A Review of Indocyanine Green Fluorescent Imaging in Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Indocyanine Green Angiography
British Journal of Ophthalmology 1996; 80: 263-266 263 PERSPECTIVE Br J Ophthalmol: first published as 10.1136/bjo.80.3.263 on 1 March 1996. Downloaded from Indocyanine green angiography Sarah L Owens A brief survey of the recent ophthalmic literature under- initial investigations of ICG was published by Flower and scores a resurgence of interest in indocyanine green angio- Hochheimer, as well as by others.4-9 Some of their initial graphy (ICGA). This imaging method may be particularly work described a camera adapted with appropriate exciter useful for the ophthalmologist, as it provides at least a and barrier filters such that simultaneous ICG and fluores- theoretical advantage for improved imaging of the choroidal cein angiography could be performed after a single injec- circulation when compared with fluorescein angiography. tion of a combined mixture of ICG and fluorescein dyes.6 New temporal and spatial technological advances (that is, The ICG dosage used in these initial absorption angio- videoangiography and scanning laser ophthalmoscopy, res- graphy studies tended to be similar to the amount used for pectively) are primarily responsible for this renewed interest. cardiac flow studies - that is, 2 mg per kilogram body Thus, ICGA could become instrumental in elucidating the weight.' The early clinical investigators were uniformly pathogenetic mechanisms of a variety of diseases processes, disappointed in the lack of usefulness of ICGA in the con- as well as serving as a diagnostic and therapeutic tool. firmation of suspected choroidal neovascularisation.9-11 The flurry of recent publications on ICGA, particularly ICGA was not a useful guide to laser therapy of choroidal regarding age-related maculopathy (ARM), suggests a new neovascularisation, but appeared to show particular standard of care for the management of patients with this promise in evaluation and monitoring growth of choroidal disorder. -

Use of Laser-Assisted Indocyanine Green Angiography for Early Division of the Forehead Flap Pedicle
Research Original Investigation Use of Laser-Assisted Indocyanine Green Angiography for Early Division of the Forehead Flap Pedicle Joshua B. Surowitz, MD; Sam P. Most, MD IMPORTANCE The paramedian forehead flap is used to reconstruct medium to large nasal defects. The staged nature, with its vascular pedicle bridging the medial eyebrow to the nose, results in significant facial deformity. Earlier division lessens this morbidity. OBJECTIVES To quantify flap neovascularization 2 weeks after the initial flap transfer and to describe an algorithm for earlier division of the flap pedicle in select patient populations. DESIGN, SETTING, AND PARTICIPANTS We performed a prospective and retrospective study at the Ambulatory Surgery Center, Stanford University, Palo Alto, California, from October 14, 2014, through January 21, 2015. Patients with defects appropriate for paramedian forehead flap reconstruction had partial-thickness defects, vascularized tissue in more than 50% of the recipient bed, and no nicotine use. The patients underwent reconstructive surgery by a single surgeon from August 24, 2012, through September 12, 2014. Laser-assisted indocyanine green angiography was used for imaging before and immediately after the initial flap transfer, before pedicle division with the pedicle atraumatically clamped, and immediately after pedicle division and flap inset. Analysis of data and calculation of relative perfusion were performed using a postprocessing analysis toolkit. MAIN OUTCOMES AND MEASURES Perfusion was calculated using the analysis toolkit as the percentage of the area of interest relative to a predetermined reference point in normal peripheral tissue. RESULTS We enrolled a total of 10 patients. The mean (SD) relative perfusion of the forehead donor site before flap transfer was 61.2% (3.4%); at initial flap transfer, 81.4% (50.2% [range, 31%-214%]) (P = .70 compared with measurement before flap transfer). -

Simultaneous Indocyanine Green and Fluorescein Angiography Using a Confocal Scanning Laser Ophthalmoscope
