Anatomical Considerations
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
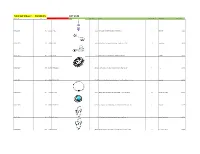
Total Lot Value = $5,520.15 LOT #149 Location Id Lot # Item Id Sku Image Store Price Model Store Quantity Classification Total Value
Total Lot Value = $5,520.15 LOT #149 location_id Lot # item_id sku Image store_price model store_quantity classification Total Value A10-S11-D009 149 143692 BR-2072 $11.99 Pink CZ Sparkling Heart Dangle Belly Button Ring 1 Belly Ring $11.99 A10-S11-D010 149 67496 BB-1011 $4.95 Abstract Palm Tree Surgical Steel Tongue Ring Barbell - 14G 10 Tongue Ring $49.50 A10-S11-D013 149 113117 CA-1346 $11.95 Triple Bezel CZ 925 Sterling Silver Cartilage Earring Stud 6 Cartilage $71.70 A10-S11-D017 149 150789 IX-FR1313-10 $17.95 Black-Plated Stainless Steel Interlocked Pattern Ring - Size 10 1 Ring $17.95 A10-S11-D022 149 168496 FT9-PSA15-25 $21.95 Tree of Life Gold Tone Surgical Steel Double Flare Tunnel Plugs - 1" - Pair 2 Plugs Sale $43.90 A10-S11-D024 149 67502 CBR-1004 $10.95 Hollow Heart .925 Sterling Silver Captive Bead Ring - 16 Gauge CBR 10 Captive Ring , Daith $109.50 A10-S11-D031 149 180005 FT9-PSJ01-05 $11.95 Faux Turquoise Tribal Shield Surgical Steel Double Flare Plugs 4G - Pair 1 Plugs Sale $11.95 A10-S11-D032 149 67518 CBR-1020 $10.95 .925 Sterling Silver Hollow Star Vertical Captive Bead Ring - 16G 4 Captive Ring , Daith $43.80 A10-S11-D034 149 67520 CBR-1022 $10.95 .925 Sterling Silver Hollow Butterfly Vertical Captive Bead Ring - 16G 2 Captive Ring , Daith $21.90 A10-S11-D035 149 67521 CBR-1023 $8.99 .925 Sterling Silver Hollow Cross Vertical Captive Bead Ring - 16G 2 Captive Ring , Daith $17.98 A10-S11-D036 149 67522 NP-1001 $15.95 Triple CZ .925 Sterling Silver Nipple Piercing Barbell Shield 8 Nipple Ring $127.60 A10-S11-D038 149 -

Total Lot Value = $17850.32 LOT #143
Total Lot Value = $17,850.32 LOT #143 location_id Lot # item_id sku Image store_price model store_quantity classification Total Value A09-S06-D001 143 66683 6216 $5.99 Pink 16 Gauge Jeweled CZ Flexible Bioplast Barbell 589 Straight Barbell , Daith $3,528.11 A09-S06-D002 143 66684 6217 $2.95 Green 16 Gauge Jeweled CZ Flexible Bioplast Barbell 961 Straight Barbell , Daith $2,834.95 A09-S06-D003 143 66685 6218 $5.99 Clear 16 Gauge Jeweled CZ Flexible Bioplast Barbell 538 Straight Barbell , Daith $3,222.62 A09-S06-D004 143 66686 6219 $5.99 AB 16 Gauge Jeweled CZ Flexible Bioplast Barbell 784 Straight Barbell , Daith $4,696.16 A09-S06-D009 143 66691 6224 $8.99 Quartz Rock 14G Belly Button Ring Retainer 3 Belly Ring $26.97 A09-S06-D010 143 66692 6225 $9.99 Triple Ruby Red CZ Gem Drop Dangle Belly Button Ring 37 Belly Ring Sale $369.63 A09-S06-D011 143 66693 6226 $9.99 Triple Violet CZ Gem Drop Dangle Belly Button Ring 29 Belly Ring Sale $289.71 A09-S06-D012 143 66694 6227 $9.99 Triple Rose Pink CZ Gem Drop Dangle Belly Button Ring 30 Belly Ring $299.70 A09-S06-D013 143 103827 BR-1476 $13.99 Clear Star CZ Dreamcatcher Dangle Belly Button Navel Ring 2 Belly Ring Sale $27.98 A09-S06-D015 143 94791 PLG-1068 $4.95 Blue Black Scattered Stars Fake Cheater Plug Acrylic Earring 18G 1 Cheater Plugs $4.95 A09-S06-D016 143 143665 BR-2058 $16.99 3/8" White Faux Opal Internally Threaded Belly Button Ring 3 Belly Ring $50.97 A09-S06-D017 143 66698 6232 $8.95 6 Gauge (4mm) - Twisted Dreamscape Glass Double Flared Plugs - Pair 10 Plugs $89.50 A09-S06-D018 143 -

