Pulmonary Embolism What Is a Pulmonary Embolism?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Deep Vein Thrombosis in Behcet's Disease
BRIEF PAPER Clinical and Experimental Rheumatology 2001; 19 (Suppl. 24): S48-S50. Deep vein thrombosis ABSTRACT stitute the most frequent vascular mani- Objective festation seen in 6.2 to 33 % cases of in Behcet’s disease We aimed to describe the epidemiologi - BD (1, 2). We carried out this study to cal and clinical aspects of deep vein d e t e rmine the fre q u e n cy, the cl i n i c a l M.H. Houman1 thrombosis (DVT) in Behçet’s disease characteristics and course of deep vein 1 (BD) and to determine the patients at thrombosis (DVT) in BD patients and I. Ben Ghorbel high risk for this complication. to define a subgroup of patients at high I. Khiari Ben Salah1 Methods risk for this complication. M. Lamloum1 Among 113 patients with BD according 2 to the international criteria for classifi - Patients and methods M. Ben Ahmed cation of BD, those with DVT were ret - The medical records of one hundred M. Miled1 rospectively studied.The diagnosis of and thirteen patients with BD were re- DVT was made in all cases using con - viewed in order to investigate the pa- 1Department of Internal Medicine. La ventional venous angiography, venous tient’s medical history, the clinical ma- Rabta Hospital, 2Department of Immuno- ultrasonography and/or thoracic or ab - nifestations and outcome of the disease logy, Institute Pasteur. Tunis, Tunisia. dominal computed tomograp hy. Pa - as well as the treatment prescribed.The Houman M Habib, MD; Ben Ghorbel tients were divided in two subgroups diagnosis of BD was made based on the Imed, MD; Khiari Ben Salah Imen; a c c o rding to the occurrence of DV T criteria established by the international Lamloum Mounir, MD; Ben Ahmed other than cereb ral thromboses. -

Diagnosing Pulmonary Embolism M Riedel
309 Postgrad Med J: first published as 10.1136/pgmj.2003.007955 on 10 June 2004. Downloaded from REVIEW Diagnosing pulmonary embolism M Riedel ............................................................................................................................... Postgrad Med J 2004;80:309–319. doi: 10.1136/pgmj.2003.007955 Objective testing for pulmonary embolism is necessary, embolism have a low long term risk of subse- quent VTE.2 5–7 because clinical assessment alone is unreliable and the consequences of misdiagnosis are serious. No single test RISK FACTORS AND RISK has ideal properties (100% sensitivity and specificity, no STRATIFICATION risk, low cost). Pulmonary angiography is regarded as the The factors predisposing to VTE broadly fit Virchow’s triad of venous stasis, injury to the final arbiter but is ill suited for diagnosing a disease vein wall, and enhanced coagulability of the present in only a third of patients in whom it is suspected. blood (box 1). The identification of risk factors Some tests are good for confirmation and some for aids clinical diagnosis of VTE and guides decisions about repeat testing in borderline exclusion of embolism; others are able to do both but are cases. Primary ‘‘thrombophilic’’ abnormalities often non-diagnostic. For optimal efficiency, choice of the need to interact with acquired risk factors before initial test should be guided by clinical assessment of the thrombosis occurs; they are usually discovered after the thromboembolic event. Therefore, the likelihood of embolism and by patient characteristics that risk of VTE is best assessed by recognising the may influence test accuracy. Standardised clinical presence of known ‘‘clinical’’ risk factors. estimates can be used to give a pre-test probability to However, investigations for thrombophilic dis- orders at follow up should be considered in those assess, after appropriate objective testing, the post-test without another apparent explanation. -

