Immunization Status of the Under Fives in an Urban Area of Malappuram District
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Judicial First Class Magistrate Court-I, Perinthalmanna.Pdf
JUDICIAL FIRST CLASS MAGISTRATE COURT -I PERINTHALMANNA Disclosure Under Section 4(1)(B) Of The Right To Information Act 2005 1) COURT NAME : Judicial First Class Magistrate Court -I Perinthalmanna. ORGANIZATION, FUNCTIONS AND DUTIES. This is a Court for Criminal Offences, Judicial First Class Magistrate is the Presiding Officer and the Head of Office. One Junior Superintendent, who is the Chief Ministerial Officer and five clerical posts are the sanctioned strength of this court. This is the filing court of Two Police Stations in Malappuram District. 2) THE POWERS AND DUTIES OF EMPLOYEES The powers and duties of the Officer and Employees of this court are as prescribed in the relevant Acts and Rules relating to Subordinate Judiciary under Honourable High Court of Kerala. 3) THE PROCEDURE FOLLOWED IN THE DECISION MAKING PROCESS, INCLUDING CHANNELS OF SUPERVISION AND ACCOUNTABILITY : The decision making process in this court involves reception of tapals including FIRs, Occurrence Reports and final Reports filed by the Police and Excise Officials, and distributed to the sections concerned. Thereafter, the same will be verified by the section concerned and put up before the Magistrate for appropriate orders. The Charge sheets filed are verified by the Bench Clerk and will be taken on file and posted in the Bench for disposal. The channel of supervision in this court is represented in the following manner: Judicial First Class Magistrate ± Junior Superintendent ± Clerks 4) THE NORMS SET BY THIS COURT FOR THE DISCHARGE OF ITS FUNCTIONS The functions of this Court are discharged in accordance with the various rules and Regulations constituted for the purpose. -

EDUCATIONAL DISTRICT - MALAPPURAM Sl
LIST OF HIGH SCHOOLS IN MALAPPURAM DISTRICT EDUCATIONAL DISTRICT - MALAPPURAM Sl. Std. Std. HS/HSS/VHSS Boys/G Name of Name of School Address with Pincode Block Taluk No. (Fro (To) /HSS & irls/ Panchayat/Muncip m) VHSS/TTI Mixed ality/Corporation GOVERNMENT SCHOOLS 1 Arimbra GVHSS Arimbra - 673638 VIII XII HSS & VHSS Mixed Morayur Malappuram Eranad 2 Edavanna GVHSS Edavanna - 676541 V XII HSS & VHSS Mixed Edavanna Wandoor Nilambur 3 Irumbuzhi GHSS Irumbuzhi - 676513 VIII XII HSS Mixed Anakkayam Malappuram Eranad 4 Kadungapuram GHSS Kadungapuram - 679321 I XII HSS Mixed Puzhakkattiri Mankada Perinthalmanna 5 Karakunnu GHSS Karakunnu - 676123 VIII XII HSS Mixed Thrikkalangode Wandoor Eranad 6 Kondotty GVHSS Melangadi, Kondotty - 676 338. V XII HSS & VHSS Mixed Kondotty Kondotty Eranad 7 Kottakkal GRHSS Kottakkal - 676503 V XII HSS Mixed Kottakkal Malappuram Tirur 8 Kottappuram GHSS Andiyoorkunnu - 673637 V XII HSS Mixed Pulikkal Kondotty Eranad 9 Kuzhimanna GHSS Kuzhimanna - 673641 V XII HSS Mixed Kuzhimanna Areacode Eranad 10 Makkarapparamba GVHSS Makkaraparamba - 676507 VIII XII