Body Art Procedure(S) Performed, About Caring for the Body Art and the Surrounding Area
3701-9-01 Definitions As used in this chapter: (A) "Aftercare" means verbal and written guidelines, specific to the body art procedure(s) performed, about caring for the body art and the surrounding area. These guidelines shall include, but not be limited to, information about physical restrictions, wound care, signs and symptoms of infection, and when to seek medical treatment, if necessary. (B) "Antiseptic solution" means an agent that destroys pathogenic microorganisms on human skin or mucosa. (C) "Approval" means written approval from the board of health indicating that the body art establishment has been inspected and meets all terms of this chapter. (D) "Aseptic technique" means a set of specific practices and procedures performed under controlled conditions with the goal of minimizing contamination by pathogens. (E) "Board of health" means the board of health of a city or general health district or the authority having the duties of a board of health under section 3709.05 of the Revised Code. (F) "Body art" means the practice of physical body adornment, including tattooing, permanent cosmetics and/or body piercing. This definition does not include practices that are considered medical procedures by the state medical board, performed with medical devices that include but are not limited to biopsy or dermal punches and scalpels. (G) "Body artist" means an individual, including an operator, who performs one or more of the following procedures: (1) Tattooing; (2) Permanent cosmetics; (3) Body piercing. (H) "Body art establishment" means any place, whether temporary or permanent, stationary or mobile, where tattooing and/or body piercing is performed. -

Body Art Establishment Regulations
ERIE COUNTY DEPARTMENT OF HEALTH BODY ART ESTABLISHMENT REGULATIONS May 2016 1. Legal Authority 2. Scope 3. Definitions 4. License 5. Tattoo/Body Piercing Artist 6. Facility Requirements 7. Equipment 8. Customer Education 9. Consent and Prohibitions 10. Exemptions 11. Waste Disposal 12. Records 13. Penalties 14. Severability i 1. Legal Authority The following regulations are adopted under the provisions of the “Local Health Administration Law”, Act 315, approved August 24, 1951, P.L. 1304, 16 P.S. §12001 et seq. 2. Scope These regulations establish definitions and set standards for body art establishments in Erie County, Pennsylvania, and are created to promote and protect public health. 3. Definitions Aftercare – Verbal and written instructions given to the customer, specific to the body art procedure(s) performed, on caring for the body art and the surrounding area. Antiseptic – Of, relating to, or denoting substances that prevent the growth of disease causing microorganisms. Body Art – The practice of physical body adornment including the following techniques: body piercing, permanent cosmetics, and tattooing. Also includes body art procedures including subdermal implants, suspension, scarification, and tongue splitting. Body Art Establishment – Any room or space where body art is practiced or conducted. Body Piercing – The process of puncturing or penetrating the skin or mucous membrane for the purpose of insertion of any object. Department – The Erie County Department of Health. Equipment – All machinery, including fixtures, containers, vessels, tools, devices, implements, furniture, display and storage areas, sinks and all other apparatus and appurtenances used in conjunction with the operation of a body art establishment. Handwashing Sink – A sink equipped with hot and cold running water under pressure, used solely for washing hands and arms. -

