Covidview Key Updates for Week 52, Ending December 26, 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Division of Personnel Employee Information and Payroll Audit Section
Division of Personnel Employee Information and Payroll Audit Section This document is provided as a service to state agencies. Note: The 90-day interval includes both the beginning and ending dates. 90-DAY (WEEKDAYS) INTERVAL CALENDAR FOR 2012 JANUARY JANUARY 2 '12 MONDAY MAY 4 '12 FRIDAY JANUARY 3 TUESDAY MAY 7 MONDAY JANUARY 4 WEDNESDAY MAY 8 TUESDAY JANUARY 5 THURSDAY MAY 9 WEDNESDAY JANUARY 6 FRIDAY MAY 10 THURSDAY JANUARY 9 MONDAY MAY 11 FRIDAY JANUARY 10 TUESDAY MAY 14 MONDAY JANUARY 11 WEDNESDAY MAY 15 TUESDAY JANUARY 12 THURSDAY MAY 16 WEDNESDAY JANUARY 13 FRIDAY MAY 17 THURSDAY JANUARY 16 MONDAY MAY 18 FRIDAY JANUARY 17 TUESDAY MAY 21 MONDAY JANUARY 18 WEDNESDAY MAY 22 TUESDAY JANUARY 19 THURSDAY MAY 23 WEDNESDAY JANUARY 20 FRIDAY MAY 24 THURSDAY JANUARY 23 MONDAY MAY 25 FRIDAY JANUARY 24 TUESDAY MAY 28 MONDAY JANUARY 25 WEDNESDAY MAY 29 TUESDAY JANUARY 26 THURSDAY MAY 30 WEDNESDAY JANUARY 27 FRIDAY MAY 31 THURSDAY JANUARY 30 MONDAY JUNE 1 '12 FRIDAY JANUARY 31 TUESDAY JUNE 4 MONDAY FEBRUARY FEBRUARY 1 '12 WEDNESDAY JUNE 5 '12 TUESDAY FEBRUARY 2 THURSDAY JUNE 6 WEDNESDAY FEBRUARY 3 FRIDAY JUNE 7 THURSDAY FEBRUARY 6 MONDAY JUNE 8 FRIDAY FEBRUARY 7 TUESDAY JUNE 11 MONDAY FEBRUARY 8 WEDNESDAY JUNE 12 TUESDAY FEBRUARY 9 THURSDAY JUNE 13 WEDNESDAY FEBRUARY 10 FRIDAY JUNE 14 THURSDAY FEBRUARY 13 MONDAY JUNE 15 FRIDAY FEBRUARY 14 TUESDAY JUNE 18 MONDAY FEBRUARY 15 WEDNESDAY JUNE 19 TUESDAY FEBRUARY 16 THURSDAY JUNE 20 WEDNESDAY FEBRUARY 17 FRIDAY JUNE 21 THURSDAY FEBRUARY 20 MONDAY JUNE 22 FRIDAY FEBRUARY 21 TUESDAY JUNE 25 MONDAY FEBRUARY -
Whats Good Events Guide December 5-8 2019 Gainesville and Alachua
WHAT’S GOOD. ALACHUA | ARCHER | GAINESVILLE | HAWTHORNE | HIGH SPRINGS | LA CROSSE | MICANOPY | NEWBERRY | WALDO Plan your weekend with the official events guide from Visit Gainesville, Alachua County December 5-8, 2019 Enjoy a Magical Holiday Theatrical Performance for the Entire Family at Spirit of the Horse Friday, December 6 – Saturday, December 7, 7 p.m. – 9 p.m., Sunday, December 8, 6 p.m. – 8 p.m. | Alachua County Agriculture and Equestrian Center 23100 W Newberry Rd., Newberry, FL 32669 Experience an inspiring holiday story that is sure to delight and entertain. This show is in its tenth year, enjoyed by audiences around the country, and 2019 marks the premiere of Spirit of the Horse in Florida. Admission is FREE FOR VETERANS with valid ID. Food available from BubbaQue’s BBQ. Browse Unique Gifts from More Than 200 Vendors at the 51st Annual Craft Festival Saturday, December 7 – Sunday, December 8, 10 a.m. – 5 p.m. | O’Connell Center 250 Gale Lemerand Dr., Gainesville, FL 32611 Find something special for yourself or that hard to shop for person in your life. The festival has been a holiday tradition for the past 51 years and is the largest indoor craft fair in North Central Florida. Watch Santa Arrive by Helicopter at Operation Santa Delivery Saturday, December 7, 10 a.m. – 1 p.m. | Santa Fe College North Field 3700 NW 91st St., Gainesville, FL 32606 Santa will visit Gainesville not by reindeer and sleigh, but by helicopter. Enjoy games, music, food and fun activities. Helicopter Photo by the Gainesville Sun. -

