Written Public Comments for the October 2017 IACC Meeting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Animated Roots of Wildlife Films: Animals, People
THE ANIMATED ROOTS OF WILDLIFE FILMS: ANIMALS, PEOPLE, ANIMATION AND THE ORIGIN OF WALT DISNEY’S TRUE-LIFE ADVENTURES by Robert Cruz Jr. A thesis submitted in partial fulfillment of the requirements for the degree of Master of Fine Arts in Science and Natural History Filmmaking MONTANA STATE UNIVERSITY Bozeman, Montana April 2012 ©COPYRIGHT by Robert Cruz Jr. 2012 All Rights Reserved ii APPROVAL of a thesis submitted by Robert Cruz Jr. This thesis has been read by each member of the thesis committee and has been found to be satisfactory regarding content, English usage, format, citation, bibliographic style, and consistency and is ready for submission to The Graduate School. Dennis Aig Approved for the School of Film and Photography Robert Arnold Approved for The Graduate School Dr. Carl A. Fox iii STATEMENT OF PERMISSION TO USE In presenting this thesis in partial fulfillment of the requirements for a master’s degree at Montana State University, I agree that the Library shall make it available to borrowers under rules of the Library. If I have indicated my intention to copyright this thesis by including a copyright notice page, copying is allowable only for scholarly purposes, consistent with “fair use” as prescribed in the U.S. Copyright Law. Requests for permission for extended quotation from or reproduction of this thesis in whole or in parts may be granted only by the copyright holder. Robert Cruz Jr. April 2012 iv TABLE OF CONTENTS 1. INTRODUCTORY QUOTES .....................................................................................1 -
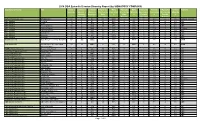
2014 DGA Episodic Director Diversity Report (By SIGNATORY COMPANY)
2014 DGA Episodic Director Diversity Report (by SIGNATORY COMPANY) Signatory Company Title Total # of Combined # Combined # Episodes Male # Episodes Male # Episodes Female # Episodes Female Network Episodes Women + Women + Directed by Caucasian Directed by Minority Directed by Caucasian Directed by Minority Minority Minority % Male % Male % Female % Female % Episodes Caucasian Minority Caucasian Minority 50/50 Productions, LLC Workaholics 13 0 0% 13 100% 0 0% 0 0% 0 0% Comedy Central ABC Studios Betrayal 12 1 8% 11 92% 0 0% 1 8% 0 0% ABC ABC Studios Castle 23 3 13% 20 87% 1 4% 2 9% 0 0% ABC ABC Studios Criminal Minds 24 8 33% 16 67% 5 21% 2 8% 1 4% CBS ABC Studios Devious Maids 13 7 54% 6 46% 2 15% 4 31% 1 8% Lifetime ABC Studios Grey's Anatomy 24 7 29% 17 71% 1 4% 2 8% 4 17% ABC ABC Studios Intelligence 12 4 33% 8 67% 4 33% 0 0% 0 0% CBS ABC Studios Mixology 12 0 0% 13 108% 0 0% 0 0% 0 0% ABC ABC Studios Revenge 22 6 27% 16 73% 0 0% 6 27% 0 0% ABC And Action LLC Tyler Perry's Love Thy Neighbor 52 52 100% 0 0% 52 100% 0 0% 0 0% OWN And Action LLC Tyler Perry's The Haves and 36 36 100% 0 0% 36 100% 0 0% 0 0% OWN The Have Nots BATB II Productions Inc. Beauty & the Beast 16 1 6% 15 94% 0 0% 1 6% 0 0% CW Black Box Productions, LLC Black Box, The 13 4 31% 9 69% 0 0% 4 31% 0 0% ABC Bling Productions Inc. -