HSS & VHSS Mixed Makkaraparamba Mankada Perinthalmanna 11 Malappuram GBHSS Down Hill - 676519 V XII HSS Boys Malappuram ( M ) Malappuram Eranad 12 Malappuram GGHSS Down Hill - 676519 V XII HSS Girls Malappuram ( M ) Malappuram Eranad 13 Manjeri GBHSS Manjeri - 676121 V XII HSS Mixed Manjeri ( M ) Areacode Eranad 14 Manjeri GGHSS Manjeri - 676121 V XII HSS Girls Manjeri ( M ) Areacode Eranad 15 Mankada GVHSS Mankada - 679324 V XII HSS & VHSS Mixed Mankada Mankada -

List of Offices Under the Department of Registration
1 List of Offices under the Department of Registration District in Name& Location of Telephone Sl No which Office Address for Communication Designated Officer Office Number located 0471- O/o Inspector General of Registration, 1 IGR office Trivandrum Administrative officer 2472110/247211 Vanchiyoor, Tvpm 8/2474782 District Registrar Transport Bhavan,Fort P.O District Registrar 2 (GL)Office, Trivandrum 0471-2471868 Thiruvananthapuram-695023 General Thiruvananthapuram District Registrar Transport Bhavan,Fort P.O District Registrar 3 (Audit) Office, Trivandrum 0471-2471869 Thiruvananthapuram-695024 Audit Thiruvananthapuram Amaravila P.O , Thiruvananthapuram 4 Amaravila Trivandrum Sub Registrar 0471-2234399 Pin -695122 Near Post Office, Aryanad P.O., 5 Aryanadu Trivandrum Sub Registrar 0472-2851940 Thiruvananthapuram Kacherry Jn., Attingal P.O. , 6 Attingal Trivandrum Sub Registrar 0470-2623320 Thiruvananthapuram- 695101 Thenpamuttam,BalaramapuramP.O., 7 Balaramapuram Trivandrum Sub Registrar 0471-2403022 Thiruvananthapuram Near Killippalam Bridge, Karamana 8 Chalai Trivandrum Sub Registrar 0471-2345473 P.O. Thiruvananthapuram -695002 Chirayinkil P.O., Thiruvananthapuram - 9 Chirayinkeezhu Trivandrum Sub Registrar 0470-2645060 695304 Kadakkavoor, Thiruvananthapuram - 10 Kadakkavoor Trivandrum Sub Registrar 0470-2658570 695306 11 Kallara Trivandrum Kallara, Thiruvananthapuram -695608 Sub Registrar 0472-2860140 Kanjiramkulam P.O., 12 Kanjiramkulam Trivandrum Sub Registrar 0471-2264143 Thiruvananthapuram- 695524 Kanyakulangara,Vembayam P.O. 13 -
List of Lacs with Local Body Segments (PDF
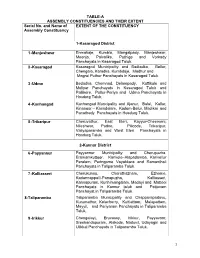
TABLE-A ASSEMBLY CONSTITUENCIES AND THEIR EXTENT Serial No. and Name of EXTENT OF THE CONSTITUENCY Assembly Constituency 1-Kasaragod District 1 -Manjeshwar Enmakaje, Kumbla, Mangalpady, Manjeshwar, Meenja, Paivalike, Puthige and Vorkady Panchayats in Kasaragod Taluk. 2 -Kasaragod Kasaragod Municipality and Badiadka, Bellur, Chengala, Karadka, Kumbdaje, Madhur and Mogral Puthur Panchayats in Kasaragod Taluk. 3 -Udma Bedadka, Chemnad, Delampady, Kuttikole and Muliyar Panchayats in Kasaragod Taluk and Pallikere, Pullur-Periya and Udma Panchayats in Hosdurg Taluk. 4 -Kanhangad Kanhangad Muncipality and Ajanur, Balal, Kallar, Kinanoor – Karindalam, Kodom-Belur, Madikai and Panathady Panchayats in Hosdurg Taluk. 5 -Trikaripur Cheruvathur, East Eleri, Kayyur-Cheemeni, Nileshwar, Padne, Pilicode, Trikaripur, Valiyaparamba and West Eleri Panchayats in Hosdurg Taluk. 