CLINICAL SCIENCES Simultaneous Indocyanine Green and Fluorescein Angiography Using a Confocal Scanning Laser Ophthalmoscope William R. Freeman, MD; Dirk-Uwe Bartsch, PhD; Arthur J. Mueller, MD, PhD; Alay S. Banker, MD; Robert N. Weinreb, MD Background: Fluorescein and indocyanine green (ICG) performed in 45 minutes. It was possible to study dif- angiography are both useful in the diagnosis and treat- ferences in fluorescein patterns by comparing identi- ment of many retinal diseases. In some cases, both tests cally timed frames and to find cases in which ICG or fluo- must be performed for diagnosis and treatment; how- rescein was optimal in visualizing retinal and subretinal ever, performing both is time-consuming and may re- structures. Confocal optical sections in the depth (z) di- quire multiple injections. mension allowed viewing in different planes. It was pos- sible to overlay ICG and fluorescein images or compare Methods: We designed a compact digital confocal scan- them side-by-side using a linked cursor. Digital trans- ning laser ophthalmoscope to perform true simulta- mission of the images was also performed. neous fluorescein and ICG angiography. We report our experience using the instrument to perform 169 angio- Conclusions: Simultaneous ICG and fluorescein angi- grams in 117 patients. ography can be performed rapidly, safely, and conve- niently. The availability of simultaneous angiography will Results: There were no unexpected adverse effects from allow critical determination of the relative advantages and mixing the dyes and administering them in 1 injection. disadvantages of both types of angiography. An entire examination, including fundus photography, fluorescein angiography, and ICG angiography, could be Arch Ophthalmol. -
And Hypericum Perforatum
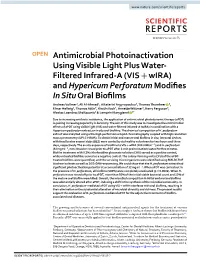
www.nature.com/scientificreports OPEN Antimicrobial Photoinactivation Using Visible Light Plus Water- Filtered Infrared-A (VIS + wIRA) and Hypericum Perforatum Modifes In Situ Oral Bioflms Andreas Vollmer1, Ali Al-Ahmad1, Aikaterini Argyropoulou2, Thomas Thurnheer 3, Elmar Hellwig1, Thomas Attin3, Kirstin Vach4, Annette Wittmer5, Kerry Ferguson6, Alexios Leandros Skaltsounis2 & Lamprini Karygianni 3* Due to increasing antibiotic resistance, the application of antimicrobial photodynamic therapy (aPDT) is gaining increasing popularity in dentistry. The aim of this study was to investigate the antimicrobial efects of aPDT using visible light (VIS) and water-fltered infrared-A (wIRA) in combination with a Hypericum perforatum extract on in situ oral bioflms. The chemical composition of H. perforatum extract was analyzed using ultra-high-performance liquid chromatography coupled with high resolution mass spectrometry (UPLC-HRMS). To obtain initial and mature oral bioflms in situ, intraoral devices with fxed bovine enamel slabs (BES) were carried by six healthy volunteers for two hours and three days, respectively. The ex situ exposure of bioflms to VIS + wIRA (200 mWcm−2) and H. perforatum (32 mg ml−1, non-rinsed or rinsed prior to aPDT after 2-min preincubation) lasted for fve minutes. Bioflm treatment with 0.2% chlorhexidine gluconate solution (CHX) served as a positive control, while untreated bioflms served as a negative control. The colony-forming units (CFU) of the aPDT- treated bioflms were quantifed, and the surviving microorganisms were identifed using MALDI-TOF biochemical tests as well as 16 S rDNA-sequencing. We could show that the H. perforatum extract had signifcant photoactivation potential at a concentration of 32 mg ml−1. -

Ophthalmic Fluorescein & Indocyanine Green Angiography
Ophthalmic Fluorescein & Indocyanine Green Angiography What Is Eye Angiography? Fluorescein and indocyanine green (ICG) angiography are diagnostic tests which use special cameras to photograph the structures in the back of the eye. These tests are very useful for finding leakage or damage to the blood vessels which nourish the retina (light sensitive tissue). In both tests, a colored dye is injected into a vein in the arm of the patient. The dye travels through the circulatory system and reaches the vessels in the retina and those of a deeper tissue layer called the choroid (see Fig. 1 below). Neither test involves the use of X–rays or harmful forms of radiation. Fluorescein is a yellow dye which glows in visible light. Indocyanine is a green dye which fluoresces with invisible infrared light; it requires a special digital camera sensitive to these light rays. Why Is Eye Angiography Performed? Both tests can help retina specialists diagnose and evaluate specific eye diseases. Fluorescein dye is best for studying the retinal circulation (see Fig. 2a below) while indocyanine green is often better for studying the deeper choroidal blood vessel layer (see Fig. 2b below). Certain eye disorders, such as diabetic retinopathy and retinal vascular occlusive disease affect primarily the retinal circulation and are usually imaged with fluorescein dye. In other disorders, such as age–related macular degeneration, where leakage is from the deeper choroidal vessels, both tests may be useful. Indocyanine green angiography is especially helpful when there is leakage of blood which may make interpretation of fluorescein studies difficult. When abnormal vessels or leakage is identified with an angiogram, laser treatment or pharmacological therapies may be indicated to prevent vision loss. -