Shameless Sociology
Shameless Sociology Shameless Sociology: Critical Perspectives on a Popular Television Series Edited by Jennifer Beggs Weber and Pamela M. Hunt Shameless Sociology: Critical Perspectives on a Popular Television Series Edited by Jennifer Beggs Weber and Pamela M. Hunt This book first published 2020 Cambridge Scholars Publishing Lady Stephenson Library, Newcastle upon Tyne, NE6 2PA, UK British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Copyright © 2020 by Jennifer Beggs Weber, Pamela M. Hunt and contributors All rights for this book reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the copyright owner. ISBN (10): 1-5275-5744-8 ISBN (13): 978-1-5275-5744-4 For Nathan, my partner in crime. – Jennifer For Perry and Grace. – Pam TABLE OF CONTENTS Acknowledgments ..................................................................................... ix Introduction ................................................................................................ 1 Pamela M. Hunt and Jennifer Beggs Weber Part 1: Social Class Dominant Hasslin’ and Subordinate Hustlin’: A Content Analysis Using the Generic Processes that Reproduce Inequality ............................ 8 Alexis P. Hilling, Erin Andro, and Kayla Cagwin Shamefully Shameless: Critical Theory and Contemporary Television ... 29 Robert J. Leonard and Kyra -

Mark Wagner's Stunt Resume
Mark Aaron Wagner HEIGHT: 5’10” Weight: 165 lbs. Stuntman / Stunt Coordinator/ Actor S.A.G./ A.F.T.R.A./ U.B.C.P./ A.C.T.R.A Suit- 38-40R, Shirt- 16x34 International Stunt Association- 818-501-5225 Waist- 32, Inseem- 31 KMR (agent)- (818) 755-7534 Shoe: 10 www.MarkAaronWagner.com (Online Demo) Current Resume on IMDB.com Feature Films (Full List Upon Request) Once Upon a Time in Hollywood Zoë Bell/ Rob Alonzo Captain Marvel (driver) Hank Amos/ Jeff Habberstad Ant-Man and The Wasp (dbl. Paul Rudd) Brycen Counts Peppermint (stunt dbl.) Keith Woulard Deadpool 2 (driver) Owen Walstrom/ Darrin Prescott Bright Rob Alonzo Predator Marny Eng/ Lance Gilbert Captain America: Civil War (dbl.- Paul Rudd) Sam Hargrave/ Doug Coleman Three Billboards (dbl.- Sam Rockwell) Doug Coleman PeeWee’s Big Holiday (dbl.- Paul Reubens) Mark Rayner Maze Runner: Scorch Trials ND George Cottle Ant-Man (dbl.- Paul Rudd) Jeff Habberstad Stretch (dbl.- Patrick Wilson) Ben Bray Captain America: Winter Soldier Strike Agent Tom Harper/ Casey O’Neil 300: Rise of an Empire Artemisia Father Damon Caro Iron Man 3 Extremis Soldier Markos Rounthwaite/ Mike Justus/ Jeff Habberstad Secret Life of Walter Mitty (dbl.- Adam Scott) Tim Trella/ Clay Cullen Dark Knight Rises ND/ Driving Tom Struthers/ George Cottle Gangster Squad (dbl.-Frank Grillo) Doug Coleman Men in Black 3 ND Wade Eastwood/ Simon Crane X-Men: First Class MIB Jeff Habberstad/ Brian Smrz Girl with the Dragon Tattoo Drving Jeff Habberstad This Is 40 (dbl.- Paul Rudd) Joel Kramer The Master (dbl.- Joaquin Phoenix) Garrett -

Shameless Television: Gendering Transnational Narratives
This is a repository copy of Shameless television: gendering transnational narratives. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/129509/ Version: Accepted Version Article: Johnson, B orcid.org/0000-0001-7808-568X and Minor, L (2019) Shameless television: gendering transnational narratives. Feminist Media Studies, 19 (3). pp. 364-379. ISSN 1468-0777 https://doi.org/10.1080/14680777.2018.1468795 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Shameless Television: Gendering Transnational Narratives Beth Johnson ([email protected]) and Laura Minor ([email protected]) School of Media and Communication, University of Leeds, Leeds, UK Abstract The UK television drama Shameless (Channel 4, 2004-2011) ran for eleven series, ending with its 138th episode in 2011. The closing episode did not only mark an end, however, but also a beginning - of a US remake on Showtime (2011-). Eight series down the line and carrying the weight of critical acclaim, this article works to consider the textual representations and formal constructions of gender through the process of adaptation. -