2-Kannur District 6 -Payyannur Payyannur Municipality and Cherupuzha, Eramamkuttoor, Kankole–Alapadamba, Karivellur Peralam, Peringome Vayakkara and Ramanthali Panchayats in Taliparamba Taluk. 7 -Kalliasseri Cherukunnu, Cheruthazham, Ezhome, Kadannappalli-Panapuzha, Kalliasseri, Kannapuram, Kunhimangalam, Madayi and Mattool Panchayats in Kannur taluk and Pattuvam Panchayat in Taliparamba Taluk. 8-Taliparamba Taliparamba Municipality and Chapparapadavu, Kurumathur, Kolacherry, Kuttiattoor, Malapattam, Mayyil, and Pariyaram Panchayats in Taliparamba Taluk. 9 -Irikkur Chengalayi, Eruvassy, Irikkur, Payyavoor, Sreekandapuram, Alakode, Naduvil, Udayagiri and Ulikkal Panchayats in Taliparamba -

Ground Water Information Booklet of Alappuzha District
TECHNICAL REPORTS: SERIES ‘D’ CONSERVE WATER – SAVE LIFE भारत सरकार GOVERNMENT OF INDIA जल संसाधन मंत्रालय MINISTRY OF WATER RESOURCES कᴂ द्रीय भजू ल बो셍 ड CENTRAL GROUND WATER BOARD केरल क्षेत्र KERALA REGION भूजल सूचना पुस्तिका, मलꥍपुरम स्ज쥍ला, केरल रा煍य GROUND WATER INFORMATION BOOKLET OF MALAPPURAM DISTRICT, KERALA STATE तत셁वनंतपुरम Thiruvananthapuram December 2013 GOVERNMENT OF INDIA MINISTRY OF WATER RESOURCES CENTRAL GROUND WATER BOARD GROUND WATER INFORMATION BOOKLET OF MALAPPURAM DISTRICT, KERALA जी श्रीनाथ सहायक भूजल ववज्ञ G. Sreenath Asst Hydrogeologist KERALA REGION BHUJAL BHAVAN KEDARAM, KESAVADASAPURAM NH-IV, FARIDABAD THIRUVANANTHAPURAM – 695 004 HARYANA- 121 001 TEL: 0471-2442175 TEL: 0129-12419075 FAX: 0471-2442191 FAX: 0129-2142524 GROUND WATER INFORMATION BOOKLET OF MALAPPURAM DISTRICT, KERALA TABLE OF CONTENTS DISTRICT AT A GLANCE 1.0 INTRODUCTION ..................................................................................................... 1 2.0 CLIMATE AND RAINFALL ................................................................................... 3 3.0 GEOMORPHOLOGY AND SOIL TYPES .............................................................. 4 4.0 GROUNDWATER SCENARIO ............................................................................... 5 5.0 GROUNDWATER MANAGEMENT STRATEGY .............................................. 11 6.0 GROUNDWATER RELATED ISaSUES AND PROBLEMS ............................... 14 7.0 AWARENESS AND TRAINING ACTIVITY ....................................................... 14 -

Public Notice for Sale/Auction of Immovable Properties {Under SARFAESI Act Read with Proviso to Rule 8 (6) of the Security Interest (Enforcement) Rules}
Corporate Office:-, “Axis House”, C-2, Wadia International Centre, Pandurang Budhkar Marg, Worli, Mumbai – 400025 Registered Office: “Trishul”, 3rd Floor Opp. Samartheshwar Temple Law Garden, Ellisbridge Ahmedabad – 380006 Retail Assets Center ;Axis Bank Limited, 2ND FLOOR,GLOBAL TOWER,NEAR V ZONE MALL PARAYENCHERI CALICUT-673016. Public notice for Sale/Auction of immovable properties {under SARFAESI Act read with proviso to Rule 8 (6) of the Security Interest (Enforcement) Rules} Whereas the Authorized