texas Southwestern Medical Center at Dallas Presidential Address APSA Dinner (Ticketed guests only) 9:00 p.m. – Midnight Signature Room, 360 Chicago, 7:30 – 9:00 p.m. John Hancock Center (off-site) Rouge, Lobby Level Speaker: Daniel DelloStritto, APSA President Finding One’s Scientific Niche: Musings from a Clinical Neuroscientist Speaker: Helen Mayberg, MD, Emory University Dessert Reception (open to all attendees) 10:00 p.m. – Midnight Imperial Foyer, Level B2 Sunday, April 17 APSA Future of Medicine and www.jointmeeting.org Residency Luncheon Noon – 2:00 p.m. Rouge, Lobby Level 2 www.jointmeeting.org Program Contents General Program Information 4 Continuing Medical Education Information 5 Faculty and Speaker Disclosures 7 Scientific Program Schedule 9 Speaker Biographies 16 Call for Nominations: 2017 Harrington Prize for Innovation in Medicine 26 AAP/ASCI/APSA Joint Meeting Faculty 27 Award Recipients 29 Call for Nominations: 2017 Harrington Scholar-Innovator Award 31 Call for Nominations: George M. -

WO 2019/079361 Al 25 April 2019 (25.04.2019) W 1P O PCT
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization I International Bureau (10) International Publication Number (43) International Publication Date WO 2019/079361 Al 25 April 2019 (25.04.2019) W 1P O PCT (51) International Patent Classification: CA, CH, CL, CN, CO, CR, CU, CZ, DE, DJ, DK, DM, DO, C12Q 1/68 (2018.01) A61P 31/18 (2006.01) DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, C12Q 1/70 (2006.01) HR, HU, ID, IL, IN, IR, IS, JO, JP, KE, KG, KH, KN, KP, KR, KW, KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, (21) International Application Number: MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, PCT/US2018/056167 OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (22) International Filing Date: SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, 16 October 2018 (16. 10.2018) TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (25) Filing Language: English (84) Designated States (unless otherwise indicated, for every kind of regional protection available): ARIPO (BW, GH, (26) Publication Language: English GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, TZ, (30) Priority Data: UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, 62/573,025 16 October 2017 (16. 10.2017) US TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, ΓΕ , IS, IT, LT, LU, LV, (71) Applicant: MASSACHUSETTS INSTITUTE OF MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, SM, TECHNOLOGY [US/US]; 77 Massachusetts Avenue, TR), OAPI (BF, BJ, CF, CG, CI, CM, GA, GN, GQ, GW, Cambridge, Massachusetts 02139 (US). -

Characterization of the Cellular Network of Ubiquitin Conjugating and Ligating Enzymes Ewa Katarzyna Blaszczak
Characterization of the cellular network of ubiquitin conjugating and ligating enzymes Ewa Katarzyna Blaszczak To cite this version: Ewa Katarzyna Blaszczak. Characterization of the cellular network of ubiquitin conjugating and ligating enzymes. Cellular Biology. Université Rennes 1, 2015. English. NNT : 2015REN1S116. tel-01547616 HAL Id: tel-01547616 https://tel.archives-ouvertes.fr/tel-01547616 Submitted on 27 Jun 2017 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. ANNÉE 2015 THÈSE / UNIVERSITÉ DE RENNES 1 sous le sceau de l’Université Européenne de Bretagne pour le grade de DOCTEUR DE L’UNIVERSITÉ DE RENNES 1 Mention : BIOLOGIE École doctorale Vie-Agro-Santé présentée par Ewa Katarzyna Blaszczak Préparée à l’unité de recherche UMR 6290, IGDR Institut de Génétique et Développement de Rennes Université Rennes 1 Thèse soutenue à Rennes le 26.06.2015 Characterization of devant le jury composé de : Aude ECHALIER-GLAZER the cellular network Maître de conférence University of Leicester / rapporteur of ubiquitin Lionel PINTARD Directeur de recherche -