STUART JOHNSON Electrician/Film&TV Lighting Gaffer
STUART JOHNSON Electrician/Film&TV Lighting Gaffer 07708720366 [email protected] Imdb Stuart Johnson XIII J I B Registered electrician City and Guilds Electrical Installation Part I 1996 & Part II 1997 AM1 & AM2 1998. Vocational Qualification 050(NVQ) 1998. Royal Air Force City and Guilds Electrical/Electronics Competences 2001. 17th Edition IEE Wiring Regs. Full driving licence, HGV Class 2. Ipaf cherry picker licence. 2018 James Arthur & Anne Marie (music vid) Gaffer, Dop Sam Meyer. https://youtu.be/pRfmrE0ToTo Little Joe (Feature Film) Best boy, Gaffer Werner Stibitz. Bureau Films Ltd. The Valley of the Fox (German TV Film) Best boy, Gaffer Roland Schnitter. UFA Fiction Germany. Paul Pogba World Cup interview (Fox USA) Gaffer. Dop Adam Docker, Red Earth Studio. Cancer Awareness (Commercial) Gaffer. Dop Adam Gillham, MTP Ltd. Man City (Spirable promo) Gaffer. The Mob Films. Jessica Hennis-Hill Adidas (Promo) Gaffer. WeAreSocial Ltd. Tadashi Izumi (Japanese promo vid) Gaffer. Turn Productions Ltd. Uber with Mo Salah (Commercial) Rigging Gaffer. WigWam Films. https://youtu.be/-u4jqI4J_yg Angry birds @ Everton FC with Wayne Rooney (Promo) Lighting Tech. The Mob Films. Adidas The Answer (Commercial) Lighting Tech. Iconoclast TV. Gucci (Commercial) Lighting Tech. North Six Europe Ltd. Aleixis Sanchez Man U (Signing promo) Lighting Tech. The Mob Films. Moving on 10 (TV Drama) Lighting Tech. Dop Len Gowing. LA Productions. 2017 The Zoo (Feature Film) Gaffer. DOP Damien Elliott. Northern Ireland, Wee Bun films. https://youtu.be/TSNMPCG8m5M The Souvenir Pt1 (Feature Film). Gaffer. DOP David Raedekker. Cheated (German Feature Film) Best Boy. Gaffer Roland Schnitter. UFA Fiction Germany. Moving on 9 (TV Drama) Best Boy. -

Surgery in Norway a Comprehensive Review at the 100-Year Jubilee of !E Norwegian Surgical Society 1911–2011
Surgery in Norway A Comprehensive Review at the 100-year Jubilee of !e Norwegian Surgical Society 1911–2011 Internet-version - corrected according to suggestions from the members of the Norwegian Surgical Societies, who received a printed “working” version in 2011. Editors: Jon Ha!ner, Tom Gerner and Arnt Jakobsen Copyright 2011: The Norwegian Surgical Association, Oslo Internet version 2012 ISBN nr: 978-82-8070-093-3 Preface The Norwegian Surgical Society was founded on the First The present book is written by leading surgeons in the of August in 1911. The main reason was discontent with different specialties, and all the manuscripts have been the surgeons’ wages and working conditions, but in 1924 reviewed and commented on by other prominent surgeons the focus changed to the scientific aspects of surgery, and to ensure objectivity. membership was opened to surgeons in training. Since then the Society has had annual meetings with free presentations, The initial manuscript was printed and distributed to all mem- and debates about surgical methods, education, specialisa- bers of the surgical societies in Norway (totally 2250) in 2011 tion, leadership, and working conditions. The social aspect for corrections and comments. The present Internet edition has also been important, an annual dinner has been ar- has been corrected according to the comments received, and an ranged since 1925. extra chapter on former Chairmen and Boards of The Norwe- gian Surgical Society/ Assosciation has been added. In 2006 the Society was renamed The Norwegian Surgical Association, with the chairmen of the other surgical socie- The initial manuscript was printed and distributed to all ties as board members. -

