Episcleritis and Scleritis: Unlocking the Differences
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Eyelid and Orbital Infections
27 Eyelid and Orbital Infections Ayub Hakim Department of Ophthalmology, Western Galilee - Nahariya Medical Center, Nahariya, Israel 1. Introduction The major infections of the ocular adnexal and orbital tissues are preseptal cellulitis and orbital cellulitis. They occur more frequently in children than in adults. In Schramm's series of 303 cases of orbital cellulitis, 68% of the patients were younger than 9 years old and only 17% were older than 15 years old. Orbital cellulitis is less common, but more serious than preseptal. Both conditions happen more commonly in the winter months when the incidence of paranasal sinus infections is increased. There are specific causes for each of these types of cellulitis, and each may be associated with serious complications, including vision loss, intracranial infection and death. Studies of orbital cellulitis and its complication report mortality in 1- 2% and vision loss in 3-11%. In contrast, mortality and vision loss are extremely rare in preseptal cellulitis. 1.1 Definitions Preseptal and orbital cellulites are the most common causes of acute orbital inflammation. Preseptal cellulitis is an infection of the soft tissue of the eyelids and periocular region that is localized anterior to the orbital septum outside the bony orbit. Orbital cellulitis ( 3.5 per 100,00 ) is an infection of the soft tissues of the orbit that is localized posterior to the orbital septum and involves the fat and muscles contained within the bony orbit. Both types are normally distinguished clinically by anatomic location. 1.2 Pathophysiology The soft tissues of the eyelids, adnexa and orbit are sterile. Infection usually originates from adjacent non-sterile sites but may also expand hematogenously from distant infected sites when septicemia occurs. -

Department of Ophthalmology Medical Faculty of Padjadjaran University Cicendo Eye Hospital, the National Eye Center Bandung
1 DEPARTMENT OF OPHTHALMOLOGY MEDICAL FACULTY OF PADJADJARAN UNIVERSITY CICENDO EYE HOSPITAL, THE NATIONAL EYE CENTER BANDUNG Case report : Clinical features and Diagnosis of Neuromyelitis Optica Spectrum Disorder (NMOSD) Presenter : Lucy Nofrida Siburian Supervisor : DR. Bambang Setiohaji, dr., SpM(K)., MH.Kes Has been reviewed and approved by supervisor of neuro-ophthalmology unit DR. Bambang Setiohaji, dr., SpM(K)., MH.Kes Friday, August 04, 2017 07.00 am 2 Abstract Introduction : Neuromyelitis optica spectrum disorder (NMOSD), previously known as Devic’s disease, is an inflammatory CNS syndrome distinct from multiple sclerosis (MS). It is characterized by severe, immune-mediated demyelination and axonal damage predominantly targeting the optic nerves and spinal cord though rarely the brain is also involved. Most patients with NMO and many with NMOSD have autoantibodies against the water channel aquaporin-4(AQP4-Ab), which are thought to be pathogenic. However, some patients are seronegative for AQP4-Abs and the lack of a biomarker makes diagnosis and management of these patients difficult. Aim : To present an NMO case and to know the current diagnosis criteria of NMOSD Case report : A woman, 42 years old, came to neuro-ophthalmology unit of Cicendo eye hospital on March 14, 2017 with sudden blurred vision on the right eye (RE) two days before admission without eye movement pain. Physical examination and body weight were normal. Visual acuity (VA) of the right eye (RE) was 1/300 and the best corrected VA on the left eye was 1.0. Anterior segment on the RE showed relative afferent pupillary defect grade 3 (RAPD), others were normal and so is on the LE. -

