Superior Orbital Fissure Syndrome of Uncertain Aetiology* Report of Ten Cases by A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Temporo-Mandibular Joint (Tmj) Dysfunction
Office: (310) 423-1220 BeverlyHillsENT.com Fax: (310) 423-1230 TEMPORO-MANDIBULAR JOINT (TMJ) DYSFUNCTION You may not have heard of it, but you use it hundreds of times every day. It is the Temporo- Mandibular Joint (TMJ), the joint where the mandible (the lower jaw) joins the temporal bone of the skull, immediately in front of the ear on each side of your head. You move the joint every time you chew or swallow. You can locate this joint by putting your finger on the triangular structure in front of your ear. Then move your finger just slightly forward and press firmly while you open your jaw all the way and shut it. The motion you feel is the TMJ. You can also feel the joint motion in your ear canal. These maneuvers can cause considerable discomfort to a patient who is having TMJ trouble, and physicians use these maneuvers with patients for diagnosis. TMJ Dysfunction can cause the following symptoms: Ear pain Sore jaw muscles Temple/cheek pain Jaw popping/clicking Locking of the jaw Difficulty in opening the mouth fully Frequent head/neck aches The pain may be sharp and searing, occurring each time you swallow, yawn, talk, or chew, or it may be dull and constant. It hurts over the joint, immediately in front of the ear, but pain can also radiate elsewhere. It often causes spasms in the adjacent muscles that are attached to the bones of the skull, face, and jaws. Then, pain can be felt at the side of the head (the temple), the cheek, the lower jaw, and the teeth. -

Clinical Indicators: Acoustic Neuroma Surgery
Clinical Indicators: Acoustic Neuroma Surgery Approach Procedure CPT Days1 Infratemporal post-auricular approach to middle cranial fossa 61591 90 Transtemporal approach to posterior cranial fossa 61595 90 Transcochlear approach to posterior cranial fossa 61596 90 Transpetrosal approach to posterior cranial fossa 61598 90 Craniectomy for cerebellopontine angle tumor 61520 90 Craniectomy, transtemporal for excision of cerebellopontine angle 61526 90 tumor Combined with middle/posterior fossa craniotomy/ 61530 90 craniectomy Definitive Procedure CPT Days Resection of neoplasm, petrous apex, intradural, including dural 61606 90 repair Resection of neoplasm, posterior cranial fossa, intradural, including 61616 90 repair Microdissection, intracranial 61712 90 Stereotactic radiosurgery 61793 90 Decompression internal auditory canal 69960 90 Removal of tumor, temporal bone middle fossa approach 69970 90 Repair Procedure CPT Days Secondary repair of dura for CSF leak, posterior fossa, by free tissue 61618 90 graft Secondary repair of dura for CSF leak, by local or regional flap or 61619 90 myocutaneous flap Decompression facial nerve, intratemporal; lateral to geniculate 69720 90 ganglion Total facial nerve decompression and/or repair (may include graft) 69955 90 Abdominal fat graft 20926 90 Fascia lata graft; by stripper 20920 90 Fascia lata graft; by incision and area exposure, complex or sheet 20922 90 Intraoperative Nerve Monitoring Procedure CPT Days Auditory nerve monitoring, setup 92585 90 1 RBRVS Global Days Intraoperative neurophysiology testing, hourly 95920 90 Facial nerve monitoring, setup 95925 90 Indications 1. History a) Auditory complaints • hearing loss • fullness • distorted sound perception b) Tinnitus • ringing • humming • hissing • crickets c) Disequilibrium • unsteadiness • dizziness • imbalance • vertigo d) Headache e) Fifth and seventh cranial nerve symptoms • facial pain • facial tingling, numbness • tics • weakness f) Family history of neurofibromatosis type II g) Diplopia h) Dysarthria, dysphasia, aspiration, hoarseness 2. -

