Host-Microbial Cross-Talk in Inflammatory Bowel Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -
Evaluation of 16S Rrna Primer Sets for Characterisation of Microbiota in Paediatric Patients with Autism Spectrum Disorder L
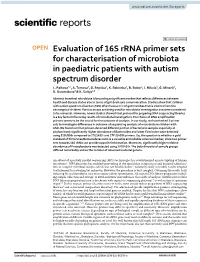
www.nature.com/scientificreports OPEN Evaluation of 16S rRNA primer sets for characterisation of microbiota in paediatric patients with autism spectrum disorder L. Palkova1,2, A. Tomova3, G. Repiska3, K. Babinska3, B. Bokor4, I. Mikula5, G. Minarik2, D. Ostatnikova3 & K. Soltys4,6* Abstract intestinal microbiota is becoming a signifcant marker that refects diferences between health and disease status also in terms of gut-brain axis communication. Studies show that children with autism spectrum disorder (ASD) often have a mix of gut microbes that is distinct from the neurotypical children. Various assays are being used for microbiota investigation and were considered to be universal. However, newer studies showed that protocol for preparing DNA sequencing libraries is a key factor infuencing results of microbiota investigation. The choice of DNA amplifcation primers seems to be the crucial for the outcome of analysis. In our study, we have tested 3 primer sets to investigate diferences in outcome of sequencing analysis of microbiota in children with ASD. We found out that primers detected diferent portion of bacteria in samples especially at phylum level; signifcantly higher abundance of Bacteroides and lower Firmicutes were detected using 515f/806r compared to 27f/1492r and 27f*/1495f primers. So, the question is whether a gold standard of Firmicutes/Bacteroidetes ratio is a valuable and reliable universal marker, since two primer sets towards 16S rRNA can provide opposite information. Moreover, signifcantly higher relative abundance of Proteobacteria was detected using 27f/1492r. The beta diversity of sample groups difered remarkably and so the number of observed bacterial genera. An advent of massively parallel sequencing (MPS) technologies has revolutionized an investigating of human microbiota1. -
C O N F E R E N C E 22 27 April 2016
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2015-2016 C o n f e r e n c e 22 27 April 2016 Cory Brayton, DVM, Ph.D., DACVP Associate Professor, Molecular & Comparative Pathobiology Johns Hopkins University School of Medicine Broadway Research Building, Suite 851 733 North Broadway Baltimore, MD 21205 CASE I: NIEHS-087 (JPC 4017222). Signalment: 11-month-old B6.129S- Cybbtm1Din/J mouse (Mus musculus) History: A breeding colony of B6.129S- Cybbtm1Din/J mice were housed in an AAALAC International accredited facility. The mice were housed in static micro isolator cases with ad libitum autoclaved food (NIH-31) and beta chip bedding. Mice were provided acidified water due to imm- unocompromised state. The mice were Body as a while, mouse. The liver was slightly enlarged, housed in the same room as B6 imm- and there are multiple tan foci in the liver and lung. (Photo courtesy of: National Institute of Environmental unocompetent mice. Sudden deaths were Health Sciences, Cellular and Molecular Pathology noted in the colony over a weekend. A total Branch and Comparative Medicine Branch, P.O. Box of 87 mice, aged from one to eleven months 12233, Research Triangle Park, NC 27709, http://www.niehs.nih.gov/research/atniehs/labs/lep/index. were affected. Of these, 45 mice were found cfm) dead and 19 sick mice were euthanized and were multifocal tan foci in the liver, spleen necropsied. Twenty males and 38 females and lung. were affected. Laboratory Results: From multiple tissues, Gross Pathology: The livers were pale and a pure culture of Burkholderia spp. -

