Measuring Volitional Competences: Psychometric Properties of a Short Form of the Volitional Components Questionnaire (VCQ) in a Clinical Sample
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Disorders of Volition Are Characterized by an Impairment Related to the Implementation of Decisions
1 Toward a Science of Volition Wolfgang Prinz, Daniel Dennett, and Natalie Sebanz This book aims at improving our understanding of the processes supporting volun- tary action by looking at conditions in which the will is impaired or even breaks down. We use this introductory chapter to prepare the ground for contributions by philoso- phers, psychologists, neuroscientists, and psychiatrists that tackle the experience of acting intentionally, the ability to make decisions and implement one’s goals, and the many ways in which the experience and the exertion of willful behavior can be dis- turbed. In the first part of this introduction, we describe the status of the will as we see it in present and past thinking. In the second part of the chapter, we provide an overview of the contributions in this book. 1.1 Studying the Will When trying to decipher the forbidding complexity of the mind/brain, the standard simplifying assumption is that it is an “input–output system” in which perception goes in and (control of) action eventually comes out. We experimenters then work from the outside in, first getting control and understanding of the peripheral input systems, and postponing difficult questions about the center, which is shrouded in fog and mystery. This makes sense but risks distorting our vision of the whole, since we seldom if ever find ways of even posing questions about the requirements for the more central components that must eventually get transformed into the highest levels of outbound or “inside-out” traffic. This potential for distortion is exacerbated by two further sources of distraction: introspection and the demands of free will. -

Cognitive Dissonance Theory Has Been Reformulated by Some Authors Since the Original Statement (Festinger, 1957) Ap- Peared in T
Japanese Psychological Research 1980, Vol.22, No.1, 32-41 ATTRIBUTION OF PERSONAL RESPONSIBILITY AND DISSONANCE REDUCTION HARUKI SAKAI AND KIYOSHI ANDOW 1 University of Tokyo The relationship between personal responsibility and dissonance reduction was investigated in a situation where an individual had to undergo a negative consequence caused by an agent beyond his control, i.e., by chance. Eighty participants received either strong or weak electric shock, depending on the oddness or evenness of spots of a die thrown either by the experimenter (Ex- perimenter-Caused condition) or by the participant himself (Participant- Caused condition). It was found that participants in the Participant-Caused condition evaluated electric shocks less painful, estimated their heart rates to be less faster, and perceived the experimenter more intelligent and favorable than participants in the Experimenter-Caused condition. These results were interpreted as lending support to the newly reformulated dissonance theory. Cognitive dissonance theory has been tion may be observed only to the degree reformulated by some authors since the that the individual sees himself as re- original statement (Festinger, 1957) ap- sponsible for bringing cognitions into an peared in the late 1950s. Brehm and inconsistent relationship (p. 10). Cohen (1962) stated that dissonance was These reformulations cited above clearly aroused only when an individual was concerned with the necessary conditions bound by a behavioral commitment to for dissonance arousal, and it may be said, one of the inconsistent cognitions. Aron- as Greenwald and Ronis (1978) pointed son (1968) stressed that the self concept or out, that dissonance theory has evolved some other firmly held expectancy must along a direction of convergence with be involved for dissonance to be aroused ideas from the tradition of self theory. -

Predicting Work Volition from Proactive Personality Trait Among University Students Üniversite Öğrencilerinin Proaktif Kişil