European Society for Paediatric Research Annual Meeting Abstracts Bilbao, Spain September 27–30, 2003
0031-3998/03/5404-0557 PEDIATRIC RESEARCH Vol. 54, No. 4, 2003 Copyright © 2003 International Pediatric Research Foundation, Inc. Printed in U.S.A. EUROPEAN SOCIETY FOR PAEDIATRIC RESEARCH ANNUAL MEETING ABSTRACTS BILBAO, SPAIN SEPTEMBER 27–30, 2003 0008NEO 0011NEO PRESCHOOL OUTCOME IN CHILDREN BORN VERY PREMATURELY EFFICACY OF ERYTHROPOITIN IN PREMATURE INFANTS AND CARED FOR ACCORDING TO NIDCAP Adnan Amin, Daifulah Alzahrani Bjo¨rn Westrup1, Birgitta Bo¨hm1, Hugo Lagercrantz1, Karin Stjernqvist2 Alhada Military Hospital City:Taif, Saudi Arabia 1Neonatal Programme, Dept. of Woman and Child Health, Astrid Lindgren Children’s Hospital, Objective: To identify the effect of early of parentral recombinant human erythropoitin (r-HuEPO) Karolinska Institute, Stockholm, Sweden;2Depts. of Psychology and of Paediatrics, University of and iron administration on blood transfusion requirement of premature infants. Methods: In a Lund, Sweden City: Stockholm and Lund, Sweden controlled clinical trial conducted at the Neonatal Intensive Care Unit, Al-Hada Military Hospital, Background/aim: Care based on the Newborn Individualized Developmental Care and Assess- Taif, Kingdom of Saudi Arabia over a 16 month period. We assigned 20 very low birth weight infants ment Program (NIDCAP) has been reported to exert a positive impact on the development of (VLBW) with gestational age of (mean Ϯ SEM 28.4 Ϯ 0.5 weeks and birth weight of (mean Ϯ SEM prematurely born infants. The aim of the present investigation was to determine the effect of such care 1031 Ϯ 42 gm), to receive either intravenous (r-HuEPO 200 U/kg/day) and iron 1mg/kg/day or on the development at preschool age of children born with a gestational age of less than 32 weeks. -

The First Golden Minute Ola Didrik Saugstad 2O Congreso Argentino
The first Golden Minute Delivery room handling of newborn infants Ola Didrik Saugstad, MD, PhD, FRCPE University of Oslo and Oslo University Hospital Norway Email: odsaugstad@[email protected] 2o Congreso Argentino de Neonatologia, Buenos Aires, June 27-29, 20013 Delivery Room Stabilisation Delivery room management •Adequate preparation •Cord clamping •Free airways •Maintenance of neutral thermal environment •Appro priate use of supplemental oxygen •Non invasive respiratory support •Timely administration of surfactant •Teamwork and communication New European Guidelines On Management of RDS Sweet D et al Neonatology 2013;103:353-368 Outline of lecture •The golden minute(s) •Suctioning Vs wiping •Cord clamping •Thermal control •Oxygenation •CPAP/Surfactant •Gentle resuscitation/stabilization The Golden Minute: Helping Babies Breathe Drying/stimulating Suctioning Ventilation Assessment 10% need help to breathe within «the golden minute» ILCOR Neonatal Resuscitation Guidelines 2010 The golden minute Perlman J et al, Circulation 2010;122 (Suppl 2) S516-538 The Golden Minute(s) Cold and Oxygen Flow V PDA Ventilation Chorioamnionitis rate T Dry Gas Oxygen Antenatal Delivery Steroids Pregnancy Room Postnatal Care Outcome Managementt Pre-eclampsia Nutrition PEEP Surfactant Temp. Sepsis Nutrition Others control 5- 9 months 15-30 min Weeks ‐months years Modified from Alan Jobe Stabilization or resuscitation „Most premature babies are not dead and therefore do not need „resuscitation“ They need assistance in transition and adaptation -

Oral and Written Public Comments
Public Comments July 21-22, 2021 1 Table of Contents Oral Comments ............................................................................................................................................. 4 Christopher Banks on behalf of The Autism Society of America .................................................................. 5 Jill Escher, J.D., M.A. on behalf of National Council on Severe Autism ........................................................ 7 Bin Feng ....................................................................................................................................................... 10 Kelly Israel on behalf of Autistic Self Advocacy Network ............................................................................ 11 Noemi Spinazzi on behalf of M.D., Down syndrome-Autism workgroup of the Down Syndrome Medical Interest Group ............................................................................................................................................. 15 Written Comments ..................................................................................................................................... 16 Oren Evans .................................................................................................................................................. 17 Ramey Chisum............................................................................................................................................. 18 Resa Warner ............................................................................................................................................... -