Helicobacter Hepaticus Model of Infection: the Human Hepatocellular Carcinoma Controversy
Review articles Helicobacter hepaticus model of infection: the human hepatocellular carcinoma controversy Yessica Agudelo Zapata, MD,1 Rodrigo Castaño Llano, MD,2 Mauricio Corredor, PhD.3 1 Medical Doctor and General Surgeon in the Abstract Gastrohepatology Group at Universidad de Antioquia in Medellin, Colombia The discovery of Helicobacter 30 years ago by Marshall and Warren completely changed thought about peptic 2 Gastrointestinal Surgeon and Endoscopist in the and duodenal ulcers. The previous paradigm posited the impossibility of the survival of microorganisms in the Gastrohepatology Group at the Universidad de stomach’s low pH environment and that, if any microorganisms survived, they would stay in the duodenum Antioquia in Medellin, Colombia 3 Institute Professor of Biology in the Faculty of or elsewhere in the intestine. Today the role of H. pylori in carcinogenesis is indisputable, but little is known Natural Sciences and the GEBIOMIC Group the about other emerging species of the genus Helicobacter in humans. Helicobacter hepaticus is one of these Gastroenterology Group at the Universidad de species that has been studied most, after H. pylori. We now know about their microbiological, genetic and Antioquia in Medellin, Colombia pathogenic relationships with HCC in murine and human infections. This review aims to show the medical and ......................................... scientifi c community the existence of new species of Helicobacter that have pathogenic potential in humans, Received: 07-05-13 thus encouraging research. Accepted: 27-08-13 Keywords Helicobacter hepaticus, Helicobacter pylori, Helicobacter spp., hepatocellular carcinoma. INTRODUCTION bacterium can infect animals including mice, dogs and ger- bils which could lead to a proposal to use H. -

Potential for Enriching Next Generation Health Promoting Gut Bacteria Through Prebiotics and Other Dietary Components.Pdf
UCC Library and UCC researchers have made this item openly available. Please let us know how this has helped you. Thanks! Title Potential for enriching next-generation health-promoting gut bacteria through prebiotics and other dietary components Author(s) Lordan, Cathy; Thapa, Dinesh; Ross, R. Paul; Cotter, Paul D. Publication date 2019-05-22 Original citation Lordan, C., Thapa, D., Ross, R.P. and Cotter, P.D., 2019. Potential for enriching next-generation health-promoting gut bacteria through prebiotics and other dietary components. Gut microbes, (20pp). DOI:10.1080/19490976.2019.1613124 Type of publication Article (peer-reviewed) Link to publisher's https://www.tandfonline.com/doi/full/10.1080/19490976.2019.1613124 version http://dx.doi.org/10.1080/19490976.2019.1613124 Access to the full text of the published version may require a subscription. Rights © 2019 The Author(s). Published with license by Taylor & Francis Group, LLC. https://creativecommons.org/licenses/by/4.0/ Item downloaded http://hdl.handle.net/10468/9128 from Downloaded on 2021-10-04T07:34:18Z Gut Microbes ISSN: 1949-0976 (Print) 1949-0984 (Online) Journal homepage: https://www.tandfonline.com/loi/kgmi20 Potential for enriching next-generation health- promoting gut bacteria through prebiotics and other dietary components Cathy Lordan, Dinesh Thapa, R. Paul Ross & Paul D. Cotter To cite this article: Cathy Lordan, Dinesh Thapa, R. Paul Ross & Paul D. Cotter (2019): Potential for enriching next-generation health-promoting gut bacteria through prebiotics and other dietary components, Gut Microbes, DOI: 10.1080/19490976.2019.1613124 To link to this article: https://doi.org/10.1080/19490976.2019.1613124 © 2019 The Author(s). -

Dietary Supplementation with Inulin-Propionate Ester Or Inulin
Gut microbiota ORIGINAL ARTICLE Dietary supplementation with inulin-propionate ester Gut: first published as 10.1136/gutjnl-2019-318424 on 10 April 2019. Downloaded from or inulin improves insulin sensitivity in adults with overweight and obesity with distinct effects on the gut microbiota, plasma metabolome and systemic inflammatory responses: a randomised cross- over trial Edward S Chambers, 1 Claire S Byrne,1 Douglas J Morrison,2 Kevin G Murphy,3 Tom Preston,2 Catriona Tedford,4 Isabel Garcia-Perez,5 Sofia Fountana,5 Jose Ivan Serrano-Contreras,5 Elaine Holmes,5 Catherine J Reynolds,6 Jordie F Roberts,6 Rosemary J Boyton,6 Daniel M Altmann,6 Julie A K McDonald, 7 Julian R Marchesi,7,8 Arne N Akbar,9 Natalie E Riddell,10 Gareth A Wallis,11 Gary S Frost1 ► Additional material is ABSTRact published online only. To view Objective To investigate the underlying mechanisms Significance of this study please visit the journal online behind changes in glucose homeostasis with delivery (http:// dx. doi. org/ 10. 1136/ What is already known on this subject? gutjnl- 2019- 318424). of propionate to the human colon by comprehensive and coordinated analysis of gut bacterial composition, ► Short-chain fatty acids (SCFA), derived from For numbered affiliations see fermentation of dietary fibre by the gut end of article. plasma metabolome and immune responses. Design Twelve non-diabetic adults with overweight microbiota, have been shown to improve host insulin sensitivity. Correspondence to and obesity received 20 g/day of inulin-propionate ester (IPE), -