Diagnosing, Treating, and Managing Scleritis in 2020 an Expert Panel Recommendation Panel Members Melissa Toyos, Md Stephen D
DIAGNOSING, TREATING, AND MANAGING SCLERITIS IN 2020 AN EXPERT PANEL RECOMMENDATION PANEL MEMBERS MELISSA TOYOS, MD STEPHEN D. ANESI, MD, FACS n Partner and Director of Research n Massachusetts Eye Research & Surgery Institution n Toyos Clinic n Waltham, MA n Nashville, TN DAVID S. CHU, MD n Medical Director, Metropolitan Eye Research THOMAS A. ALBINI, MD & Surgery Institute n Professor of Clinical Ophthalmology n Associate Professor of Clinical Ophthalmology n University of Miami Health n Rutgers University n Bascom Palmer Eye Institute n Newark, NJ n Miami, FL ROBERT C. WANG, MD n Texas Retina Associates n Dallas, TX Corresponding Author: Melissa Toyos, MD; Toyos Clinic, Nashville, TN; [email protected]. This work was supported by an unrestricted medical writing grant from Mallinckrodt Pharmaceuticals and is based on a virtual roundtable discussion hosted by Evolve Medical Education LLC. Although uncommon, scleritis is a dangerous immune-me- DIAGNOSING SCLERITIS diated disease that can potentially threaten the structural Melissa Toyos, MD: What percentage of patients in integrity of the eye and may be indicative of potentially your practice have scleritis? life-threatening systemic vasculitis.1,2 Data on the genetic factors of scleritis is lacking, but it is thought that genes affect- Stephen D. Anesi, MD, FACS: Scleritis accounts for 10% ing systemic autoimmune diseases impact scleritis as well.2 to 15% of the patients I see in my practice. Differentiating between episcleritis and scleritis and posterior and anterior scleritis can be challenging for physicians. An David S. Chu, MD: I agree; 10% to 15% sounds right to accurate diagnosis is critical to properly treat the disease and me as well. -

Contrast Sensitivity Function in Graves' Ophthalmopathy and Dysthyroid Optic Neuropathy Br J Ophthalmol: First Published As 10.1136/Bjo.77.11.709 on 1 November 1993
Britishjournal ofOphthalmology 1993; 77: 709-712 709 Contrast sensitivity function in Graves' ophthalmopathy and dysthyroid optic neuropathy Br J Ophthalmol: first published as 10.1136/bjo.77.11.709 on 1 November 1993. Downloaded from Maria S A Suttorp-Schulten, Rob Tijssen, Maarten Ph Mourits, Patricia Apkarian Abstract defocus greatly facilitates the process of subjec- Contrast sensitivity function was measured by tive refraction correction, but reduced contrast a computer automated method on 38 eyes with sensitivity at low spatial frequencies may present dysthyroid optic neuropathy and 34 eyes with with normal Snellen acuity. As there are various Graves' ophthalmopathy only. The results degrees ofvisual loss within the group ofpatients were compared with 74 healthy control eyes. with dysthyroid neuropathy, assessment of Disturbances of contrast sensitivity functions spatial vision across the frequency and contrast were found in both groups when compared with spectrum may reveal visual impairment not controls. The eyes affected with dysthyroid readily detected by standard visual acuity optic neuropathy showed pronounced loss of measures. contrast sensitivity in the low frequency range, The contrast sensitivity function has proved a which facilitates differentiation between the useful tool for detecting visual disturbances two groups. when Snellen acuity fails to show comparable (BrJ Ophthalmol 1993; 77: 709-712) dysfunction - for example, in glaucoma,'4 retinal disease,'516 and pterygia." The clinical potential for contrast sensitivity functions has also been Graves' ophthalmopathy is related to thyroid demonstrated in patients with optic neuro- disease and is characterised by oedema and pathies, " 2"02' including dysthyroid optic neuro- infiltration ofthe extraocular muscles and orbital pathy."22 This study compares the contrast tissue. -