Implications to Occipital Headache
The Journal of Neuroscience, March 6, 2019 • 39(10):1867–1880 • 1867 Neurobiology of Disease Non-Trigeminal Nociceptive Innervation of the Posterior Dura: Implications to Occipital Headache X Rodrigo Noseda, Agustin Melo-Carrillo, Rony-Reuven Nir, Andrew M. Strassman, and XRami Burstein Department of Anesthesia, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts 02115 Current understanding of the origin of occipital headache falls short of distinguishing between cause and effect. Most preclinical studies involving trigeminovascular neurons sample neurons that are responsive to stimulation of dural areas in the anterior 2/3 of the cranium and the periorbital skin. Hypothesizing that occipital headache may involve activation of meningeal nociceptors that innervate the posterior 1⁄3 of the dura, we sought to map the origin and course of meningeal nociceptors that innervate the posterior dura overlying the cerebellum. Using AAV-GFP tracing and single-unit recording techniques in male rats, we found that neurons in C2–C3 DRGs innervate the dura of the posterior fossa; that nearly half originate in DRG neurons containing CGRP and TRPV1; that nerve bundles traverse suboccipital muscles before entering the cranium through bony canals and large foramens; that central neurons receiving nociceptive information from the posterior dura are located in C2–C4 spinal cord and that their cutaneous and muscle receptive fields are found around the ears, occipital skin and neck muscles; and that administration of inflammatory mediators to their dural receptive field, sensitize their responses to stimulation of the posterior dura, peri-occipital skin and neck muscles. These findings lend rationale for the common practice of attempting to alleviate migraine headaches by targeting the greater and lesser occipital nerves with anesthetics. -

Livestock ID Product Catalog Int Ide Cover Ins Not Pr Do Table of Contents
Livestock ID Product Catalog INSIDE COVER DO NOT PRINT Table of Contents Z Tags Z1 No-Snag-Tag® Premium Tags .........................................02 Z Tags The New Z2 No-Tear-Tag™ System .....................................04 We’ve joined forces to bring you Temple Tag Herdsman® Two Piece Tags ........................................06 the best tags in the business. Z Tags Feedlot Tags..........................................................................08 Datamars is a worldwide leader in high-performance livestock identification Temple Tag Feeder Tags ...................................................................10 systems. With its state-of-the-art global manufacturing facilities and Temple Tag Original Tag .................................................................. 12 worldwide technical expertise, Datamars has added Temple Tag® and Z Tags® Temple Tag CalfHerder™ Tag ............................................................ 13 to the company’s global portfolio of world-class brands. Temple Tag FaStocker® Tag ..............................................................14 ComfortEar® Radio Frequency Identification Tags (RFID) ...........16 Datamars can bring you new and improved products faster than ever before. Temple Tag & Z Tags Taggers and Accessories .............................18 But one thing hasn’t changed, and that’s our unwavering commitment to America’s livestock producers. Temple Tag & Z Tags Custom Tag Decoration ..............................20 Temple Tag & Z Tags Hot Stamp Machines ................................... -

Human Sacrifice and Mortuary Treatments in the Great Temple of Tenochtitlán
FAMSI © 2007: Ximena Chávez Balderas Human Sacrifice and Mortuary Treatments in the Great Temple of Tenochtitlán Research Year: 2005 Culture: Mexica Chronology: Postclassic Location: México City, México Site: Tenochtitlán Table of Contents Introduction The bone collection in study Human sacrifice and mortuary treatments Methodology Osteobiography Tafonomic analysis Sacrifice by heart extraction Decapitation: Trophy skulls, Tzompantli skulls and elaboration of skull masks Skull masks Population analysis based upon DNA extraction Preliminary results Final considerations List of Figures Sources Cited Introduction The present report describes the study undertaken with the osteologic collection obtained from the Great Temple excavations in Tenochtitlán; this collection was assembled in the interval from 1978 to 2005. The financial support granted to us by FAMSI enabled the creation of four lines of research: 1) packing and preventive conservation; 2) osteobiography; 3) mortuary treatments; and 4) population genetics. Immediately, a detailed exposition of the work and its results up to the present moment will be given. Submitted 11/16/2006 by: Ximena Chávez Balderas [email protected] Figure 1. General view of the archaeological zone of the Great Temple in México City. 2 The bone collection in study For the present study the human remains found in 19 offerings in the Great Temple of Tenochtitlán were analyzed. This place symbolizes the axis mundi for the Mexicas. The deposits were temporarily situated in the period comprehended between 1440 and 1502 A.D., which corresponds mostly to stage IVb (1469-1481 A.D.). The total number of bodies studied was 1071. From these, seventy-four were recovered in the context of offerings and correspond to skull masks, decapitated skulls, tzompantli skulls, isolated remains and a primary context. -