Yersinia Aldovae (Formerly Yersinia Enterocolitica-Like Group X2): a New Species of Enterobacteriaceae Isolated from Aquatic Ecosystems HERVE BERCOVIER,'T ARNOLD G
INTERNATIONALJOURNAL OF SYSTEMATICBACTERIOLOGY, Apr. 1984, p. 166-172 Vol. 34, No. 2 OO20-7713/84/020166-07$02.00/0 Yersinia aldovae (Formerly Yersinia enterocolitica-Like Group X2): a New Species of Enterobacteriaceae Isolated from Aquatic Ecosystems HERVE BERCOVIER,'t ARNOLD G. STEIGERWALT,2 ANNIE GUIYOULE,' GERALDINE HUNTLEY-CARTER,3 AND DON J. BRENNER2* Centre National des Yersinia, fnstitut Pasteur, 15724 Paris, Cedek 15, France,' and Molecular Biology Laboratory, Biotechnology Branch,2 and Enteric Laboratory Section, Enteric Diseases Branch13Division of Bacterial Diseases, Center for Infectious Diseases, Centers for Disease Control, Atlanta, Georgia 30333 Previously, a group of 40 Yersinia enterocolitica-like strains that were isolated from water and fish were called group X2. These strains produced acid from L-rhamnose, did not ferment sorbose, cellobiose, melibiose, or raffinose, and rarely fermented sucrose (5% in 48 h, 10% in 7 days). This pattern of reactions separated group X2 strains from Yersinia enterocolitica, Yersinia intermedia, Yersinia frederiksenii, and Yersinia kristensenii. Positive reactions for acetoin production (Voges-Proskauer test), ornithine decarbox- ylase, and lack of acid production from melibiose distinguished group X2 strains from both Yersinia pseudotuberculosis and Yersinia pestis. Group X2 strains exhibited variable reactions only in tests for citrate utilization, hydrolysis of Tween 80, and acid production from maltose. Genetically, group X2 strains formed a single deoxyribonucleic acid hybridization group with an average level of relatedness of 86% or more (86% as determined by the S1 method at 60°C or by the hydroxyapatite method at 75°C and 92% as determined by the hydroxyapatite method at 60°C). The level of divergence among related sequences in 60°C reactions was 0.5%, as determined by the hydroxyapatite method. -

UTR Shortening Is a Molecular Signature of Mtorc1 Activation
ARTICLE Received 22 Sep 2014 | Accepted 18 Apr 2015 | Published 15 Jun 2015 DOI: 10.1038/ncomms8218 mRNA 30-UTR shortening is a molecular signature of mTORC1 activation Jae-Woong Chang1,*, Wei Zhang2,*, Hsin-Sung Yeh1, Ebbing P. de Jong1, Semo Jun1, Kwan-Hyun Kim1, Sun S. Bae3, Kenneth Beckman4, Tae Hyun Hwang5, Kye-Seong Kim6, Do-Hyung Kim1, Timothy J. Griffin1, Rui Kuang2 & Jeongsik Yong1 Mammalian target of rapamycin (mTOR) enhances translation from a subset of messenger RNAs containing distinct 50-untranslated region (UTR) sequence features. Here we identify 30-UTR shortening of mRNAs as an additional molecular signature of mTOR activation and show that 30-UTR shortening enhances the translation of specific mRNAs. Using genetic or chemical modulations of mTOR activity in cells or mouse tissues, we show that cellular mTOR activity is crucial for 30-UTR shortening. Although long 30-UTR-containing transcripts minimally contribute to translation, 3-0UTR-shortened transcripts efficiently form polysomes in the mTOR-activated cells, leading to increased protein production. Strikingly, selected E2 and E3 components of ubiquitin ligase complexes are enriched by this mechanism, resulting in elevated levels of protein ubiquitination on mTOR activation. Together, these findings identify a previously uncharacterized role for mTOR in the selective regulation of protein synthesis by modulating 30-UTR length of mRNAs. 1 Department of Biochemistry, Molecular Biology and Biophysics, University of Minnesota Twin Cities, 321 Church Street, SE 6-155 Jackson Hall, Minneapolis, Minnesota 55455, USA. 2 Department of Computer Science and Engineering, University of Minnesota, Minneapolis, Minnesota 55455, USA. 3 Department of Pharmacology, Pusan National University School of Medicine, Yangsan 626-870, Republic of Korea. -

A Critical Role for A20 in -Cell Protection David Liuwantara,1 Mark Elliot,2 Mariya W
Nuclear Factor-B Regulates -Cell Death A Critical Role for A20 in -Cell Protection David Liuwantara,1 Mark Elliot,2 Mariya W. Smith,2 Andrew O. Yam,1 Stacy N. Walters,1 Eliana Marino,1 Andy McShea,2 and Shane T. Grey1 Apoptotic -cell death is central to the pathogenesis of and as the final effector mechanism (5,6). Evidence from type 1 diabetes and may be important in islet graft rejec- the NOD mouse (a widely studied model of autoimmune tion. Despite this, genetic control of -cell apoptosis is only diabetes) (7) indicates that autoreactive cytolytic T-cells poorly understood. We report that inhibition of gene tran- (8), as well as soluble mediators including proinflamma- scription sensitized -cells to tumor necrosis factor (TNF)- tory cytokines and free radicals, contribute to increased ␣–induced apoptosis, indicating the presence of a regulated -cell apoptotic destruction during the pathogenesis of antiapoptotic response. Using oligonucleotide microarrays type 1 diabetes (6,9). Transplantation of islets is consid- and real-time PCR, we identified TNFAIP3/A20 as the most ered to be one potential approach that could restore highly regulated antiapoptotic gene expressed in cytokine- stimulated human and mouse islets. Cytokine induction of normal metabolic control for the cure of type 1 diabetes. A20 mRNA in primary islets and insulinoma cells was rapid However, multiple obstacles are faced in islet transplants, and observed within 1 h, consistent with A20 being an including cellular rejection akin to the mechanisms in- immediate early response gene in -cells. Regulation of volved in autoimmune destruction of -cells, and also A20 was nuclear factor-B (NF-B)–dependent, two NF-B primary nonfunction, a phenomena related to lack of sites within the A20 promoter were found to be necessary nutrients, hypoxia, and nonspecific inflammatory media- and sufficient for A20 expression in -cells. -