Preseptal and Orbital Cellulitis
Journal of Microbiology and Infectious Diseases / 2014; 4 (3): 123-127 JMID doi: 10.5799/ahinjs.02.2014.03.0154 REVIEW ARTICLE Preseptal and orbital cellulitis Emine Akçay, Gamze Dereli Can, Nurullah Çağıl Yıldırım Beyazıt Univ. Medical Faculty Atatürk Training and Research Hospital Dept. of Ophthalmology, Ankara, Turkey ABSTRACT Preseptal cellulitis (PC) is defined as an inflammation of the eyelid and surrounding skin, whereas orbital cellulitis (OC) is an inflammation of the posterior septum of the eyelid affecting the orbit and its contents. Periorbital tissues may become infected as a result of trauma (including insect bites) or primary bacteremia. Orbital cellulitis generally occurs as a complication of sinusitis. The most commonly isolated organisms are Staphylococcus aureus, Streptococcus pneu- moniae, S. epidermidis, Haempphilus influenzae, Moraxella catarrhalis and S. pyogenes. The method for the diagnosis of OS and PS is computed tomography. Using effective antibiotics is a mainstay for the treatment of PC and OC. There is an agreement that surgical drainage should be performed in cases of complete ophthalmoplegia or significant visual impairment or large abscesses formation. This infections are also at a greater risk of acute visual loss, cavernous sinus thrombosis, meningitis, cerebritis, endo- phthalmitis, and brain abscess in children. Early diagnosis and appropriate treatment are crucial to control the infection. Diagnosis, treatment, management and complications of PC and OC are summarized in this manuscript. J Microbiol Infect Dis 2014; 4(3): 123-127 Key words: infection, cellulitis, orbita, preseptal, diagnosis, treatment Preseptal ve Orbital Sellülit ÖZET Preseptal selülit (PS) göz kapağı ve çevresindeki dokunun iltihabi reaksiyonu iken orbital selülit (OS) orbitayı ve onun içeriğini etkileyen septum arkası dokuların iltihabıdır. -

CAUSES, COMPLICATIONS &TREATMENT of A“RED EYE”
CAUSES, COMPLICATIONS & TREATMENT of a “RED EYE” 8 Most cases of “red eye” seen in general practice are likely to be conjunctivitis or a superficial corneal injury, however, red eye can also indicate a serious eye condition such as acute angle glaucoma, iritis, keratitis or scleritis. Features such as significant pain, photophobia, reduced visual acuity and a unilateral presentation are “red flags” that a sight-threatening condition may be present. In the absence of specialised eye examination equipment, such as a slit lamp, General Practitioners must rely on identifying these key features to know which patients require referral to an Ophthalmologist for further assessment. Is it conjunctivitis or is it something more Iritis is also known as anterior uveitis; posterior uveitis is serious? inflammation of the choroid (choroiditis). Complications include glaucoma, cataract and macular oedema. The most likely cause of a red eye in patients who present to 4. Scleritis is inflammation of the sclera. This is a very rare general practice is conjunctivitis. However, red eye can also be presentation, usually associated with autoimmune a feature of a more serious eye condition, in which a delay in disease, e.g. rheumatoid arthritis. treatment due to a missed diagnosis can result in permanent 5. Penetrating eye injury or embedded foreign body; red visual loss. In addition, the inappropriate use of antibacterial eye is not always a feature topical eye preparations contributes to antimicrobial 6. Acid or alkali burn to the eye resistance. The patient history will usually identify a penetrating eye injury Most general practice clinics will not have access to specialised or chemical burn to the eye, but further assessment may be equipment for eye examination, e.g. -

A Case of Very Limited Wegener's Granulomatosis and Scleritis
A Case of Very Limited Wegener's Granulomatosis and Scleritis Jean Yang, M.D. Case Presentation: The patient is a 75 year old man who underwent cataract extraction of the right eye in March 93. The surgery was uneventful. A year and half later, the patient developed a large, rapidly advancing conjunctival mass medially in the right eye. Biopsy of the lesion revealed chronic inflammation. The right eye was treated with topical dexamethasone/neomycin/polytrim without any improvement. The patient was referred in August this year. The past medical history was significant for hypertension. Review of systems was significant for fatigue. On examination, the visual acuity was counting fingers at 3 ft OD, and 20/30 OS. The biomicroscopic examination showed a large conjunctival mass superonasally as seen below. There was diffuse conjunctival injection and inflammation. Conjunctiva inferotemporally also appeared to be elevated as seen in the figure below. Superiorly, a corneal pannus was also noted. The rest of the exam and the exam of the left eye was unremarkable. An immunologic workup included a negative ANCA, an erythrocyte sedimentation rate of 65, mildly elevated soluble IL-2 receptor level at 894, and ANA with rat liver subtrate of 1:80. Urinalysis was positive for glucose, but negative for RBC. The rest of the workup including a chest X-ray, CBC, FTA-abs, RPR, rheumatoid factor, and immune complex assays were all negative. The patient underwent conjunctival and scleral biopsy of the right eye. Intraoperatively, after the conjunctiva was lifted, multiple scleral nodules were noted. Histopathology of the specimen revealed probable vasculitis with micro-abscesses, seen below, with epithelioid cells and eosinophils seen further below, suggestive of Wegener's granulomatosis. -