Knowledge of Skull Base Anatomy and Surgical Implications of Human Sacrifice Among Pre-Columbian Mesoamerican Cultures
See the corresponding retraction, DOI: 10.3171/2018.5.FOCUS12120r, for full details. Neurosurg Focus 33 (2):E1, 2012 Knowledge of skull base anatomy and surgical implications of human sacrifice among pre-Columbian Mesoamerican cultures RAUL LOPEZ-SERNA, M.D.,1 JUAN LUIS GOMEZ-AMADOR, M.D.,1 JUAN BArgES-COLL, M.D.,1 NICASIO ArrIADA-MENDICOA, M.D.,1 SAMUEL ROMERO-VArgAS, M.D., M.SC.,2 MIGUEL RAMOS-PEEK, M.D.,1 MIGUEL ANGEL CELIS-LOPEZ, M.D.,1 ROGELIO REVUELTA-GUTIErrEZ, M.D.,1 AND LESLY PORTOCArrERO-ORTIZ, M.D., M.SC.3 1Department of Neurosurgery, Instituto Nacional de Neurologia y Neurocirugia “Manuel Velasco Suárez;” 2Department of Spine Surgery, Instituto Nacional de Rehabilitación; and 3Department of Neuroendocrinology, Instituto Nacional de Neurologia y Neurocirugia “Manuel Velasco Suárez,” Mexico City, Mexico Human sacrifice became a common cultural trait during the advanced phases of Mesoamerican civilizations. This phenomenon, influenced by complex religious beliefs, included several practices such as decapitation, cranial deformation, and the use of human cranial bones for skull mask manufacturing. Archaeological evidence suggests that all of these practices required specialized knowledge of skull base and upper cervical anatomy. The authors con- ducted a systematic search for information on skull base anatomical and surgical knowledge among Mesoamerican civilizations. A detailed exposition of these results is presented, along with some interesting information extracted from historical documents and pictorial codices to provide a better understanding of skull base surgical practices among these cultures. Paleoforensic evidence from the Great Temple of Tenochtitlan indicates that Aztec priests used a specialized decapitation technique, based on a deep anatomical knowledge. -
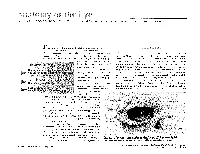
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Evisceration, Enucleation and Exenteration
CHAPTER 10 EVISCERATION, ENUCLEATION AND EXENTERATION This chapter describes three operations that either remove the contents of the eye (evisceration), the eye itself (enucleation) or the whole orbital contents (exenteration). Each operation has specific indications which are important to understand. In many cultures the removal of an eye, even if blind, is resisted. If an eye is very painful or grossly disfigured an operation will be accepted more readily. However, if the eye looks normal the patient or their family may be very reluctant to accept its removal. Therefore tact, compassion and patience are needed when recommending these operations. ENUCLEATION AND EVISCERATION There are several reasons why either of these destructive operations may be necessary: 1. Malignant tumours in the eye. In the case of a malignant tumour or suspected malignant tumour the eye should be removed by enucleation and not evisceration.There are two important intraocular tumours, retinoblastoma and melanoma and for both of them the basic treatment is enucleation. Retinoblastoma is a relatively common tumour in early childhood. At first the growth is confined to the eye. Enucleation must be carried out at this stage and will probably save the child’s life. It is vital not to delay or postpone surgery. If a child under 6 has a blind eye and the possibility of a tumour cannot be ruled out, it is best to remove the eye. Always examine the other eye very carefully under anaesthetic as well. It may contain an early retinoblastoma which could be treatable and still save the eye. Retinoblastoma spreads along the optic nerve to the brain. -