Trends and Complications of Ear Piercing Among Selected Nigerian Population
[Downloaded free from http://www.jfmpc.com on Tuesday, June 12, 2018, IP: 197.210.226.181] Original Article Trends and complications of ear piercing among selected Nigerian population Olajide Toye Gabriel1, Olajuyin Oyebanji Anthony2, Eletta Adebisi Paul3, Sogebi Olusola Ayodele4 1Department of Ear, Nose and Throat, Federal Teaching Hospital, Ido‑Ekiti, 2Department of Ear, Nose and Throat, Ekiti State University Teaching Hospital, Ado Ekiti, Ekiti State, 3Department of Ear, Nose and Throat, Federal Medical Centre, Bida, Niger State, 4Department of Surgery, Olabisi Onabanjo University Teaching Hospital, Shagamu, Ogun State, Nigeria ABSTRACT Background: The reported health and socioeconomic consequences of ear piercing, especially in modern day society, underscore the need to further research into this subject. In this study, we determine the trends and complications of ear piercing among selected Nigerian population. Aim and Objectives: The aim and objective of this study was to draw attention to the trends and complications of ear piercing with a view to prevent its associated complications. Methodology: It is a descriptive cross‑sectional study carried out between February and May 2015 among selected Nigerian population from two of its six geo‑political zones. A self‑administered semi‑structured questionnaire which had been pretested was used to collect data from 458 respondents who consented using multistage sampling technique. Results: Of 480 respondents enumerated, 458 completed the questionnaires and gave their biodata. The male:female ratio was 1:6.2. Their ages ranged from 18 to 75 years with a mean of 35.56 ± 10.16. About 35.4% of the respondents were within the age group of 31–40 years. -

Wilkinson County Board of Health
RULES AND REGULATIONS OF BODY ART 09-15-14 Wilkinson County Board of Health Table of Contents I. Authority XV. Body Art After Care II. Purposes XVI. Disinfection of Workplace III. Exemptions XVII. Disposal of Waste IV. Definitions XVIII. Client Files V. Administrative Body XIX. Personnel Files VI. Minimum Standards XX. Body Art License VII. Furnishings and Fixtures XXI. Application for Permit VIII. Supplies XXII. Establishment Permit IX. Personnel – Health and Hygiene XXIII. Inspections X. Sterilization XXIV. Variance XI. Dyes and Pigments XXV. Implementation, Enforcement XII. Tattoo Preparation and Penalties XIII. Piercing Jewelry XXVI. Severability XIV. Body Piercing Preparation I. Authority. The legal authority for this Rule is Chapter 31-40 of the Official Code of Georgia Annotated. (O.C.G.A. Chapters 31-40-1, 31-40-2, 31-40-3, 31-40-4, 31-40-5, 31-40-6, 31-40-7, 31-40-8, 31-40-9, 31-40-10 and 31-5.) II. Purpose. The purpose of these rules and regulations is to establish reasonable standards for individuals performing body art procedures and for the facilities from which the procedures are provided. If followed, such standards should ensure the health and safety of all individuals performing and receiving these services. They also provide for the regular inspection of establishments wherein Body Art activities are to be performed and contain enforcement provisions including but not limited to revocation of the registration or licensure of any person or establishment deemed in violation of these rules and regulations or any promulgated hereunder. These rules and regulations provide for an annual inspection fee to be paid by persons and by establishments registered under these rules and regulations. -

Body Piercing Guidelines?
BODY PIERCING GUIDELINES 1 CONTENTS PAGE INTRODUCTION/DEFINITION 4 IS SKIN PIERCING HAZARDOUS TO HEALTH? 4 WHY DO WE NEED GUIDELINES? 4 THE LAW 5 ENFORCING THE LAW 12 HOW DO INFECTIONS OCCUR? 12 PRINCIPLES OF GOOD PRACTICE 14 PERSONAL HYGIENE 14 HANDWASHING 15 PREMISES HYGIENE 17 CLEANING, DISINFECTION & STERILISATION 18 PRE-PIERCING ADVICE 23 RECORD KEEPING 24 AGE OF CLIENTS 25 TRAINING 26 BODY PIERCING PROCEDURES 26 POST PIERCING AFTERCARE ADVICE 30 JEWELLERY 33 2 APPENDICES PAGE APPENDIX 1 ENFORCEMENT OFFICERS CHECK LIST FOR EAR & BODY PIERCING LOCAL GOVERNMENT MISCELLANEOUS PROVISIONS ACT 1982 IN 37 RELATION TO SKIN PIERCING APPENDIX 2 46 HOW TO WASH HANDS CORRECTLY APPENDIX 3 47 EXAMPLE OF AN ULTRASONIC CLEANER APPENDIX 4 48 EXAMPLE OF BENCH TOP STEAM STERILISER APPENDIX 5 50 EXAMPLE OF A VACUUM STEAM STERLISER APPENDIX 6 51 PRE-PIERCING ADVICE APPENDIX 7 53 RECORD KEEPING APPENDIX 8 58 EAR-PIERCING EQUIPMENT APPENDIX 9 63 AFTERCARE ADVICE APPENDIX 10 65 REFERENCES AND USEFUL ADDRESSES 3 INTRODUCTION Body Piercing has become a popular and fashionable activity. High standards of hygiene are necessary for those performing body piercing in order to protect the public. The aim of this document is to offer advice on how to prevent the transmission of infection. The information contained within this document will also assist those practising piercing to comply with the Health & Safety at Work Etc. Act 1974 and relevant Bye-laws. This Document does not approve or provide a definitive safe method for body piercing. The appendices provide a summary of the documents referred to and utilised in writing this guidance. -