Kastamonu Üniversitesi Kastamonu University Kastamonu Eğitim Dergisi Kastamonu Education Journal Ocak 2018 Cilt:26 Sayı:1 January 2018 Volume:26 Issue:1 Kastamonu - TÜRKİYE Kastamonu - TURKEY Predicting Work Volition From Proactive Personality Trait Among University Students Üniversite Öğrencilerinin Proaktif Kişiliklerinin Çalışma İradesi Algısındaki Yordayıcı Rolü Hilal BÜYÜKGÖZEa aHacettepe Üniversitesi, Eğitim Fakültesi, Eğitim Bilimleri Bölümü, Ankara, Türkiye. Özet Abstract Bu araştırmada, üniversite öğrencilerinin çalışma iradesi düzeylerinin The current study aimed to elaborate on how work volition of university proaktif kişilik özellikleri ile ilişkisi ve proaktif kişiliğin çalışma iradesindeki students associated with proactive personality trait, and to what extent açıklama gücü belirlenmeye çalışılmıştır. Katılımcılar, 242’si kadın ve 110’u proactive personality predicted work volition. Participants consisted of erkek olmak üzere 352 üniversite öğrencisinden oluşmaktadır. Bulgular, erkek 352 university students including 242 females and 110 males. Findings katılımcıların kadınlara göre daha yüksek çalışma iradesine sahip olduğunu demonstrated that male university students had stronger work volition göstermiştir. Katılımcıların çalışma iradesi ve proaktif kişilik özelliği ile orta perceptions than female students. Further, a positive, moderate level düzeyde ve aynı yönlü bir ilişki olduğu belirlenirken, kariyer engeli algısı relationship between work volition and proactive personality was explored, ile proaktif kişilik arasında -
On Consciousness As a Sense a Communication of the Intractable Studies Institute Patrick M
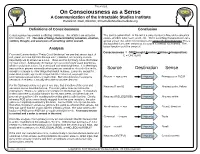
Theoretical. On Consciousness as a Sense A Communication of the Intractable Studies Institute Patrick M. Rael, Director, IntractableStudiesInstitute.org SM SM Definitions of Consciousness Conclusion Consciousness has several conflicting definitions. The definition we will solve This can be generalized: In the mind, a sensory neuron fires and a sensation here includes: def - The state of being characterized by sensation, emotion, occurs, whether color, taste, smell, etc. There is nothing that would rule out a volition, thought, and awareness of something within oneself. special sensor that when fired produces the sense of consciousness! This is distinguished from other senses as it’s source is internal, not external. The logical function could be sense of: Analysis Consciousness = OR(Thought,Emotion,Volition,Introspection) From the Communication “Pretty Good Sentience” we see that sensor input of C = OR(TEVI) red, green and blue light into the eye are 1) detected, and equally or more importantly are 2) sensed as a color. These are the 3 primary colors the human eye can sense. Additionally the human eye can sense night vision brightness, which mostly lacks colors, it’s more black and white brightness. It is seemingly impossible to present externally what a persons sensation of a color like red is, Source Destination Sense except to compare to other things that match redness. Everyone, except for color-blind people, agrees the crayon labeled red is red, so people can communicate sensed colors to each other. But nobody knows if a persons Photon → eye cone Neuron(s) Primary color R,G,B sensation of redness is actually the same as another persons. -
Spontaneous Hypnosis in the Ÿ Or En Sic Context
Spontaneous Hypnosis in the ÿ or en sic Context John 0.Beahrs, MD "Hypnosis" denotes either specific phenomena (altered volition, perception, cog- nition, and recall) or interpersonal transactions that often elicit them. Basic research leads to paradox: hypnosis is validated, and shown to be dissociative in essence, at the same time that neither its phenomena nor transactions can be separated from those of everyday living without logical absurdity. This paradox can be resolved by assuming that consciousness and volition are complex, occurring simultaneously at many levels in the same waking individual. Hypnotic-like phenomena and transac- tions occur spontaneously, in either covert or overt forms. The former are pervasive, whereas the latter are often associated with psychological trauma. Forensic impli- cations are twofold: for criminal responsibility, and the reliability of eyewitness testimony. Hypnotic-like states and transactions are rarely affirmed as an insanity defense because at some level these subjects are aware of what they are doing and why. Diminished capacity and mitigation of sentence are more appropriate defense strategies. Several conflicted traditions of case law have evolved to protect eyewitness testimony from hypnotic-like distortions in cognition, perception, and memory that can occur either during or outside of formal hypnotic procedures. These include the admissibility of posthypnotic testimony, due process safeguards at eyewitness identification procedures, and the admissibility of expert testimony on the findings of eyewitness research. These areas are inseparable from one another and demand a systematic coordinated approach. The word "hypnosis" is used to denote nomena include a shift toward either certain unexplained phenomena, subjective nonvolition (a hand "just interpersonal transactions that often lifts"), altered perception that can in- elicit them, or a formal ritualistic pro- clude positive and negative hallucina- cedure. -