Officer of Axis Bank Ltd. (hereinafter referred to as ‘the Bank’), under Securitisation and Reconstruction of Financial Assets and Enforcement of Security Interest Act, 2002 (in short ‘SARFAESI Act) and in exercise of powers conferred under Section 13(12) read with the Security Interest (Enforcement) Rules, 2002 issued Demand Notice under Sec. 13(2) of SARFAESI Act calling upon the below-mentioned Borrowers/Co-borrowers/mortgagors/Guarantors to repay the amount mentioned in the notice being the amount due together with further interest thereon at the contractual rate plus all costs charges and incidental expenses etc. till the date of payment within 60 days from the date of the said notice. The Borrowers/Co-borrowers/mortgagors/Guarantors having failed to repay the above said amount within the specified period, the authorized officer has taken over physical possession in exercise of powers conferred under Section 13(4) of SARFAESI Act read with Security Interest (Enforcement) Rules, 2002, which is to be sold by way of auction on “As Is Where Is Basis”, “As Is What Is Basis”, “Whatever There Is Basis”,for realization of Bank’s dues under Rules 8 and 9 of Security Interest (Enforcement) Rules, 2002 by inviting tenders/bids as per below Auction schedule: AUCTION SCHEDULE All the piece and parcels of immovable property admeasuring 3.906 Ares with all improvements thereon situated in Survey No.87/2 Amminikkad Amsom in thazhekkode village of Perinthalmanna Taluk in Malappuram district Sale deed No. -
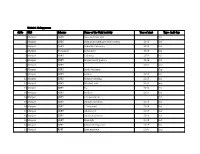
District: Malappuram Sl.No ULB Scheme Name of the Unit/ Activity
District: Malappuram Sl.No ULB Scheme Name of the Unit/ Activity Year of start Type- Ind/ Grp 1 Manjeri SJSRY Sanu tailoring unit Ind 2 Manjeri SJSRY Stringz kudumbasree (data entry) 2013 Ind 3 Manjeri SJSRY Rahmath stationary 2015 Ind 4 Manjeri Yuvashree Royal store 2015 Ind 5 Manjeri SJSRY Tailoring 2014 Ind 6 Manjeri SJSRY Shalus beauti parlour 2014 Ind 7 Manjeri SJSRY 2017 Grp 8 Manjeri SJSRY Sneha tailoring Grp 9 Manjeri SJSRY Golden 2014 Ind 10 Manjeri SJSRY Tishma tailoring 2015 Ind 11 Manjeri SJSRY Excelant unit 2013 Grp 12 Manjeri SJSRY K s 2014 Ind 13 Manjeri SJSRY Modern 2016 Ind 14 Manjeri SJSRY C h decoration Ind 15 Manjeri SJSRY Athulya furniture 2015 Ind 16 Manjeri SJSRY P l m sound 2014 Ind 17 Manjeri SJSRY Athira toys 2014 Ind 18 Manjeri SJSRY Anoos decoration 2016 Ind 19 Manjeri SJSRY Hair style 2015 Ind 20 Manjeri SJSRY Jalaja tailoring unit 2015 Ind 21 Manjeri RME Jams nutrimix 2006 Grp 22 Manjeri RME Dhanyadhra ayurvedic Ind 23 Manjeri NULM Day care 2018 Ind 24 Manjeri NULM Electrical sale 2018 Ind 25 Manjeri NULM Tailoring 2018 Ind 26 Manjeri NULM Pharmaceuticals 2018 Ind 27 Manjeri NULM Catering unit 2018 Ind 28 Manjeri NULM Santhwanam 2018 Ind 29 Manjeri NULM Day Care 2018 Grp 30 Tanur Own Fund Meenus flour & oil mill 2010 Ind 31 Tanur Own Fund Pavithra vanitha cantein 2015 Grp 32 Tanur Linkage Loan Sangeetha vanitha cantein 2000 Grp 33 Tanur Own Fund Panchami cloth bag 2017 Grp 34 Tanur RME Madurima palaharam 2010 Grp 35 Tanur Own Fund Chembakkam palaharam 2016 Grp 36 Tanur RME Ruchi palaharam 2011 Grp 37 Tanur -