Anaphylaxis During Intraoperative Indocyanine Green Angiography: a Complication to Watch Out
Case Report Anaphylaxis during intraoperative indocyanine green angiography: A complication to watch out Harnarayan Singh, Ankur Bajaj, Kiran Jangra1, Sviashanmugam Dhandapani Abstract Indocyanine green (ICG) angiography is widely used in cerebrovascular neurosurgery. We would like to report a case of intraoperative anaphylaxis to ICG during aneurysmal clipping and a view from the neurosurgeons’ perspective during such an event. Key words: Anaphylaxis, indocyanine green, neurosurgery INTRODUCTION ophthalmology and cardiology who have been using ICG for a fairly long time, neurosurgeons are just exploring Indocyanine green (ICG) angiography exists since 2003 the possibilities of its usefulness. There is no doubt of in the field of cerebrovascular surgery. The popularity of it being a surgeon and patient friendly modality. We ICG is gaining ground in the neurosurgical speciality due would like to report a case of anaphylaxis to ICG during to the competition offered by endovascular embolisation aneurysmal surgery. This is indeed a rare occurrence; in terms of not compromising the main vessels not however, it is always prudent to be extra cautious. jeopardising the safety of perforators along with satisfactory obliteration of an aneurysm. After achieving CASE REPORT satisfactory results with vascular microsurgery, new avenues are being considered to obtain safety of the A 55-year-old female presented with sudden severe vessels around, along with complete obliteration headache and vomiting. She was a known case of of aneurysm. Intraoperative digital substraction hypertension for 10 years, for which she was on angiography (Op-DSA) is increasingly being used in medication amlodipine, 5 mg OD. She was conscious, advanced care centres to ascertain the perfection in alert and with no focal deficits (Hunt and Hess Grade clipping technique. -
Optical Imaging Probes in Oncology
www.impactjournals.com/oncotarget/ Oncotarget, Vol. 7, No. 30 Review Optical imaging probes in oncology Cristina Martelli1,2, Alessia Lo Dico1,3, Cecilia Diceglie1,2,4, Giovanni Lucignani2,5 and Luisa Ottobrini1,2,6 1 Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy 2 Centre of Molecular and Cellular Imaging-IMAGO, Milan, Italy 3 Umberto Veronesi Foundation, Milan, Italy 4 Tecnomed Foundation, University of Milan-Bicocca, Monza, Italy 5 Department of Health Sciences, University of Milan, Milan, Italy 6 Institute for Molecular Bioimaging and Physiology (IBFM), National Research Council (CNR), Milan, Italy Correspondence to: Luisa Ottobrini, email: [email protected] Keywords: cancer, fluorescent probes, biomarkers, molecular processes, tumor cell features Received: October 02, 2015 Accepted: April 10, 2016 Published: April 27, 2016 ABSTRACT Cancer is a complex disease, characterized by alteration of different physiological molecular processes and cellular features. Keeping this in mind, the possibility of early identification and detection of specific tumor biomarkers by non-invasive approaches could improve early diagnosis and patient management. Different molecular imaging procedures provide powerful tools for detection and non-invasive characterization of oncological lesions. Clinical studies are mainly based on the use of computed tomography, nuclear-based imaging techniques and magnetic resonance imaging. Preclinical imaging in small animal models entails the use of dedicated instruments, and beyond the already cited imaging techniques, it includes also optical imaging studies. Optical imaging strategies are based on the use of luminescent or fluorescent reporter genes or injectable fluorescent or luminescent probes that provide the possibility to study tumor features even by means of fluorescence and luminescence imaging. -