Volition in Prospective Memory 1 Title: Volition in Prospective
Volition in Prospective Memory Title: Volition in Prospective Memory: evidence against differences in recalling free and fixed delayed intentions Authors: Mikkel C. Vinding 1) Jonas Kristoffer Lindeløv 2,3) Yahui Xiao 4,5,6) Raymond C. K. Chan 4,5,6) Thomas Alrik Sørensen 2,3,4) Affiliations: 1) NatMEG, Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden 2) CNRU, CFIN, Health, Aarhus University, Aarhus, Denmark. 3) Centre for Cognitive Neuroscience, Department of Communication and Psychology, Aalborg University, Aalborg, Denmark. 4) Sino-Danish Center for Education and Research, Aarhus, Denmark & Beijing, China. 5) Neuropsychology and Applied Cognitive Neuroscience Laboratory, CAS Key Laboratory of Mental Health, Institute of Psychology, Chinese Academy of Sciences, Beijing, China. 6) Department of Psychology, University of Chinese Academy of Sciences, Beijing, China. Contact information: Mikkel C. Vinding Department of Clinical Neuroscience Karolinska Institutet Nobels väg 9, D3 171 77 Stockholm Sweden Email: [email protected] 1 Volition in Prospective Memory 1 Abstract 2 Human volition can be defined as the extent to which actions are generated by internal states or as a response 3 to externally dictated instructions. Whether actions are voluntary or not influence the cognitive process of 4 action generation and perception of action. The influence of volition on deciding actions at a later point in time 5 is a less explored dimension. A voluntary decision on future action requires that the intention must be stored in 6 the prospective memory until the intended action is performed. It is unknown if the distinction between freely 7 chosen actions and externally dictated actions has a cognitive relevance for delayed intentions. -
GRC 2012 Ings Graduate Research Conference Electrical and Computer Engineering Roceed P Rence E Conf
ECE-GRC 2012 ings Graduate Research Conference Electrical and Computer Engineering roceed P rence e Conf April 27th, 2012 Hilton UH Hotel & Conference Center University of Houston Conference Committee General Chair Conference Coordination Financial Committee: Judging Committee: Dr. Pauline Markenscoff MyTrang Baccam Dr. Steven Pei Chair Dr. David Jackson Monica Sanchez Dr. Ben Jansen Dr. Jiming Bao Technical Committee: Communications Committee: Local Arrangements Committee: Dr. Wanda Wosik Chair Dr. Bhavin Sheth Chair Dr. Ji Chen Chair Sohini Sengupta Ruoli Jiang Anthony Lau Nitin Kushawaha Printing is provided by Texas Learning & Computation Center The 2012 CDC/GRC gratefully acknowledges generous support received from our sponsors 8th Annual Graduate Research Conference April 27, 2012 c apstone D esign The Hilton UH Hotel & Conference Center onference Houston, Texas c Program 8:00 - 8:55 am Breakfast and registration, Waldorf Astoria Room 210, Lobby 8:55 - 9:00 am Opening Ceremonies, Plaza Room 247 • Opening Remarks by Dr. Pauline Markenscoff, Conference Chair • Welcome to Technical Sessions by Dr. Wanda Wosik 9:00 - 10:00 am Technical Program - Oral Session A, Plaza Room 247 10:00 - 10:30 am Remarks by • Dr. Rathindra Bose, VC/VP for Research and Technology Transfer • Dr. Badri Roysam, Chairman, ECE Department 10:30 - 10:45 am Coffee Break, Waldorf Astoria Room 210, Lobby 10:45 - 11:30 am Technical Program - Oral Session B, Plaza Room 247 11:30 - 12:30 pm Lunch, Waldorf Astoria Room 210 12:30 - 1:00 pm Plenary Presentation, Dr. Stefan -

Consciousness Science and Its Theories Spontaneous Perception