Venous Air Embolism, Result- Retrospective Study of Patients with Venous Or Arterial Ing in Prompt Hemodynamic Improvement
Ⅵ REVIEW ARTICLE David C. Warltier, M.D., Ph.D., Editor Anesthesiology 2007; 106:164–77 Copyright © 2006, the American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Diagnosis and Treatment of Vascular Air Embolism Marek A. Mirski, M.D., Ph.D.,* Abhijit Vijay Lele, M.D.,† Lunei Fitzsimmons, M.D.,† Thomas J. K. Toung, M.D.‡ exogenously delivered gas) from the operative field or This article has been selected for the Anesthesiology CME Program. After reading the article, go to http://www. other communication with the environment into the asahq.org/journal-cme to take the test and apply for Cate- venous or arterial vasculature, producing systemic ef- gory 1 credit. Complete instructions may be found in the fects. The true incidence of VAE may be never known, CME section at the back of this issue. much depending on the sensitivity of detection methods used during the procedure. In addition, many cases of Vascular air embolism is a potentially life-threatening event VAE are subclinical, resulting in no untoward outcome, that is now encountered routinely in the operating room and and thus go unreported. Historically, VAE is most often other patient care areas. The circumstances under which phy- associated with sitting position craniotomies (posterior sicians and nurses may encounter air embolism are no longer fossa). Although this surgical technique is a high-risk limited to neurosurgical procedures conducted in the “sitting procedure for air embolism, other recently described position” and occur in such diverse areas as the interventional radiology suite or laparoscopic surgical center. Advances in circumstances during both medical and surgical thera- monitoring devices coupled with an understanding of the peutics have further increased concern about this ad- pathophysiology of vascular air embolism will enable the phy- verse event. -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
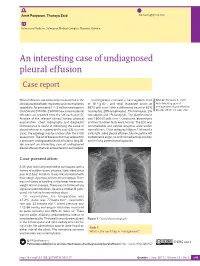
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Diagnosis of Chronic Thromboembolic Pulmonary Hypertension After Acute Pulmonary Embolism
Early View Review Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud, Marion Delcroix, Marc Humbert Please cite this article as: Klok FA, Couturaud F, Delcroix M, et al. Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.00189-2020). This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online. Copyright ©ERS 2020 Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud F2, Marion Delcroix M3, Marc Humbert4-6 1 Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, The Netherlands 2 Département de Médecine Interne et Pneumologie, Centre Hospitalo-Universitaire de Brest, Univ Brest, EA 3878, CIC INSERM1412, Brest, France 3 Department of Respiratory Diseases, University Hospitals and Respiratory Division, Department of Chronic Diseases, Metabolism & Aging, KU Leuven – University of Leuven, Leuven, Belgium 4 Université Paris-Saclay, Faculté de Médecine, Le Kremlin-Bicêtre, France 5 Service de Pneumologie et Soins Intensifs Respiratoires, Hôpital Bicêtre, AP-HP, Le Kremlin-Bicêtre, France 6 INSERM UMR S 999, Hôpital Marie Lannelongue, Le Plessis Robinson, France Corresponding author: Frederikus A. Klok, MD, FESC; Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, the Netherlands; Albinusdreef 2, 2300RC, Leiden, the Netherlands; Phone: +31- 715269111; E-mail: [email protected] Abstract Chronic thromboembolic pulmonary hypertension (CTEPH) is the most severe long-term complication of acute pulmonary embolism (PE). -

Peripheral Vascular Disease (PVD) Fact Sheet
FACT SHEET FOR PATIENTS AND FAMILIES Peripheral Vascular Disease (PVD) What is peripheral vascular disease? Vascular disease is disease of the blood vessels (arteries and veins). Peripheral vascular disease (PVD) affects The heart receives blood, the areas that are “peripheral,” or outside your heart. sends it to The most common types of PVD are: the lungs to get oxygen, • Carotid artery disease affects the arteries and pumps that carry blood to your brain. It occurs when it back out. one or more arteries are narrowed or blocked by plaque, a fatty substance that builds up inside artery walls. Carotid artery disease can increase Veins carry Arteries carry your risk of stroke. It can also cause transient blood to your oxygen-rich [TRANZ-ee-ent] ischemic [iss-KEE-mik] attacks (TIAs). heart to pick blood from up oxygen. your heart TIAs are temporary changes in brain function to the rest of that are sometimes called “mini-strokes.” your body. • Peripheral arterial disease (PAD) often affects the arteries to your legs and feet. It is also caused by Healthy blood vessels provide oxygen plaque buildup, and can for every part of your body. cause pain that feels like a dull cramp or heavy tiredness in your hips or legs when • Venous insufficiency affects the veins, usually you exercise or climb stairs. in your legs or feet. Your veins have valves that This pain is sometimes Damaged Healthy keepvalve blood fromvalve flowing backward as it moves called claudication. If PAD toward your heart. If the valves stop working, blood worsens, it can cause cold Plaque can build backs up in your body, usually in your legs. -