LIST of PRIVATE LABS APPROVED by STATE for COVID TESTING AS on 21-08-2020 Cost of Tests Fixed by Government of Kerala in Private Sector
LIST OF PRIVATE LABS APPROVED BY STATE FOR COVID TESTING AS ON 21-08-2020 Cost of tests fixed by Government of Kerala in Private Sector. TYPE OF RESULT RATE( Inclusive of Tax) TEST RT-PCR CONFIRMATORY Rs 2750/- OPEN CBNAAT CONFIRMATORY Rs 3000/- TRUENAT If STEP1 is positive, require step 2 for confirmation STEP 1- Rs 1500/- STEP 1 negative is confirmatory STEP2- Rs1500/-( required only if STEP1 turns positive) ANTIGEN Positive results are confirmatory. Rs 625/- Negative results in a symptomatic person require + cost of further RT-PCR/CBNAAT/TRUENAT test RT- PCR/CBNAAT/TRUENAT if required Private Labs approved for RT-PCR open system 1. DDRC SRL Diagnostics Pvt Ltd, Panampilly Nagar, Ernakulam 2. MIMS Lab Services, Govindapuram, Kozhikode 3. Lab Services of Amrita Institute of Medical Sciences & Research Centre, AIMSPonekkara, Kochi 4. Dane Diagnostics Pvt Ltd, 18/757 (1), RC Road, Palakkad 5. Medivision Scan & Diagnostic Research Centre Pvt Ltd, Sreekandath Road, Kochi 6. MVR Cancer Centre & Research Institute, CP 13/516 B, C, Vellalaserri NIT (via), Poolacode, Kozhikode 7. Aza Diagnostic Centre, Stadium Puthiyara Road, Kozhikode 8. Neuberg Diagnostics Private Limited, Thombra Arcade, Ernakulam 9. Jeeva Specialty Laboratory, Thrissur 10. MES Medical College, Perinthalmanna, Malappuram Private Labs approved for XPERT/CBNAAT Testing 1. Amrita Institute of Medical Science, Kochi 2. Aster Medcity, Aster DM Healthcare Ltd, Kutty Sahib Road, Kothad, Cochin 3. NIMS Medicity, Aralumoodu, Neyyattinkara, Thiruvananthapuram 4. Rajagiri Hospital Laboratory Services, Rajagiri Hospital, Chunangamvely, Aluva 5. Micro Health LAbs, MPS Tower, Kozhikode 6. Believers Church Medical College Laboratory, St Thomas Nagar, Kuttapuzha P.O., Thiruvalla 7. -

1. Fresh Stage Carriage Permit
RTA Malappuram 25, January 2017 Public Agenda REGIONAL TRANSPORT AUTHORITY – MALAPPURAM 25 JANUARY 2017 AGENDA (PUBLIC) 1. FRESH STAGE CARRIAGE PERMIT Item No. 1 G2/181536/2015/M Agenda To re-consider the application for regular Stage Carriage permit to operate on the route Tirur – Theyyala – Pookiparamba (via) Vylathur Plate Company, Parapparappuram, Manalippuzha (Pocker Padi) and Arakkal (Thennala) as OS. Applicant Mr. Gafoor, S/o. Ahammed, Thottiparamabil House, Omachappuzha P.O., Perincheri, Tirur, Malappuram. Proposed Timings Tirur Theyyala Pookkiparamba A D Pass A D 6.20 6.50 7.10 8.05 7.35 7.15 8.20 8.50 9.10 10.10 9.40 9.20 10.20 10.50 11.10 12.15 11.45 11.25 12.30 1.00 01.20 02.35 2.05 01.45 02.50 3.20 3.40 4.45 4.15 3.55 05.00 5.30 05.50 6.50 6.20 06.00 7.05 7.35 7.55 8.55 Halt 8.25 8.05 1 RTA Malappuram 25, January 2017 Public Agenda Item No. 2 G2/145630/2015/M Agenda To re-consider