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -
Cboe to Observe National Day of Mourning on Wednesday, December 5, 2018
Cboe to Observe National Day of Mourning on Wednesday, December 5, 2018 Reference ID: C2018120300 Overview To honor the memory of former President George H.W. Bush, Cboe will be observing the National Day of Mourning scheduled for Wednesday, December 5, 2018. Set forth below are the trading and settlement schedules Cboe options, equities, and futures exchanges will follow this week. Cboe Equities Exchange Trading Schedules Cboe BYX Exchange, BZX Exchange, EDGA Exchange, and EDGX Exchange will be closed for trading on Wednesday, December 5, 2018. Normal trading will resume on Thursday, December 6. Cboe Options Exchange Trading Schedules Cboe Options Exchange, BZX Options Exchange, C2 Options Exchange, and EDGX Options Exchange will be closed for trading on Wednesday, December 5, 2018. Normal trading will resume on Thursday, December 6. Options Settlement Schedule The chart below reflects the changes to options settlement calculation day. Regular ***Regular Option Expiration Exercise Last Settlement Modified/Updated ***Updated Settlement Option Type Type Style Trading Calculation Last Trade Day Calculation Day Day Day Wednesday ETP Wednesday Weekly PM Wednesday Tuesday Tuesday EOD EOD Wednesday Index Wednesday Weekly PM Wednesday Tuesday Tuesday EOD EOD Wednesday Volatility Index Weekly AM Tuesday Tuesday Thursday SOQ SOQ Wednesday Index and Equity FLEX Wednesday PM Wednesday Tuesday Tuesday EOD EOD ***EOD indicates settlement occurs at the EOD based on the official closing price. ***SOQ will be conducted on Thursday versus Wednesday. The exchanges will issue a separate regulatory circular when information regarding exercise advice and contra exercise advice cut-off times becomes available. Settlement of Weekly VIX Options The final settlement value for the VIX weekly options with an expiration date of December 5, 2018 normally would have been determined by a Special Opening Quotation (SOQ) in constituent Standard & Poor’s (S&P) 500 (SPX) option series on Cboe Options Exchange on December 5, 2018. -
Payroll Calendar 2021
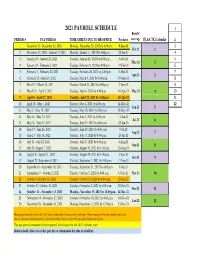
2021 PAYROLL SCHEDULE 1 Benefit PERIOD # PAY PERIOD TIME SHEETS DUE TO HR OFFICE Paydates coverage FLSA 7K Calendar 2 1 December 13- December 26, 2020 Monday, December 28, 2020 by 4:00 p.m. 8-Jan-21 3 Feb-21 1 2 December 27, 2020 - Janurary 9, 2021 Monday, January 11, 2021 by 4:00 p.m. 22-Jan-21 4 3 January 10 - January 23, 2021 Tuesday, January 26, 2021 by 4:00 p.m. 5-Feb-21 5 Mar-21 2 4 January 24 - February 6, 2021 Tuesday, February 9, 2021 by 4:00 p.m. 19-Feb-21 6 5 February 7 - February 20, 2021 Tuesday, February 26, 2021 by 4:00 p.m. 5-Mar-21 7 Apr-21 3 6 February 21 - March 6, 2021 Tuesday, March 9, 2021 by 4:00 p.m. 19-Mar-21 8 7 March 7 - March 20, 2021 Tuesday, March 23, 2021 by 4:00 p.m. 2-Apr-21 9 8 March 21 - April 3, 2021 Tuesday, April 6, 2021 by 4:00 p.m. 16-Apr-21 May-21 4 10 9 April 4 - April 17, 2021 Tuesday, April 20, 2021 by 4:00 p.m. 30-Apr-21 11 10 April 18 - May 1, 2021 Tuesday, May 4, 2021 by 4:00 p.m. 14-May-21 12 Jun-21 5 11 May 2 - May 15, 2021 Tuesday, May 18, 2021 by 4:00 p.m. 28-May-21 12 May 16 - May 29, 2021 Tuesday, June 1, 2021 by 4:00 p.m. 11-Jun-21 Jul-21 6 13 May 30 - June 12, 2021 Tuesday, June 15, 2021 by 4:00 p.m. -