International Academy of Perinatal Medicine (Iapm)
History, Organization and Activities PREFACE Organization and Activities History, he International Academy of Perina- by Prof. Erich Saling, President of IAPM. tal Medicine (IAPM) was created in T 2005, with the agreement of the Presi- FOREWORD dents of three scientific societies: the by José M. Carrera, Secretary General ) World Association of Perinatal Medicine of IAPM. (WAPM), the European Association of Peri- CHAPTER 1 natal Medicine (EAPM) and the Internatio- The History of Perinatal Medicine. nal Society «The Fetus as a Patient» (ISFAP). IAPM ( th On the 25 of May 2005 took place the CHAPTER 2 foundational ceremony in Barcelona The fathers of Perinatal Medicine: (Spain) with venue at the Royal Academy the academic medals. of Medicine of Catalonia. CHAPTER 3 The objective of the Academy is to create a Identity and mission of International place for the studystudy, reflection, dialogue Academy of Perinatal Medicine (IAPM). INTERNATIONAL and prpromotionomotion of PPerinatal Medicine, es- CHAPTER 4 pecially on those ississues related to bioethics, History of International Academy the appropriate appapplication of the techno- of Perinatal Medicine (IAPM): ACADEMY logical advances aand the sociologic and the foundation. huhumanisticmanistic ddimensionsimensi of the fi eld. CHAPTER 5 OF PERINATAL Furthermore, the AAcademy endeavours to Constitution of IAPM and By-Laws. constitute a friendshfriendship-based bond among ththee ththreeree scscientificientifi Societies that have CHAPTER 6 sponsored its foundfoundation. Basic Organization of the IAPM. MEDICINE In the same act oof the foundation, the CHAPTER 7 members of the BBoard of the Academy The International Council: were elected. Prof. Erich Saling (Germany) Regular Fellows of IAPM. (IAPM) was elected as President,Pre and Professors CHAPTER 8 Asim Kurjak (Croati(Croatia), Aris Antsaklis (Gree- Honorary Members ce), Frank ChervenaChervenak (USA) and H. -
Transcript for the IACC Full Committee Meeting on July 9, 2013
1 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES INTERAGENCY AUTISM COORDINATING COMMITTEE FULL COMMITTEE MEETING TUESDAY, JULY 9, 2013 The Interagency Autism Coordinating Committee (IACC) met in Room 10, Sixth Floor, C Wing, Building 31, 31 Center Drive, Bethesda, Maryland, from 9:09 a.m. until 5:28 p.m., Thomas Insel, Chair, presiding. PRESENT: THOMAS INSEL, M.D., Chair, IACC, National Institute of Mental Health (NIMH) SUSAN DANIELS, Ph.D., Executive Secretary, IACC, NIMH IDIL ABDULL, Somali American Autism Foundation JAMES BALL, Ed.D., BCBA-D, JB Autism Consulting and Autism Society of America (attended by phone) ANSHU BATRA, M.D., Our Special Kids JAMES BATTEY, M.D., Ph.D., National Institute on Deafness and Other Communication Disorders (NIDCD) 2 PRESENT (continued): LINDA BIRNBAUM, Ph.D., National Institute of Environmental Health Sciences (NIEHS) (attended by phone) COLEEN BOYLE, Ph.D., M.S.Hyg., U.S. Centers for Disease Control and Prevention (CDC) JOSEPHINE BRIGGS, M.D., National Center for Complementary and Alternative Medicine (NCCAM) SALLY BURTON-HOYLE, Ed.D., Eastern Michigan University MATTHEW CAREY, Ph.D., Left Brain Right Brain (attended by phone) JAN CRANDY, Nevada State Autism Treatment Assistance Program and Nevada Commission on Autism Spectrum Disorders GERALDINE DAWSON, Ph.D., Duke University DENISE DOUGHERTY, Ph.D., Agency for Healthcare Research and Quality (AHRQ) TIFFANY FARCHIONE, M.D., U.S. Food and Drug Administration (FDA) ALAN GUTTMACHER, M.D., Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) LAURA KAVANAGH, M.P.P., Health Resources and Services Administration (HRSA) DONNA KIMBARK, Ph.D., U.S.