the application for regular Stage Carriage permit to operate on the route Olavettur – Mukkam (via) Puthiyodathuparamba, Mundumuzhi, Edavannappara, Edasserikadavu, Keezhuparamba, Pazhamparamba, Pottammal, Cheruvadi, Kodiyathur and Karasserri Junction. Applicant Mr. Sameer K.P., S/o. Shoukathali, Kizhkalathil House, Cheruvadi P.O., Kozhikkode Proposed Timings (Settled on 10.01.2017) Olavattur Puthiydthprma Edavannappara Cheruvadi Mukkam A D A D A D A D A D 5.10 5.15 P 5.40 6.12 6.07 P 5.42 6.15 6.20 P 6.45 6.53 7.13 7.20 7.40 8.40 8.15 8.20 7.55 9.16 9.36 9.37 9.57 11.00 10.39 10.40 10.19 11.09 11.29 P 11.49 12.34 12.14 12.59 12.39 01.40 02.00 02.05 02.26 03.45 03.25 04.10 03.50 04.31 04.51 05.11 05.40 05.20 06.05 05.45 06.10 06.30 P 06.50 07.55 07.35 08.50 08.45 P 08.20 P 08.00 08.55 09.00 P 09.25 10.00 09.55 P 09.30 Halt 2 RTA Malappuram 25, January 2017 Public Agenda Item No. -

Ahtl-European STRUGGLE by the MAPPILAS of MALABAR 1498-1921 AD
AHTl-EUROPEAn STRUGGLE BY THE MAPPILAS OF MALABAR 1498-1921 AD THESIS SUBMITTED FDR THE AWARD OF THE DEGREE DF Sactnr of pitilnsopliQ IN HISTORY BY Supervisor Co-supervisor PROF. TARIQ AHMAD DR. KUNHALI V. Centre of Advanced Study Professor Department of History Department of History Aligarh Muslim University University of Calicut Al.garh (INDIA) Kerala (INDIA) T6479 VEVICATEV TO MY FAMILY CONTENTS SUPERVISORS' CERTIFICATE ACKNOWLEDGEMENT LIST OF MAPS LIST OF APPENDICES ABBREVIATIONS Page No. INTRODUCTION 1-9 CHAPTER I ADVENT OF ISLAM IN KERALA 10-37 CHAPTER II ARAB TRADE BEFORE THE COMING OF THE PORTUGUESE 38-59 CHAPTER III ARRIVAL OF THE PORTUGUESE AND ITS IMPACT ON THE SOCIETY 60-103 CHAPTER IV THE STRUGGLE OF THE MAPPILAS AGAINST THE BRITISH RULE IN 19™ CENTURY 104-177 CHAPTER V THE KHILAFAT MOVEMENT 178-222 CONCLUSION 223-228 GLOSSARY 229-231 MAPS 232-238 BIBLIOGRAPHY 239-265 APPENDICES 266-304 CENTRE OF ADVANCED STUDY DEPARTMENT OF HISTORY ALIGARH MUSLIM UNIVERSITY ALIGARH - 202 002, INDIA CERTIFICATE This is to certify that the thesis "And - European Struggle by the Mappilas of Malabar 1498-1921 A.D." submitted for the award of the degree of Doctor of Philosophy of the Aligarh Muslim University, is a record of bonafide research carried out by Salahudheen O.P. under our supervision. No part of the thesis has been submitted for award of any degree before. Supervisor Co-Supervisor Prof. Tariq Ahmad Dr. Kunhali.V. Centre of Advanced Study Prof. Department of History Department of History University of Calicut A.M.U. Aligarh Kerala ACKNOWLEDGEMENT My earnest gratitude is due to many scholars teachers and friends for assisting me in this work. -

Achievement of Three Years