Oral and Fecal Campylobacter Concisus Strains Perturb Barrier Function by Apoptosis Induction in HT-29/B6 Intestinal Epithelial Cells
Oral and Fecal Campylobacter concisus Strains Perturb Barrier Function by Apoptosis Induction in HT-29/B6 Intestinal Epithelial Cells Hans Linde Nielsen1, Henrik Nielsen1, Tove Ejlertsen2, Jørgen Engberg3, Dorothee Gu¨ nzel4, Martin Zeitz5, Nina A. Hering5, Michael Fromm4,Jo¨ rg-Dieter Schulzke5*, Roland Bu¨ cker5 1 Department of Infectious Diseases, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark, 2 Department of Clinical Microbiology, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark, 3 Department of Clinical Microbiology, Slagelse Hospital, Slagelse, Denmark, 4 Institute of Clinical Physiology, Charite´ Universita¨tsmedizin Berlin, Berlin, Germany, 5 Department of Gastroenterology, Infectious Diseases and Rheumatology, Division of General Medicine and Nutrition, Charite´ Universita¨tsmedizin Berlin, Berlin, Germany Abstract Campylobacter concisus infections of the gastrointestinal tract can be accompanied by diarrhea and inflammation, whereas colonization of the human oral cavity might have a commensal nature. We focus on the pathophysiology of C. concisus and the effects of different clinical oral and fecal C. concisus strains on human HT-29/B6 colon cells. Six oral and eight fecal strains of C. concisus were isolated. Mucus-producing HT-29/B6 epithelial monolayers were infected with the C. concisus strains. Transepithelial electrical resistance (Rt) and tracer fluxes of different molecule size were measured in Ussing chambers. Tight junction (TJ) protein expression was determined by Western blotting, and subcellular TJ distribution was analyzed by confocal laser-scanning microscopy. Apoptosis induction was examined by TUNEL-staining and Western blot of caspase-3 activation. All strains invaded confluent HT-29/B6 cells and impaired epithelial barrier function, characterized by a time- and dose-dependent decrease in Rt either after infection from the apical side but even more from the basolateral compartment. -

Rapid Identification of Klebsiella Pneumoniae, Corynebacterium Kutscheri, and Streptococcus Pneumoniae Using Triplex Polymerase Chain Reaction in Rodents
Exp. Anim. 62(1), 35–40, 2013 —Original— Rapid Identification of Klebsiella pneumoniae, Corynebacterium kutscheri, and Streptococcus pneumoniae Using Triplex Polymerase Chain Reaction in Rodents Eui-Suk JEONG1), Kyoung-Sun Lee1,2), Seung-Ho HEO1,3), Jin-Hee SEO1), and Yang-Kyu CHOI1) 1)Department of Laboratory Animal Medicine, College of Veterinary Medicine, Konkuk University, 1 Hwayang-dong, Gwangjin-gu, Seoul 143-701, Republic of Korea 2)Osong Medical Innovation Foundation Laboratory Animal Center, 186 Osong Saengmyung-Ro, Gangoe-myeon, Cheongwon-gun, Chungbuk 363-951, Republic of Korea 3)Asan Institute for Life Sciences, University of Ulsan College of Medicine, 388–1 Pungnap-2-dong, Songpa-gu Seoul 138-736, Republic of Korea Abstract: Klebsiella pneumoniae, Corynebacterium kutscheri, and Streptococcus pneumoniae are important pathogens that cause respiratory infections in laboratory rodents. In this study, we used species-specific triplex PCR analysis to directly detect three common bacterial pathogens associated with respiratory diseases. Specific targets were amplified with conventional PCR using thetyrB gene from K. pneumoniae, gyrB gene from C. kutscheri, and ply gene from S. pneumoniae. Our primers were tested against purified DNA from another eleven murine bacteria to determine primer specificity. Under optimal PCR conditions, the triplex assay simultaneously yielded a 931 bp product from K. pneumoniae, a 540 bp product from C. kutscheri, and a 354 bp product from S. pneumoniae. The triplex assay detection thresholds for pure cultures were 10 pg for K. pneumoniae and S. pneumoniae, and 100 pg for C. kutscheri. All three bacteria were successfully identified in the trachea and lung of experimentally infected mice at the same time. -