Red Eye Sub-Conjunctival Hemorrhage
AEP Course 1 Friday 1:00 - 2:00 pm Disclosures Red Eye • Consultant for Alcon Cecelia Koetting, OD FAAO Virginia Eye Consultants Norfolk, VA VOA Conference Norfolk 2018 Nothing makes the office more Multiple Causes of “Red Eye” nervous than when this walks in. • Sub-Conjunctival hemorrhage • Allergic Conjunctivitis • Viral Conjunctivitis • Bacterial Conjunctivitis • Episcleritis • Scleritis • Ocular Surface Disease How to Triage Sub-Conjunctival • On the phone • Get as much information as possible about which eye, Hemorrhage when, how, recent surgeries, recent trauma and what medications have been used • In the room • Gather the same information as well as details on symptoms • Help to avoid possible spread of bacterial and viral conjunctivitis 1 AEP Course 1 Friday 1:00 - 2:00 pm Causes • Straining from: • Broken blood vessel releasing blood into the • Coughing • Vomiting surrounding sub conjunctival tissue • Constipation • A bruise • Diarrhea • Lifting • More common in patients on blood thinners • Sneezing • Bruise more easily and will take longer to resolve • Rubbing the eyes • Contact lens • Severe dryness • Trauma, surgery, injections • Blood clotting disorders and blood thinners • Occasionally, high blood pressure High BP • Remember to ask if the patient is on blood thinners or blood pressure meds Allergic Conjunctivitis • Last time took BP meds • Possibly check BP in office if haven't taken • Inflammation in the lining of the conjunctiva from allergies • IgE and Mast Cell release • Symptoms: itching, redness, tearing, foreign body -

Postoperative Eye Protection After Cataract Surgery Anterior Uveitis Responds to Ganciclovir, but the Relapse Rate Is High and Prolonged Therapy May Be Required
Correspondence 1152 Sir, 4 Ioannidis AS, Bacon J, Frith P. Juxtapapillary cytomegalovirus Cytomegalovirus and Eye retinitis with optic neuritis. J Neuroophthalmol 2008; 28(2): 128–130. 5 Mansour AM. Cytomegalovirus optic neuritis. Curr Opin We read with interest the very comprehensive article Ophthalmol 1997; 8(3): 55–58. by Carmichael on cytomegalovirus (CMV) and eye.1 6 Patil AJ, Sharma A, Kenney MC, Kuppermann BD. In addition to the clinical features reported by the Valganciclovir in the treatment of cytomegalovirus retinitis author,1 we would like to highlight some additional in HIV-infected patients. Clin Ophthalmol 2012; 4: 111–119. salient clinical points associated with CMV and eye. With regard to clinical manifestation of CMV anterior R Agrawal uveitis, the iris atrophy is patchy or diffuse, with no posterior synechiae and no posterior segment changes.2 Department of Ophthalmology, Tan Tock Seng It is usually associated with increased intraocular Hospital, Singapore pressure.2 Chee and Jap3 also reported the presence of an E-mail: [email protected] immune ring in the cornea of patients with CMV anterior uveitis. Nodular endothelial lesions are white, medium- Eye (2012) 26, 1152; doi:10.1038/eye.2012.103; sized, nodular lesions surrounded by a translucent halo, published online 25 May 2012 which are significantly associated with CMV infection in cases of chronic anterior uveitis.2,3 Anterior uveitis with ocular hypertension resistant to topical steroid therapy and not clinically suggestive of the herpes group of Sir, virus makes the clinician suspect CMV infection.2 CMV Postoperative eye protection after cataract surgery anterior uveitis responds to ganciclovir, but the relapse rate is high and prolonged therapy may be required. -