WO 2016/130546 Al 18 August 2016 (18.08.2016) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2016/130546 Al 18 August 2016 (18.08.2016) P O P C T (51) International Patent Classification: (72) Inventors: HELLER, Daniel A.; 116 1 York Avenue, Apt. A61K 47/48 (2006.01) A61K 9/16 (2006.01) 3G, New York, NY 10065 (US). SHAMAY, Yosef; c/o A61K 31/00 (2006.01) Memorial Sloan Kettering Cancer Center, 1275 York Av enue, New York, NY 10065 (US). (21) International Application Number: PCT/US2016/017153 (74) Agents: HAULBROOK, William, R. et al; Choate, Hall & Stewart LLP, Two International Place, Boston, MA (22) International Filing Date: 021 10 (US). 9 February 2016 (09.02.2016) (81) Designated States (unless otherwise indicated, for every (25) Filing Language: English kind of national protection available): AE, AG, AL, AM, (26) Publication Language: English AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, (30) Priority Data: DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, 62/1 14,507 10 February 2015 (10.02.2015) US HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, (71) Applicant: MEMORIAL SLOAN KETTERING CAN¬ KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, MG, CER CENTER [US/US]; 1275 York Avenue, New York, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, NY 10065 (US). -
Clinical Study Protocol PP LNM 01
PINPOINT® for Lymph Node Mapping Clinical Study Protocol PP LNM 01 Clinical Study Protocol PROTOCOL NUMBER PP LNM 01 TITLE A Randomized, Prospective, Open Label, Multicenter Study Assessing the Safety and Utility of PINPOINT® Near Infrared Fluorescence Imaging in the Identification of Lymph Nodes in Subjects with Uterine and Cervical Malignancies who are Undergoing Lymph Node Mapping SHORT TITLE FILM PROTOCOL VERSION Version 6.0, August 25th, 2017 SPONSOR Novadaq Technologies Inc. 5090 Explorer Dr., Ste. 202, Mississauga, Ontario, Canada, L4W 4T9 Confidential This is a Novadaq Technologies Inc., document that contains confidential information. It is intended solely for the recipient clinical investigator(s) and must not be disclosed to any other party. Page 1 of 56 PINPOINT® for Lymph Node Mapping Clinical Study Protocol PP LNM 01 PROTOCOL APPROVAL Protocol Number: PP LNM 01 Title of Protocol: A Randomized, Prospective, Open Label, Multicenter Study Assessing the Safety and Utility of PINPOINT® Near Infrared Fluorescence Imaging in the Identification of Lymph Nodes in Subjects with Uterine and Cervical Malignancies who are Undergoing Lymph Node Mapping. Version: 6.0, August 25th, 2017 Approved by: 08/25/2017 Lori Swalm Date Sr. Vice President, Regulatory, Clinical and Economic Affairs Novadaq Technologies Inc. Approved by: Matt McKittrick On behalf of Date Yohan D’Souza, PhD Clinical Regulatory Scientist Novadaq Technologies Inc. Version 6.0, August 25th, 2017 Page 3 of 56 Novadaq - CONFIDENTIAL PINPOINT® for Lymph Node Mapping Clinical Study Protocol PP LNM 01 PROTOCOL APPROVAL Protocol Number: PP LNM 01 Title of Protocol: A Randomized, Prospective, Open Label, Multicenter Study Assessing the Safety and Utility of PINPOINT® Near Infrared Fluorescence Imaging in the Identification of Lymph Nodes in Subjects with Uterine and Cervical Malignancies who are Undergoing Lymph Node Mapping. -

Universidade De Brasília Faculdade De Ciências Da Saúde
UNIVERSIDADE DE BRASÍLIA FACULDADE DE CIÊNCIAS DA SAÚDE RODRIGO SOUZA SILVA VALLE DOS REIS AVALIAÇÃO IN SILICO DE FÁRMACOS COMERCIAIS PARA REPOSICIONAMENTO NA TERAPÊUTICA DA TUBERCULOSE BRASÍLIA 2020 Rodrigo Souza Silva Valle Dos Reis AVALIAÇÃO IN SILICO DE FÁRMACOS COMERCIAIS PARA REPOSICIONAMENTO NA TERAPÊUTICA DA TUBERCULOSE Dissertação de Mestrado apresentada ao Programa de Pós-Graduação em Ciências Farmacêuticas da Faculdade de Ciências da Saúde, Universidade de Brasília, como requisito parcial à obtenção do título de Mestre em Ciências Farmacêuticas. Orientador(a): Prof. Dr. Mauricio Homem de Mello BRASÍLIA 2020 Rodrigo Souza Silva Valle Dos Reis AVALIAÇÃO IN SILICO DE FÁRMACOS COMERCIAIS PARA REPOSICIONAMENTO NA TERAPÊUTICA DA TUBERCULOSE Dissertação de Mestrado apresentada ao Programa de Pós-Graduação em Ciências Farmacêuticas, Faculdade de Ciências da Saúde, Universidade de Brasília, como requisito parcial à obtenção do título de Mestre em Ciências Farmacêuticas. Aprovada em 27 de Agosto de 2020. Banca Examinadora ____________________________________ Prof. Dr. Maurício Homem de Mello – Universidade de Brasília ____________________________________ Profª. Dra. Pérola de Oliveira Magalhães – Universidade de Brasília ____________________________________ Profª. Dra. Márcia Renata Mortari – Universidade de Brasília AGRADECIMENTOS Ao professor Maurício, pela oportunidade de conhecer uma área completamente nova e diferente de tudo o que já havia tido contado na graduação, pela orientação fantástica, sempre disposto a ajudar e a sanar qualquer dúvida e principalmente por me acalmar e motivar, muito mais vezes do que imagina. À minha mãe, dona Lúcia, que sempre acredita em mim e me motiva em tudo o que decido fazer. Às todas as minhas colegas de InSiliTox, pelo companheirismo nos poucos momentos que pudemos interagir pessoalmente, mas principalmente à Adriana e a Giulia, com quem eu aprendi muito e sem as quais esse trabalho teria sido muito mais árduo e sem graça.