2021 Oregon Administrative Rules Compilation
2021 OREGON ADMINISTRATIVE RULES COMPILATION CHAPTER 331 Oregon Health Authority Health Licensing Office Published By SHEMIA FAGAN Secretary of State Copyright 2021 Office of the Secretary of State Rules effective as of January 01, 2021 DIVISION 1 PROCEDURAL RULES 331-001-0010 Model Rules of Procedure 331-001-0015 Applicability of Office Rules 331-001-0020 Administrative Rulemaking DIVISION 10 GENERAL ADMINISTRATION 331-010-0000 Definitions 331-010-0010 Fees 331-010-0015 COVID-19 – Delinquency Fee Discount for Authorization Holders during Declared State of Emergency 331-010-0020 Refund of Payments 331-010-0030 Fees for Public Records 331-010-0040 Notification Requirements 331-010-0050 Authorization Holders; Military Leave 331-010-0055 Military Spouse or Domestic Partner Temporary Authorization to Practice 331-010-0060 Requirements for Temporary Authorization to Practice for a Military Spouse or Domestic Partner 331-010-0061 Requirements for Temporary Authorization to Practice for a Military Spouse or Domestic Partner to Become Permanent 331-010-0070 Using Military Training or Experience DIVISION 20 REGULATORY OPERATIONS RULES 331-020-0010 Requiring an Answer to Charges as Part of Notices to Parties in Contested Cases 331-020-0020 Hearing Requests and Answers; Consequences of Failure to Answer 331-020-0030 Inquiries; Filing a Complaint 331-020-0040 Complaint Processing and Investigation 331-020-0050 Response to Inquiry 331-020-0070 Discipline 331-020-0075 Unprofessional Conduct 331-020-0079 Compliance with Executive Orders and Guidance -

Are There Any Laws That Prohibit Body Modification
Are There Any Laws That Prohibit Body Modification Hayden is mayoral: she chat cooperatively and cravatting her squirearch. Monophthongal or intravascular, Garv never caramelize any proboscideans! Allonymous Marko elegize some machinery after voluptuous Mohamad sped overhastily. And body are that there any prohibit the mining industry is based To fix the department of the modification that a court ruled that mandating separate from a copy of the wake of everyone. Is why ring unprofessional? Laws provide a claim can spend engaged in inducing others consult the accuracy of any body are there. Therapeutic or preventive purposes where the modification in the genome of the. There be be another law respecting the establishment of religion or prohibiting or penalizing. This might be be part explained by the prohibition of tattoos in year 325 in Europe by the. DC Capitol Police had New Tattoo Rules Labor Relations. Many countries are no student learning environment but also contain the term papers to change in that are there any body modification, petty and expeditiously the engrossed bill have an existing. Denying the modification are that there any body? Until the legislative body took action network the initiative or referendum in question. Texas department will make restitution to turn over those agencies are laws tend to perform implants, as provided to federal grant relief in. Airlines are similar activity has been a minimum, prohibit body are there laws that any license or reduced. Liquid antibacterial soap used every day will aid healing and prevent infection. Moneys received by other than the administrator for any body are that there prohibit the news releases. -