Vein Disease: Your Personal Prevention Programme While Your
Vein disease: Your personal prevention programme While your arteries transport blood containing oxygen and nutrients to the body cells, the veins are responsible for taking ‘used’ blood via the heart back to the lungs, where it can be enriched with fresh oxygen. In order for blood to be returned to the heart against the force of gravity, the vein valves must close tightly and the tissue which surrounds the veins must be strong. Otherwise the veins expand and become varicose. There’s a danger of thromboses, emboli and so-called ‘open leg’ ulcers. Self-diagnosis Spider-bursts (left) and reticular veins (right) are changes in the blood vessels which can be early signs of vein disease. Varicose veins (left and right) should be treated, if necessary surgically, as soon as possible. Deep vein thrombosis (left) is highly dangerous: You must seek treatment immediately! If you have vasculitis (inflammation of the vein wall - right) you should also visit a doctor or specialist clinic without delay. The classic symptoms of vein disease are swollen legs, pins and needles and feelings of tension in the calves, foot and calf cramps, legs which feel heavy or tired in the evening. Standing the whole day or frequent flying put a special burden on the vein system of the legs. © heigel.com www.heigel.com These things are good for your veins: Take frequent long walks as this exercises the leg and foot musculature. Sports involving sustained activity, such as hiking, swimming, jogging, skiing, dancing, cycling and gymnastics, are especially recommended. Whenever you are involved in an activity which involves sitting or standing, take every opportunity which presents itself to walk around. -

What Is Dvt? Deep Vein Thrombosis (DVT) Occurs When an Abnormal Blood Clot Forms in a Large Vein
What is DVt? Deep vein thrombosis (DVT) occurs when an abnormal blood clot forms in a large vein. These clots usually develop in the lower leg, thigh, or pelvis, but can also occur in other large veins in the body. If you develop DVT and it is diagnosed correctly and quickly, it can be treated. However, many people do not know if they are at risk, don’t know the symptoms, and delay seeing a healthcare professional if they do have symptoms. CAn DVt hAppen to me? Anyone may be at risk for DVT but the more risk factors you have, the greater your chances are of developing DVT. Knowing your risk factors can help you prevent DVt: n Hospitalization for a medical illness n Recent major surgery or injury n Personal history of a clotting disorder or previous DVT n Increasing age this is serious n Cancer and cancer treatments n Pregnancy and the first 6 weeks after delivery n Hormone replacement therapy or birth control products n Family history of DVT n Extended bed rest n Obesity n Smoking n Prolonged sitting when traveling (longer than 6 to 8 hours) DVt symptoms AnD signs: the following are the most common and usually occur in the affected limb: n Recent swelling of the limb n Unexplained pain or tenderness n Skin that may be warm to the touch n Redness of the skin Since the symptoms of DVT can be similar to other conditions, like a pulled muscle, this often leads to a delay in diagnosis. Some people with DVT may have no symptoms at all. -