Characterization of Antibiotic Resistance Genes in the Species of the Rumen Microbiota
ARTICLE https://doi.org/10.1038/s41467-019-13118-0 OPEN Characterization of antibiotic resistance genes in the species of the rumen microbiota Yasmin Neves Vieira Sabino1, Mateus Ferreira Santana1, Linda Boniface Oyama2, Fernanda Godoy Santos2, Ana Júlia Silva Moreira1, Sharon Ann Huws2* & Hilário Cuquetto Mantovani 1* Infections caused by multidrug resistant bacteria represent a therapeutic challenge both in clinical settings and in livestock production, but the prevalence of antibiotic resistance genes 1234567890():,; among the species of bacteria that colonize the gastrointestinal tract of ruminants is not well characterized. Here, we investigate the resistome of 435 ruminal microbial genomes in silico and confirm representative phenotypes in vitro. We find a high abundance of genes encoding tetracycline resistance and evidence that the tet(W) gene is under positive selective pres- sure. Our findings reveal that tet(W) is located in a novel integrative and conjugative element in several ruminal bacterial genomes. Analyses of rumen microbial metatranscriptomes confirm the expression of the most abundant antibiotic resistance genes. Our data provide insight into antibiotic resistange gene profiles of the main species of ruminal bacteria and reveal the potential role of mobile genetic elements in shaping the resistome of the rumen microbiome, with implications for human and animal health. 1 Departamento de Microbiologia, Universidade Federal de Viçosa, Viçosa, Minas Gerais, Brazil. 2 Institute for Global Food Security, School of Biological -

Endogenous Enterobacteriaceae Underlie Variation in Susceptibility to Salmonella Infection
ARTICLES https://doi.org/10.1038/s41564-019-0407-8 Endogenous Enterobacteriaceae underlie variation in susceptibility to Salmonella infection Eric M. Velazquez1, Henry Nguyen1, Keaton T. Heasley1, Cheng H. Saechao1, Lindsey M. Gil1, Andrew W. L. Rogers1, Brittany M. Miller1, Matthew R. Rolston1, Christopher A. Lopez1,2, Yael Litvak 1, Megan J. Liou1, Franziska Faber 1,3, Denise N. Bronner1, Connor R. Tiffany1, Mariana X. Byndloss1,2, Austin J. Byndloss1 and Andreas J. Bäumler 1* Lack of reproducibility is a prominent problem in biomedical research. An important source of variation in animal experiments is the microbiome, but little is known about specific changes in the microbiota composition that cause phenotypic differences. Here, we show that genetically similar laboratory mice obtained from four different commercial vendors exhibited marked phenotypic variation in their susceptibility to Salmonella infection. Faecal microbiota transplant into germ-free mice repli- cated donor susceptibility, revealing that variability was due to changes in the gut microbiota composition. Co-housing of mice only partially transferred protection against Salmonella infection, suggesting that minority species within the gut microbiota might confer this trait. Consistent with this idea, we identified endogenous Enterobacteriaceae, a low-abundance taxon, as a keystone species responsible for variation in the susceptibility to Salmonella infection. Protection conferred by endogenous Enterobacteriaceae could be modelled by inoculating mice with probiotic Escherichia coli, which conferred resistance by using its aerobic metabolism to compete with Salmonella for resources. We conclude that a mechanistic understanding of phenotypic variation can accelerate development of strategies for enhancing the reproducibility of animal experiments. recent survey suggests that the majority of researchers Results have tried and failed to reproduce their own experiments To determine whether genetically similar strains of mice obtained A or experiments from other scientists1. -