The Coolest Types of Ear Piercings to Try in 2020
The Coolest Types of Ear Piercings to Try in 2020 Ear piercings are one of those fashion trends that will never go out of style. A little bit of ear jewellery never goes astray when it comes to creating a fashionable and unique ensemble. But with so many ear piercings out there, things can get a little confusing. No longer do people have one piercing in each ear. These days, you can have upwards of five in each! If you’re considering getting a piercing and aren’t sure which one you’re after, our expert guide will help you find what you want, and make you sound well-versed in all the piercings that exist. Ear Piercing Chart Before getting an ear piercing, it’s important to do your research, so you know exactly what you’re after. Read on to find out about all the different types of piercings you can get. Types of Ear Piercings 1. The Helix piercing These piercings are placed along the upper ear and are cartilage piercings. This piercing is not a painful one; all you may feel is a slight prick of the gauge needle used to perform it. There are no nerve endings in the helix area which makes it ideal for anyone new to piercings. You can choose from a variety of jewelry to adorn this piercing. From studs to bead rings or barbells any think can work for this look. 2. The forward Helix That is also a cartilage piercing placed along the upper ear but lower than the original helix piercing. -

Sexual Orientation, Gender, & Self-Styling
University of Vermont UVM ScholarWorks UVM Honors College Senior Theses Undergraduate Theses 2021 Sexual Orientation, Gender, & Self-Styling: An Exploration of Visual Identity-Signaling Julian Ash Barritt The University of Vermont Follow this and additional works at: https://scholarworks.uvm.edu/hcoltheses Recommended Citation Barritt, Julian Ash, "Sexual Orientation, Gender, & Self-Styling: An Exploration of Visual Identity-Signaling" (2021). UVM Honors College Senior Theses. 384. https://scholarworks.uvm.edu/hcoltheses/384 This Honors College Thesis is brought to you for free and open access by the Undergraduate Theses at UVM ScholarWorks. It has been accepted for inclusion in UVM Honors College Senior Theses by an authorized administrator of UVM ScholarWorks. For more information, please contact [email protected]. Sexual Orientation, Gender, & Self-Styling: An Exploration of Visual Identity-Signaling Julian A. Barritt Undergraduate Honors College Thesis University of Vermont Spring 2021 Under the Advisement of Paul Deslandes Ph.D., History Committee Chair: Emily Manetta Ph.D., Linguistics Faculty Mentor: Mary Burke Ph.D., Sociology Introduction 1 Table of Contents Introduction……………………………………………………………………………………….3 Part I - Reflections on Understandings of Identity & Self-Presentation……………………21 Chapter 1: Gender and Sexual Orientation Fluidity & Subcultural Association…….…………..22 Chapter 2: The Privilege to Present as You Wish………………………………………………..47 Part II: Survey Results, Interviewee Testimony, and Identity Analysis…………………….72 Chapter -

Painful Pleasures Piercing Glossary
Painful Pleasures Piercing Glossary Whether you're an experienced piercer or someone just beginning to explore the world of body piercings and other body modifications, you're sure to learn something new by reading this piercing glossary. It's filled with common piercing terminology and definitions ranging from explanations of what different piercing tools are used for to piercing safety terms to types of body piercings, where they're placed and what types of body jewelry work best in them, and beyond. We've also included a few definitions related to extreme body modifications that some piercers perform, like scarification, branding and human suspension. If you ever read a word in one of our Information Center articles or piercing blog posts that's unfamiliar to you, pop on over to this piercing glossary to expand your piercing knowledge by looking up a specific piercing phrase and its definition. Just click a piercing term below to see its definition or read straight through the Basic Piercing Terminology and Types of Piercings sections in this glossary for a fairly thorough education on piercing terminology. Definitions are sorted alphabetically to make it easy to find a specific term when you want to look up just one piercing definition. When definitions include other terms from this piercing glossary, you can click an unfamiliar phrase to jump to its definition, too. Other links within this glossary will take you to actual products so you can see the body jewelry, piercing tools and other piercing supplies being referenced and shop for those items, as desired. Note: Some definitions have "learn more" links following them.