Teaching Neuroimages: Central Serous Chorioretinopathy After Corticosteroid Treatment for Optic Neuritis
RESIDENT & FELLOW SECTION Teaching NeuroImages: Central Serous Chorioretinopathy After Corticosteroid Treatment for Optic Neuritis Jennifer Ling, MSc, and Jonathan A. Micieli, MD, CM Correspondence Dr. Micieli Neurology 2021;96:e305-e306. doi:10.1212/WNL.0000000000010807 ® jmicieli@ kensingtonhealth.org Figure Superior Central Serous Chorioretinopathy (CSCR) in the Right Eye and Central CSCR in the Left Eye After Corticosteroid Treatment for Optic Neuritis (A) Color fundus photographs demonstrating a localized superior serous detachment of the retina in the right eye (white arrow) and subfoveal serous detachment of the retina in the left eye (white arrow). (B) Optical coherence tomography of the macula over the localized areas of serous retina detachments demonstrating the subretinal fluid in both eyes (dashed white arrow). A 37-year-old woman presented with a 1-week history of painful vision loss in both eyes from optic MORE ONLINE neuritis. She was treated with intravenous, followed by oral corticosteroids. After she completed Teaching slides intravenous corticosteroids, she developed a new area of blurred vision inferiorly (right eye) and links.lww.com/WNL/ centrally (left eye) secondary to central serous chorioretinopathy (CSCR), which resolved after B213 oral prednisone taper (figure). CSCR is characterized by well-circumscribed serous detachments of the retina and is typically seen after exogenous corticosteroid use. CSCR can be misdiagnosed as optic neuritis1 or develop in patients with optic neuritis after corticosteroid treatment2 and should be kept in the differential diagnosis for worsening vision after corticosteroids. From the Faculty of Medicine (J.L.), University of British Columbia, Vancouver, British Columbia, Canada; Department of Ophthalmology and Vision Sciences (J.A.M.), University of Toronto, Toronto, Ontario, Canada; Division of Neurology (J.A.M.), Department of Medicine, University of Toronto, Toronto, Ontario, Canada; and Kensington Vision and Research Centre (J.A.M.), Toronto, Ontario, Canada. -
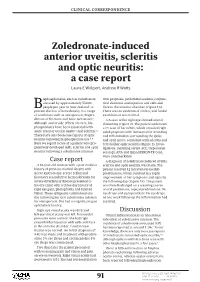
Zoledronate-Induced Anterior Uveitis, Scleritis and Optic Neuritis: a Case Report Laura E Wolpert, Andrew R Watts
clinical correspondence Zoledronate-induced anterior uveitis, scleritis and optic neuritis: a case report Laura E Wolpert, Andrew R Watts isphosphonates, such as zoledronate, with proptosis, periorbital oedema, conjunc- are used by approximately 55,000 tival chemosis and injection and cells and Bpeople per year in New Zealand1 to flare in the anterior chamber (Figure 1A). prevent the loss of bone density in a range There was no evidence of vitritis, and fundal of conditions such as osteoporosis, Paget’s examination was normal. 2 disease of the bone and bone metastases. A B-scan of the right eye showed scleral Although ocular side effects are rare, bis- thickening (Figure 2). The patient underwent phosphonates have been associated with a CT scan of her orbits, which revealed right- 3,4 4,5 acute anterior uveitis (AAU) and scleritis. sided proptosis with intraconal fat stranding There have also been case reports of optic and inflammation surrounding the globe 6–8 neuritis following bisphosphonate use. and optic nerve, consistent with scleritis and Here we report a case of a patient who pro- retrobulbar optic neuritis (Figure 3). Inves- gressively developed AAU, scleritis and optic tigations, including serum ACE, treponemal neuritis following a zoledronate infusion. serology, ANA and QuantiFERON-TB Gold, were unremarkable. Case report A diagnosis of zoledronate-induced uveitis, A 61-year-old woman with a past medical scleritis and optic neuritis was made. The history of previous morbid obesity with patient received 1g intravenous methyl- sleeve gastrectomy, severe reflux and prednisolone, which resulted in a rapid ileostomy secondary to hemicolectomy for improvement of her symptoms and signs by severe diverticular disease presented to the following day (Figure 1B).