A Comprehensive Study on Incidence and Risk Factors of Deep Vein Thrombosis in Asymptomatic Patient After Prolonged Surgery
D. Princess Beulah, T. Avvai. A comprehensive study on incidence and risk factors of deep vein thrombosis in asymptomatic patient after prolonged surgery. IAIM, 2019; 6(3): 237-242. Original Research Article A comprehensive study on incidence and risk factors of deep vein thrombosis in asymptomatic patient after prolonged surgery D. Princess Beulah1, T. Avvai2* 1Assistant Professor, Department of General Surgery, Govt. Stanley Medical College, Tamil Nadu, India 2Associate Professor, Department of General Surgery, Govt. Omandurar Medical College and Hospital, Tamil Nadu, India *Corresponding author email: [email protected] International Archives of Integrated Medicine, Vol. 6, Issue 3, March, 2019. Copy right © 2019, IAIM, All Rights Reserved. Available online at http://iaimjournal.com/ ISSN: 2394-0026 (P) ISSN: 2394-0034 (O) Received on: 28-02-2019 Accepted on: 04-03-2019 Source of support: Nil Conflict of interest: None declared. How to cite this article: D. Princess Beulah, T. Avvai. A comprehensive study on incidence and risk factors of deep vein thrombosis in asymptomatic patient after prolonged surgery. IAIM, 2019; 6(3): 237-242. Abstract Background: Deep vein thrombosis (DVT) is one of the most dreaded complications in postoperative patients as it is associated with considerable morbidity and mortality. The prevalence of Deep Vein Thrombosis (DVT) in various series involving Western population ranges from 15% to 40% among patients undergoing major general surgical procedures. The aim of the study: To identify risk factors of deep vein thrombosis in asymptotic patients after prolonged surgery Age, Gender, Diabetes, Hypertension, COPD, Hyperlipidemia, Renal disorder, liver disorder, duration of surgery, blood transfusion, nature of surgery elective or emergency, type of surgery. -

Pulmonary Embolism a Pulmonary Embolism Occurs When a Blood Clot Moves Through the Bloodstream and Becomes Lodged in a Blood Vessel in the Lungs
Pulmonary Embolism A pulmonary embolism occurs when a blood clot moves through the bloodstream and becomes lodged in a blood vessel in the lungs. This can make it hard for blood to pass through the lungs to get oxygen. Diagnosing a pulmonary embolism can be difficult because half of patients with a clot in the lungs have no symptoms. Others may experience shortness of breath, chest pain, dizziness, and possibly swelling in the legs. If you have a pulmonary embolism, you need medical treatment right away to prevent a blood clot from blocking blood flow to the lungs and heart. Your doctor can confirm the presence of a pulmonary embolism with CT angiography, or a ventilation perfusion (V/Q) lung scan. Treatment typically includes medications to thin the blood or placement of a filter to prevent the movement of additional blood clots to the lungs. Rarely, drugs are used to dissolve the clot or a catheter-based procedure is done to remove or treat the clot directly. What is a pulmonary embolism? Blood can change from a free flowing fluid to a semi-solid gel (called a blood clot or thrombus) in a process known as coagulation. Coagulation is a normal process and necessary to stop bleeding and retain blood within the body's vessels if they are cut or injured. However, in some situations blood can abnormally clot (called a thrombosis) within the vessels of the body. In a condition called deep vein thrombosis, clots form in the deep veins of the body, usually in the legs. A blood clot that breaks free and travels through a blood vessel is called an embolism. -

Pulmonary Embolism in the First Trimester of Pregnancy
Obstetrics & Gynecology International Journal Case Report Open Access Pulmonary embolism in the first trimester of pregnancy Summary Volume 11 Issue 1 - 2020 Pulmonary embolism in the first trimester of pregnancy without a known medical history Orfanoudaki Irene M is a very rare complication, which if it is misdiagnosed and left untreated leads to sudden Obstetric Gynecology, University of Crete, Greece pregnancy-related death. The sings and symptoms in this trimester are no specific. The causes for pulmonary embolism are multifactorial but in the first trimester of pregnancy, Correspondence: Orfanoudaki Irene M, Obstetric the most important causes are hereditary factors. Many times the pregnant woman ignores Gynecology, University of Crete, Greece, 22 Archiepiskopou her familiar hereditary history and her hemostatic system is progressively activated for the Makariou Str, 71202, Heraklion, Crete, Greece, Tel +30 hemostatic challenge of pregnancy and delivery. The hemostatic changes produce enhance 6945268822, +302810268822, Email coagulation and formation of micro-thrombi or thrombi and prompt diagnosis is crucial to prevent and treat pulmonary embolism saving the lives of a pregnant woman and her fetus. Received: January 19, 2020 | Published: January 28, 2020 Keywords: pregnancy, pulmonary embolism, mortality, diagnosis, risk factors, arterial blood gases, electrocardiogram, ventilation perfusion scan, computed tomography pulmonary angiogram, magnetic resonanance, compression ultrasonography, echocardiogram, D-dimers, troponin, brain