SUSTAINABLE DEVELOPMENT THROUGH KUDUMBASHREE CDS Report from Perinthalmanna CDS 2018-2020 Report submitted by, Sarika. S State Assistant Programme Manager - Tribal Kudumbashree State Mission 1 Perinthalmanna Perinthalmanna is a municipality in Malappuram district of Kerala. It was the capital of Valluvanad, a princely state ruled by the Valluvakonathiris, a suspected branch of the Pallava dynasty of the ancient Tamil kingdoms. Thirumandhamkunnu Bhagavathi Temple and Tali Mahadeva temple are located at Angadipuram, 3 km north of the town. Perinthalmanna became a Panchayath in 1933. Later upgraded to municipality on 10 February 1990. As of 2011 India census, Perinthalmanna had a population of 49,723 spreading an area of 34 sq km. The municipal area is divided into 31 administration wards. Perinthalmanna is a prominent and fast-developing settlement in the district. The town is equidistant, at approximately 70 Km, from Palakkad, Thrissur and Kozhikode cities. The Kozhikode-Palakkad Road (NH 966) and the Perumbilavu-Nilambur Road (SH 9 & 23) meet at the Main Junction of Perinthalmanna. This geographic positioning and connectivity with all important settlements in the region has been catalystic to the growth of this town. This strong connectivity has attracted higher level facilities to the town. But this also means a heavy volume of through-traffic that adds to the chaos in the town. Perinthalmanna is located near the southern boundary of Malappuram District, along National Highway 966. The town is well connected by roads to the other important towns in the district like Malappuram, Manjeri, Nilambur, Kottakkal, Pattambi and Shornur and the neighbouring LSGs Angadippuram, Vettathur, Thazhekkode, Alipparamba, Elamkulam and Pulamanthole. -

Classical Arts/Kathakali/Son G
BLOCK PANCHAYATHS/MUNICIPALITIES/CORPORATIONS ALLOTTED TO THE FELLOWSHIP ARTISTS Block Panchayat/Municipal Sl No Name Address Art Category District Taluk ity/Corporation where the artist is deployed ULLADAMPARAMBIL, KALAVOOR Classical Arts P.O. AMBALAPPUZHA TALUK, 1 REMYA R / Music Alappuzha Ambalappuzha Ambalappuzha ALAPPUZHA DIST PIN 688522 / Vocal AMBANAKULANGARA VELI MANNANCHERRY P O Classical Arts / 2 VINSHIA S AMBALAPPUZHA ALAPPUZHA - 688 Dance/Mohiniyatta Alappuzha Ambalappuzha Ambalappuzha 538 m Classical SIVASADANAM, KAROOR, Arts/Kathakali/Son AMBALAPUZHA.P.O ALAPPUZHA, 3 KRISHNAKUMAR M N g Alappuzha Ambalappuzha Ambalappuzha 688561 Vijay Bhavan, NR Tharayil L.P.S. 4 Reshmi V Ponakam, Mavelikara 690101 Finearts /Painting Alappuzha Mavelikkara Bharanikkavu RETHEESH BHAVAN, KOLLAKADAVU P.O. KOLLAKADAVU, Folklore Arts / Folk 5 REJITHA RAJAN TALUK - CHENGANNUR DIST. Alappuzha Chenganoor Bharanikkavu ALAPPUZHA - 690509 song ALATHOOR HOUSE KODIYATTUKARA CHENGANNUR Folklore Arts / 6 HARIKRISHNAN M G Alappuzha Chenganoor Bharanikkavu ALAPPUZHA 689121 Vanchipattu MANOLIL HOUSE EDANAD P.O. Folklore Arts / 7 HARISH KUMAR M. S. CHENGANNUR ALAPPUZHA 689 123 Alappuzha Chengannur Chengannoor Vanchipattu kunnileparambil nadukkethil, puliyoor p Classical Arts / 8 AISWARYA o, chengannur, alappuzha, kerala Dance/Mohiniyatta Alappuzha Chengannur Chenganoor m CHERUVELIL ILLAM PANDANAD WEST PO CHENGANNUR, 9 SREEKUMAR C N Finearts /Painting Alappuzha Chengannur Chenganoor ALAPUZHA 689506 Classical Arts NISHADHAM, VARANAD.P.O, / Kathakali / CHERTHALA,