2019 Payroll Calendar
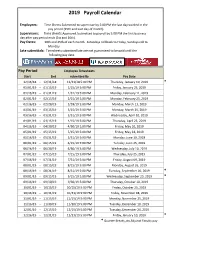
2019 Payroll Calendar Employees: Time Sheets Submitted to supervisor by 5:00 PM the last day worked in the pay period (15th and Last day of month). Supervisors: Time sheets Approved /submitted to payroll by 5:00 PM the first business day after pay period ends (1st and 16th). Pay Dates: 10th and 25th of each month. Saturdays roll back to Friday, Sundays roll to Monday. Late submittals: Timesheets submitted late are not guaranteed to be paid until the following pay date. Pay Period Employee Timesheets Start End submitted By Pay Date 12/16/18 - 12/31/18 12/31/18 5:00 PM Thursday, January 10, 2019 * 01/01/19 - 01/15/19 1/15/19 5:00 PM Friday, January 25, 2019 01/16/19 - 01/31/19 1/31/19 5:00 PM Monday, February 11, 2019 02/01/19 - 02/15/19 2/15/19 5:00 PM Monday, February 25, 2019 02/16/19 - 02/28/19 2/28/19 5:00 PM Monday, March 11, 2019 03/01/19 - 03/15/19 3/15/19 5:00 PM Monday, March 25, 2019 03/16/19 - 03/31/19 3/31/19 5:00 PM Wednesday, April 10, 2019 04/01/19 - 04/15/19 4/15/19 5:00 PM Thursday, April 25, 2019 04/16/19 - 04/30/19 4/30/19 5:00 PM Friday, May 10, 2019 05/01/19 - 05/15/19 5/15/19 5:00 PM Friday, May 24, 2019 05/16/19 - 05/31/19 5/31/19 5:00 PM Monday, June 10, 2019 06/01/19 - 06/15/19 6/15/19 5:00 PM Tuesday, June 25, 2019 06/16/19 - 06/30/19 6/30/19 5:00 PM Wednesday, July 10, 2019 07/01/19 - 07/15/19 7/15/19 5:00 PM Thursday, July 25, 2019 07/16/19 - 07/31/19 7/31/19 5:00 PM Friday, August 09, 2019 08/01/19 - 08/15/19 8/15/19 5:00 PM Monday, August 26, 2019 08/16/19 - 08/31/19 8/31/19 5:00 PM Tuesday, September 10, -

BILLING CYCLE SCHEDULE Department of Procurement, Disbursements & Contract Services 1135 Old Main 600 Lincoln Avenue Charleston, IL 61920
Eastern Illinois University BILLING CYCLE SCHEDULE Department of Procurement, Disbursements & Contract Services 1135 Old Main 600 Lincoln Avenue Charleston, IL 61920 Billing Cycle Beginning Date Billing Cycle Ending Date June 26, 2018 July 25, 2018 Tuesday Wednesday July 26, 2018 August 24, 2018 Thursday Friday August 26, 2018 September 25, 2018 Sunday Tuesday September 26, 2018 October 25, 2018 Wednesday Thursday October 26, 2018 November 26, 2018 Friday Monday November 27, 2018 December 26, 2018 Tuesday Wednesday December 27, 2018 January 25, 2019 Thursday Friday January 26, 2019 February 25, 2019 Saturday Monday February 26, 2019 March 25, 2019 Tuesday Monday March 26, 2019 April 25, 2019 Tuesday Thursday April 26, 2019 May 24, 2019 Friday Friday May 26, 2019 June 25, 2019 Sunday Tuesday June 26, 2019 July 25, 2019 Wednesday Thursday Revised 2/2/18 1 Transactions with a Post Date of: Must be Reviewed Upload to Banner & Approved by: July 1, 2018 – July 6, 2018 July 12, 2018 July 13, 2018 Thursday Friday July 7, 2018 – July 13, 2018 July 19, 2018 July 20, 2018 Thursday Friday July 14, 2018 – July 20, 2018 July 26, 2018 July 27, 2018 Thursday Friday July 21, 2018 – July 27, 2018 August 2, 2018 August 3, 2018 Thursday Friday July 28, 2018 – August 3, 2018 August 9, 2018 August 10, 2018 Thursday Friday August 4, 2018 – August 10, 2018 August 16, 2018 August 17, 2018 Thursday Friday August 11, 2018 – August 17, 2018 August 23, 2018 August 24, 2018 Thursday Friday August 18, 2018 – August 24, 2018 August 30, 2018 August 31, 2018 Thursday -