Neuroscience of Consciousness, 2021, 7(2), 1–11 DOI: https://doi.org/10.1093/nc/niab016 Review Article Special Issue: Consciousness science and its theories Spontaneous perception: a framework for task-free, self-paced perception Downloaded from https://academic.oup.com/nc/article/2021/2/niab016/6338412 by guest on 04 August 2021 Shira Baror1 and Biyu J. He1,2,*,† 1Neuroscience Institute, New York University School of Medicine, 435 E 30th Street, New York, NY 10016, USA;2Departments of Neurology, Neuroscience & Physiology, Radiology, New York University School of Medicine, 435 E 30th Street, New York, NY 10016, USA †Biyu J. He, http://orcid.org/0000-0003-1549-1351 *Correspondence address. Neuroscience Institute, New York University School of Medicine, 435 E 30th Street, New York, NY 10016, USA. E-mail: [email protected] Abstract Flipping through social media feeds, viewing exhibitions in a museum, or walking through the botanical gardens, people consistently choose to engage with and disengage from visual content. Yet, in most laboratory settings, the visual stimuli, their presentation dura- tion, and the task at hand are all controlled by the researcher. Such settings largely overlook the spontaneous nature of human visual experience, in which perception takes place independently from specific task constraints and its time course is determined bythe observer as a self-governing agent. Currently, much remains unknown about how spontaneous perceptual experiences unfold in the brain. Are all perceptual categories extracted during spontaneous perception? Does spontaneous perception inherently involve volition? Is spontaneous perception segmented into discrete episodes? How do different neural networks interact over time during spontaneous perception? These questions are imperative to understand our conscious visual experience in daily life. -
Essays on Colour
Essays on Colour ESSAYS ON COLOUR A collection of columns from Cabinet Magazine Eleanor Maclure Introduction For every issue the editors of Cabinet Magazine, an American quarterly arts and culture journal, ask one of their regular contributors to write about a specific colour. The essays are printed as Cabinet’s regular Colours Column. To date, forty-two different colours have been the subject of discussion, beginning with Bice in their first ever issue. I first encountered Cabinet magazine when I stumbled upon Darren Wershler-Henry’s piece about Ruby, on the internet. I have since been able to collect all of the published columns and they have provided a wealth of knowledge, information and invaluable research about colour and colour names. Collectively, the writings represent a varied and engaging body of work, with approaches ranging from the highly factual to the deeply personal. From the birth of his niece in Matthew Klam’s Purple, to a timeline of the history of Lapis Lazuli mining in Ultramarine by Matthew Buckingham, the essays have provided fascinating insights into a whole range of colours, from basic terms such as black and red, to the more obscure: porphyry and puce. While some focus very much on the colour in question, others diverge into intricate tales of history, chemistry or geopolitics. There are personal anecdotes, legends and conspiracies, but more than that, the essays demonstrate the sheer diversity of ways we can talk about colour. The essays gathered here have become far more than just the background reading they began as. The aim of this book is to bring together the works, as a unique representation of the different ways we relate to, experience and interpret colours. -

Laminar Cortical Dynamics of Cognitive and Motor Working Memory, Sequence Learning and Performance: Toward a Unified Theory of How the Cerebral Cortex Works
Laminar Cortical Dynamics of Cognitive and Motor Working Memory, Sequence Learning and Performance: Toward a Unified Theory of How the Cerebral Cortex Works Stephen Grossberg1 and Lance R. Pearson2* Department of Cognitive and Neural Systems Center for Adaptive Systems1 and Center of Excellence for Learning in Education, Science, and Technology 677 Beacon Street Boston University Boston, MA 02215 617-353-7858 (Phone) 617-353-7755 (Fax) [email protected] http://www.cns.bu.edu/Profiles/Grossberg Department of Psychology2 Vanderbilt University 111 21st Avenue South Nashville, TN 37203 502-741-6493 (Phone) [email protected] Corresponding Author: Stephen Grossberg Technical Report CAS/CNS TR-08-002 Submitted: April, 2006 Running Title: Cortical Working Memory and Sequence Learning Key words: working memory, competitive queuing, immediate serial recall, immediate free recall, delayed free recall, continuous-distracter free recall, sensory-motor imitation, chunking, sequence learning, prefrontal cortex, parietal cortex, position coding, rank order cells, cerebral cortex, laminar computing * Authors are listed in alphabetical order. 1 Supported in part by the National Science Foundation (NSF SBE-0354378) and the Office of Naval Research (ONR N00014-01-1-0624). 2 Supported in part by the Air Force Office of Scientific Research (AFOSR F49620-01-1- 0397), the National Science Foundation (NSF SBE-0354378), and the Office of Naval Research (ONR N00014-95-1-0409 and ONR N00014-01-1-0624). Present address: Department of Psychology, Vanderbilt University, 111 21st Avenue South, Nashville, TN 37203 ABSTRACT How does the brain carry out working memory storage, categorization, and voluntary performance of event sequences? The LIST PARSE neural model proposes an answer to this question that unifies the explanation of cognitive, neurophysiological, and anatomical data from humans and monkeys. -