Fish Bacterial Flora Identification Via Rapid Cellular Fatty Acid Analysis
Fish bacterial flora identification via rapid cellular fatty acid analysis Item Type Thesis Authors Morey, Amit Download date 09/10/2021 08:41:29 Link to Item http://hdl.handle.net/11122/4939 FISH BACTERIAL FLORA IDENTIFICATION VIA RAPID CELLULAR FATTY ACID ANALYSIS By Amit Morey /V RECOMMENDED: $ Advisory Committe/ Chair < r Head, Interdisciplinary iProgram in Seafood Science and Nutrition /-■ x ? APPROVED: Dean, SchooLof Fisheries and Ocfcan Sciences de3n of the Graduate School Date FISH BACTERIAL FLORA IDENTIFICATION VIA RAPID CELLULAR FATTY ACID ANALYSIS A THESIS Presented to the Faculty of the University of Alaska Fairbanks in Partial Fulfillment of the Requirements for the Degree of MASTER OF SCIENCE By Amit Morey, M.F.Sc. Fairbanks, Alaska h r A Q t ■ ^% 0 /v AlA s ((0 August 2007 ^>c0^b Abstract Seafood quality can be assessed by determining the bacterial load and flora composition, although classical taxonomic methods are time-consuming and subjective to interpretation bias. A two-prong approach was used to assess a commercially available microbial identification system: confirmation of known cultures and fish spoilage experiments to isolate unknowns for identification. Bacterial isolates from the Fishery Industrial Technology Center Culture Collection (FITCCC) and the American Type Culture Collection (ATCC) were used to test the identification ability of the Sherlock Microbial Identification System (MIS). Twelve ATCC and 21 FITCCC strains were identified to species with the exception of Pseudomonas fluorescens and P. putida which could not be distinguished by cellular fatty acid analysis. The bacterial flora changes that occurred in iced Alaska pink salmon ( Oncorhynchus gorbuscha) were determined by the rapid method. -

International Journal of Systematic and Evolutionary Microbiology (2016), 66, 5575–5599 DOI 10.1099/Ijsem.0.001485
International Journal of Systematic and Evolutionary Microbiology (2016), 66, 5575–5599 DOI 10.1099/ijsem.0.001485 Genome-based phylogeny and taxonomy of the ‘Enterobacteriales’: proposal for Enterobacterales ord. nov. divided into the families Enterobacteriaceae, Erwiniaceae fam. nov., Pectobacteriaceae fam. nov., Yersiniaceae fam. nov., Hafniaceae fam. nov., Morganellaceae fam. nov., and Budviciaceae fam. nov. Mobolaji Adeolu,† Seema Alnajar,† Sohail Naushad and Radhey S. Gupta Correspondence Department of Biochemistry and Biomedical Sciences, McMaster University, Hamilton, Ontario, Radhey S. Gupta L8N 3Z5, Canada [email protected] Understanding of the phylogeny and interrelationships of the genera within the order ‘Enterobacteriales’ has proven difficult using the 16S rRNA gene and other single-gene or limited multi-gene approaches. In this work, we have completed comprehensive comparative genomic analyses of the members of the order ‘Enterobacteriales’ which includes phylogenetic reconstructions based on 1548 core proteins, 53 ribosomal proteins and four multilocus sequence analysis proteins, as well as examining the overall genome similarity amongst the members of this order. The results of these analyses all support the existence of seven distinct monophyletic groups of genera within the order ‘Enterobacteriales’. In parallel, our analyses of protein sequences from the ‘Enterobacteriales’ genomes have identified numerous molecular characteristics in the forms of conserved signature insertions/deletions, which are specifically shared by the members of the identified clades and independently support their monophyly and distinctness. Many of these groupings, either in part or in whole, have been recognized in previous evolutionary studies, but have not been consistently resolved as monophyletic entities in 16S rRNA gene trees. The work presented here represents the first comprehensive, genome- scale taxonomic analysis of the entirety of the order ‘Enterobacteriales’.