Julian Date Cheat Sheet for Regular Years
Date Code Cheat Sheet For Regular Years Day of Year Calendar Date 1 January 1 2 January 2 3 January 3 4 January 4 5 January 5 6 January 6 7 January 7 8 January 8 9 January 9 10 January 10 11 January 11 12 January 12 13 January 13 14 January 14 15 January 15 16 January 16 17 January 17 18 January 18 19 January 19 20 January 20 21 January 21 22 January 22 23 January 23 24 January 24 25 January 25 26 January 26 27 January 27 28 January 28 29 January 29 30 January 30 31 January 31 32 February 1 33 February 2 34 February 3 35 February 4 36 February 5 37 February 6 38 February 7 39 February 8 40 February 9 41 February 10 42 February 11 43 February 12 44 February 13 45 February 14 46 February 15 47 February 16 48 February 17 49 February 18 50 February 19 51 February 20 52 February 21 53 February 22 54 February 23 55 February 24 56 February 25 57 February 26 58 February 27 59 February 28 60 March 1 61 March 2 62 March 3 63 March 4 64 March 5 65 March 6 66 March 7 67 March 8 68 March 9 69 March 10 70 March 11 71 March 12 72 March 13 73 March 14 74 March 15 75 March 16 76 March 17 77 March 18 78 March 19 79 March 20 80 March 21 81 March 22 82 March 23 83 March 24 84 March 25 85 March 26 86 March 27 87 March 28 88 March 29 89 March 30 90 March 31 91 April 1 92 April 2 93 April 3 94 April 4 95 April 5 96 April 6 97 April 7 98 April 8 99 April 9 100 April 10 101 April 11 102 April 12 103 April 13 104 April 14 105 April 15 106 April 16 107 April 17 108 April 18 109 April 19 110 April 20 111 April 21 112 April 22 113 April 23 114 April 24 115 April -

Nevada Gaming Statistics: December Historical Comparison Summary of 10-Year Revenue Trends
Nevada Gaming Statistics: December Historical Comparison Summary of 10-Year Revenue Trends This report compares monthly Nevada gaming results for December over the past ten years for selected reporting areas: Statewide, Las Vegas Strip, Downtown Las Vegas, Boulder Strip, and Washoe County. December 2020 was an overall negative month for Las Vegas gaming revenues, with increases in many reporting areas. Statewide Las Vegas Strip Downtown LV Boulder Strip Washoe County Total win -35.35% -50.66% -27.93% -24.61% -11.81% Slot win -34.43% -54.69% -41.57% -24.34% -8.57% Slot handle -26.60% -43.17% -43.30% -17.44% -11.99% Game win -37.14% -45.89% 0.61% -26.72% -25.17% Game handle -35.36% -43.99% 7.70% -29.23% -20.05% Bacc win -16.98% -15.69% n/a n/a n/a Bacc handle -49.51% -49.97% n/a n/a n/a Tables for Statewide, Las Vegas Strip, Downtown Las Vegas, Boulder Strip, and Washoe County follow. Questions? Contact the Center for Gaming Research at (702) 895-2234 or [email protected] University Libraries University of Nevada, Las Vegas Nevada Gaming Statistics: December Historical Comparison Statewide figures for the month of December, 2011-2020 Dec-11 Dec-12 Dec-13 Dec-14 Dec-15 Dec-16 Dec-17 Dec-18 Dec-19 Dec-20 Change% Total Revenue 855,664 943,304 1,034,024 950,692 982,061 956,095 960,384 999,665 1,057,603 683,733 -35.35% Slot Revenue 480,863 492,185 557,721 559,151 565,464 547,296 579,724 635,880 700,142 459,024 -34.43% Slot Handle 9,265,183 9,269,021 8,995,500 9,091,886 9,135,121 9,387,581 9,792,635 9,873,913 10,103,059 7,415,574 -26.60% -

Ril May June July August September October
NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY DECEMBER NOVEMBER OCTOBER SEPTEMBER AUGUST JULY JUNE MAY APRIL MARCH FEBRUARY JANUARY NOVEMBER DECEMBER JANUARY -

2021 Calendar Campaign
One Tail at a Time 2021 Calendar Pets Date Status Date Status Date Status Date Status Date Status Date Status Date Status Date Status Friday, January 1 Not Available Saturday, February 20 Not Available Sunday, April 11 Available Monday, May 31 Not Available Tuesday, July 20 Available Wednesday, September 8 Not Available Thursday, October 28 Available Thursday, December 16 Available Saturday, January 2 Available Sunday, February 21 Available Monday, April 12 Not Available Tuesday, June 1 Available Wednesday, July 21 Not Available Thursday, September 9 Available Friday, October 29 Available Friday, December 17 Available Sunday, January 3 Available Monday, February 22 Available Tuesday, April 13 Available Wednesday, June 2 Available Thursday, July 22 Not Available Friday, September 10 Available Saturday, October 30 Available Saturday, December 18 Not Available Monday, January 4 Available Tuesday, February 23 Available Wednesday, April 14 Available Thursday, June 3 Available Friday, July 23 Available Saturday, September 11 Available Sunday, October 31 Not Available Sunday, December 19 Available Tuesday, January 5 Available Wednesday, February 24 Available Thursday, April 15 Not Available Friday, June 4 Available Saturday, July 24 Available Sunday, September 12 Available Monday, November 1 Available Monday, December 20 Available Wednesday, January 6 Available Thursday, February 25 Available Friday, April 16 Not Available Saturday, June 5 Available Sunday, July 25 Available Monday, September 13 Available Tuesday, November 2 Available Tuesday, -

FDA Briefing Document: Pfizer-Biontech COVID-19 Vaccine
Vaccines and Related Biological Products Advisory Committee Meeting December 10, 2020 FDA Briefing Document Pfizer-BioNTech COVID-19 Vaccine Sponsor: Pfizer and BioNTech Table of Contents List of Tables ............................................................................................................................. 3 List of Figures ............................................................................................................................ 4 Glossary..................................................................................................................................... 5 1. Executive Summary ............................................................................................................... 6 2. Background ............................................................................................................................ 7 2.1. SARS-CoV-2 Pandemic ................................................................................................ 7 2.2. EUA Request for the Pfizer and BioNTech COVID-19 Vaccine BNT162b2 .................... 8 2.3. U.S. Requirements to Support Issuance of an EUA for a Biological Product ........................................................................................................................... 8 2.4. Applicable Guidance for Industry ................................................................................... 9 2.5. Safety and Effectiveness Information Needed to Support an EUA ................................. 9 2.6. Continuation