The Human Gut Microbiome in Early-Onset Type 1 Diabetes from the TEDDY Study Tommi Vatanen1*, Eric A
OPEN LETTER https://doi.org/10.1038/s41586-018-0620-2 The human gut microbiome in early-onset type 1 diabetes from the TEDDY study Tommi Vatanen1*, Eric A. Franzosa1,2, Randall Schwager2, Surya Tripathi1, Timothy D. Arthur1, Kendra Vehik3, Åke Lernmark4, William A. Hagopian5, Marian J. Rewers6, Jin-Xiong She7, Jorma Toppari8,9, Anette-G. Ziegler10,11,12, Beena Akolkar13, Jeffrey P. Krischer3, Christopher J. Stewart14,15, Nadim J. Ajami14, Joseph F. Petrosino14, Dirk Gevers1,19, Harri Lähdesmäki16, Hera Vlamakis1, Curtis Huttenhower1,2,20* & Ramnik J. Xavier1,17,18,20* Type 1 diabetes (T1D) is an autoimmune disease that targets species, and deficiency of bacteria that produce short-chain fatty pancreatic islet beta cells and incorporates genetic and acids (SCFAs)7,8 in cases of T1D or islet autoimmunity (IA)8,11,15,18. environmental factors1, including complex genetic elements2, Corroborating these findings, decreased levels of SCFA-producing patient exposures3 and the gut microbiome4. Viral infections5 bacteria were found in adults with type 2 diabetes (T2D)19. In addi- and broader gut dysbioses6 have been identified as potential tion, increased intestinal permeability14 and decreased microbial diver- causes or contributing factors; however, human studies have not sity12 after IA but before T1D diagnosis have been reported. Studies yet identified microbial compositional or functional triggers that using the nonobese diabetic (NOD) mouse model have determined are predictive of islet autoimmunity or T1D. Here we analyse immune mechanisms that mediate the protective effects of SCFAs9 10,913 metagenomes in stool samples from 783 mostly white, non- and the microbiome-linked sex bias in autoimmunity20. -

What Is the Healthy Gut Microbiota Composition? a Changing Ecosystem Across Age, Environment, Diet, and Diseases
microorganisms Review What is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases Emanuele Rinninella 1,2,* , Pauline Raoul 2, Marco Cintoni 3 , Francesco Franceschi 4,5, Giacinto Abele Donato Miggiano 1,2, Antonio Gasbarrini 2,6 and Maria Cristina Mele 1,2 1 UOC di Nutrizione Clinica, Dipartimento di Scienze Gastroenterologiche, Endocrino-Metaboliche e Nefro-Urologiche, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Rome, Italy; [email protected] (G.A.D.M.); [email protected] (M.C.M.) 2 Istituto di Patologia Speciale Medica, Università Cattolica del Sacro Cuore, 00168 Rome, Italy; [email protected] (P.R.); [email protected] (A.G.) 3 Scuola di Specializzazione in Scienza dell’Alimentazione, Università di Roma Tor Vergata, 00133 Rome, Italy; [email protected] 4 UOC di Medicina d’Urgenza e Pronto Soccorso, Dipartimento di Scienze dell’Emergenza, Anestesiologiche e della Rianimazione, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Rome, Italy; [email protected] 5 Istituto di Medicina Interna e Geriatria, Università Cattolica del Sacro Cuore, 00168 Rome, Italy 6 UOC di Medicina Interna e Gastroenterologia, Dipartimento di Scienze Gastroenterologiche, Endocrino-Metaboliche e Nefro-Urologiche, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Rome, Italy * Correspondence: [email protected] Received: 29 November 2018; Accepted: 9 January 2019; Published: 10 January 2019 Abstract: Each individual is provided with a unique gut microbiota profile that plays many specific functions in host nutrient metabolism, maintenance of structural integrity of the gut mucosal barrier, immunomodulation, and protection against pathogens. Gut microbiota are composed of different bacteria species taxonomically classified by genus, family, order, and phyla.