11 Contemplative Neuroscience As an Approach to Volitional Consciousness
Nancey Murphey, George F.R. Ellis, and Timothy O'Conner, eds., Downward Causation and the Neurobiology of Free Will (Springer, 2009), pp. 187-197. 11 Contemplative Neuroscience as an Approach to Volitional Consciousness Evan Thompson Department of Philosophy University of Toronto 170 St. George Street, 4th floor Toronto, ON M5R 2M8 Canada [email protected] Summary. This chapter presents a methodological approach to volitional consciousness for cognitive neuroscience based on studying the voluntary self- generation and self-regulation of mental states in meditation. Called contemplative neuroscience, this approach views attention, awareness, and emotion regulation as flexible and trainable skills, and works with experimental participants who have undergone training in contemplative practices designed to hone these skills. Drawing from research on the dynamical neural correlates of contemplative mental states and theories of large-scale neural coordination dynamics, I argue for the importance of global system causation in brain activity and present an “interventionist” approach to intentional causation. Key words: volition, consciousness, neurodynamics, neurophenomenology, contemplative neuroscience, meditation. In this chapter I sketch a methodological approach to volitional consciousness for cognitive neuroscience based on studying the voluntary self-generation and self- regulation of mental states in meditation. Called contemplative neuroscience, this approach views attention, awareness, and emotion regulation as flexible and train- able skills, and works with experimental participants who have undergone exten- sive training in contemplative practices designed to hone these skills. My discus- sion here is premised on the following three working assumptions (Lutz et al. 2007; Lutz et al. 2008): 188 Evan Thompson • Advanced contemplative practitioners can generate new data that would not exist without contemplative mental training. -
Best Practices for Graphic Designers, Color Works
Best Practices for Graphic Designers Color Works Best Practices for Graphic Designers Color Works An Essential Guide to Understanding and Applying Color Design Principles Eddie Opara John Cantwell Contents Foreword 006 Chapter 04 Production & Information Chromatophobia by Michael Bierut Preface 008 4.0 Overview 093 Speaking the Language of Color 4.1 Eye on Print: Simon Esterson 094 by Eddie Opara 4.2 Living Print: Gael Towey 100 4.3 Pantone: Systems of Color 106 Chapter 01 Context 4.4 Infographics and Color: Jacques Bertin 114 4.5 Wayfinding and Color: Cartlidge Levene 122 1.0 Overview 011 1.1 Black and White: 012 Hjalti Karlsson and Jan Wilker Chapter 05 Clients & The Subjective 1.2 Color and Space: Morag Myerscough 016 1.3 Craftsmanship of Color: 022 5.0 Overview 129 The Dutch Guilder 5.1 Tiffany & Co.: Paula Scher 130 1.4 Concept and Color: Tony Brook 028 5.2 Changing Big Blue: IBM 134 1.5 Color and Tradition: Lufthansa 034 5.3 Color and Flexible Form: Swisscom 140 5.4 Breaking from the Pack: Mohawk Paper 146 5.5 The Color Subjective: Stefan Sagmeister 150 Chapter 02 Awareness 2.0 Overview 041 Chapter 06 The Foundation 2.1 Color in Branding 1: Brian Collins 042 2.2 Color in Branding 2: Michael Rock 048 6.0 Overview 157 2.3 Branding Large Events with Color: 054 6.1 The Art of Seeing: Perceptions of Color 158 The 1972 and 2012 Olympics 6.2 The Cultural Significance of Color 162 2.4 A City’s Colors: Willy Wong 062 6.3 Wheel of Fortune and Color Systems 168 2.5 Saving Lives with Color: 068 6.4 Chroma and the Chromatics 174 Deborah Adler 6.5 Relativity and Reactivity of Color 180 6.6 Dimension in Color 184 Chapter 03 The Digital Color Lexicon 188 3.0 Overview 075 About the Authors 192 3.1 The Future of Color: Adobe Kuler 076 Contributors 192 3.2 Color in Motion: Matt Pyke 082 3.3 The Color of the News: Kojo Boateng 086 How to use this book Each chapter has its own icon which is used to cross-reference other related parts of the book.