98796-Anatomy of the Orbit
Anatomy of the orbit Prof. Pia C Sundgren MD, PhD Department of Diagnostic Radiology, Clinical Sciences, Lund University, Sweden Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lay-out • brief overview of the basic anatomy of the orbit and its structures • the orbit is a complicated structure due to its embryological composition • high number of entities, and diseases due to its composition of ectoderm, surface ectoderm and mesoderm Recommend you to read for more details Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 3 x 3 Imaging technique 3 layers: - neuroectoderm (retina, iris, optic nerve) - surface ectoderm (lens) • CT and / or MR - mesoderm (vascular structures, sclera, choroid) •IOM plane 3 spaces: - pre-septal •thin slices extraconal - post-septal • axial and coronal projections intraconal • CT: soft tissue and bone windows 3 motor nerves: - occulomotor (III) • MR: T1 pre and post, T2, STIR, fat suppression, DWI (?) - trochlear (IV) - abducens (VI) Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Superior orbital fissure • cranial nerves (CN) III, IV, and VI • lacrimal nerve • frontal nerve • nasociliary nerve • orbital branch of middle meningeal artery • recurrent branch of lacrimal artery • superior orbital vein • superior ophthalmic vein Lund University / Faculty of Medicine / Inst. Clinical Sciences / Radiology / ECNR Dubrovnik / Oct 2018 Lund University / Faculty of Medicine / Inst. -

Surgical Anatomy of the Ligamentous Attachments in the Temple and Periorbital Regions
Cosmetic Surgical Anatomy of the Ligamentous Attachments in the Temple and Periorbital Regions Christopher J. Moss, M.B., B.S., F.R.A.C.S., Dip.Anat., Bryan C. Mendelson, F.R.C.S.(E), F.R.A.C.S., F.A.C.S., and G. Ian Taylor, F.R.C.S., F.R.A.C.S., M.D. Melbourne, Australia This study documents the anatomy of the deep attach- complex system of deep attachments that arise ments of the superficial fasciae within the temporal and from the underlying deep fascia/periosteum. periorbital regions. A highly organized and consistent three-dimensional connective tissue framework supports The subSMAS plane that contains these attach- the overlying skin and soft tissues in these areas. ments is therefore not always a simple cleavage The regional nerves and vessels display constant and plane. This explains why surgical dissection is predictable relationships with both the fascial planes and considerably more complicated in the midfa- their ligamentous attachments. Knowledge of these rela- tionships allows the surgeon to use the tissue planes and cial, temporal, and periorbital regions than in soft-tissue ligaments as intraoperative landmarks for the the scalp. vital neurovascular structures. This results in improved In the cheek, these deep attachments have efficiency and safety for aesthetic procedures in these been defined as the zygomatic, masseteric, and regions. (Plast. Reconstr. Surg. 105: 1475, 2000.) mandibular-cutaneous ligaments.21,22 These lig- aments provide a lateral line of fixation for the mobile tissues of the medial cheek. Release of The patterns of arrangement of the layers of these retaining ligaments is fundamental to the superficial fascia in the cheek,1–9 forehead,10–13 14 15,16 extended SMAS technique of “deep-plane” sur- scalp, and temple have been well de- 18,19,23,24 scribed. -

Where Is the Temporo-Mandibular Joint?
TMJ Insight into causes and treatments • How does the Temporo-Mandibular Joint work? • What causes TMJ pain? • How is TMJ pain treated? Open your jaw all the way and shut it. This simple movement would not be possible without the Temporo-Mandibular Joint (TMJ). It connects the temporal bone (the bone that forms the side of the skull) and the mandible (the lower jaw). Even though it is only a small disc of cartilage, it separates the bones so that the mandible may slide easily whenever you talk, swallow, chew, kiss, etc. Therefore, damage to this complex, triangular structure in front of your ear, can cause considerable discomfort. Where is the Temporo-Mandibular Joint? You can locate this joint by putting your finger on the triangular structure in front of your ear. Then move your finger just slightly forward and press firmly while you open your jaw all the way and close it. You can also feel the joint motion in your ear canal. How does the TMJ work? When you bite down hard, you put force on the object between your teeth and on the joint. In terms of physics, the jaw is the lever and the TMJ is the fulcrum. Actually, more force is applied (per square foot) to the joint surface than to whatever is between your teeth because the cartilage between the bones provides a smooth surface, over which the joint can freely slide with minimal friction. Therefore, the forces of chewing can be distributed over a wider surface in the joint space and minimize the risk of injury.