Understanding Bladder Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Bladder Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis
cancer.org | 1.800.227.2345 Bladder Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Finding cancer early, when it's small and hasn't spread, often allows for more treatment options. Some early cancers may have signs and symptoms that can be noticed, but that's not always the case. ● Can Bladder Cancer Be Found Early? ● Bladder Cancer Signs and Symptoms ● Tests for Bladder Cancer Stages and Outlook (Prognosis) After a cancer diagnosis, staging provides important information about the extent (amount) of cancer in the body and the likely response to treatment. ● Bladder Cancer Stages ● Survival Rates for Bladder Cancer Questions to Ask About Bladder Cancer Here are some questions you can ask your cancer care team to help you better understand your cancer diagnosis and treatment options. ● Questions To Ask About Bladder Cancer 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Can Bladder Cancer Be Found Early? Bladder cancer can sometimes be found early -- when it's small and hasn't spread beyond the bladder. Finding it early improves your chances that treatment will work. Screening for bladder cancer Screening is the use of tests or exams to look for a disease in people who have no symptoms. At this time, no major professional organizations recommend routine screening of the general public for bladder cancer. This is because no screening test has been shown to lower the risk of dying from bladder cancer in people who are at average risk. Some providers may recommend bladder cancer tests for people at very high risk, such as: ● People who had bladder cancer before ● People who had certain birth defects of the bladder ● People exposed to certain chemicals at work Tests that might be used to look for bladder cancer Tests for bladder cancer look for different substances and/or cancer cells in the urine. -

Continent Urostomy Guide
$POUJOFOU6SPTUPNZ(VJEF "QVCMJDBUJPOPGUIF6OJUFE0TUPNZ"TTPDJBUJPOTPG"NFSJDB *OD i4FJ[FUIF 0QQPSUVOJUZw CONTINENT UROSTOMY GUIDE Ilene Fleischer, MSN, RN, CWOCN, Author Patti Wise, BSN, RN, CWOCN, Author Reviewed by: Authors and Victoria A.Weaver, RN, MSN, CETN Revised 2009 by Barbara J. Hocevar, BSN,RN,CWOCN, Manager, ET/WOC Nursing, Cleveland Clinic © 1985 Ilene Fleischer and Patti Wise This guidebook is available for free, in electronic form, from United Ostomy Associations of America (UOAA). UOAA may be contacted at: www.ostomy.org • [email protected] • 800-826-0826 CONTENTS INTRODUCTION . 3 WHAT IS A CONTINENT UROSTOMY? . 4 THE URINARY TRACT . 4 BEFORE THE SURGERY . .5 THE SURGERY . .5 THE STOMA . 7 AFTER THE SURGERY . 7 Irrigation of the catheter(s) 8 Care of the drainage receptacles 9 Care of the stoma 9 Other important information 10 ROUTINE CARE AT HOME . 10 Catheterization schedule 11 How to catheterize your pouch 11 Special considerations when catheterizing 11 Care of the catheter 12 Other routine care 12 HELPFUL HINTS . .13 SUPPLIES FOR YOUR CONTINENT UROSTOMY . 14 LIFE WITH YOUR CONTINENT UROSTOMY . 15 Clothing 15 Diet 15 Activity and exercise 15 Work 16 Travel 16 Telling others 17 Social relationships 17 Sexual relations and intimacy 17 RESOURCES . .19 GLOSSARY OF TERMS . 20 BIBLIOGRAPHY . .21 1 INTRODUCTION Many people have ostomies and lead full and active lives. Ostomy surgery is the main treatment for bypassing or replacing intestinal or urinary organs that have become diseased or dysfunctional. “Ostomy” means opening. It refers to a number of ways that bodily wastes are re-routed from your body. A urostomy specifi cally redirects urine. -
Cystectomy (Bladder Removal) with Ileal Conduit Urinary Diversion
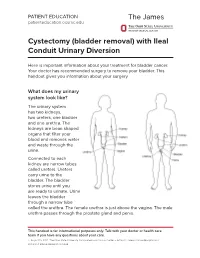
PATIENT EDUCATION patienteducation.osumc.edu Cystectomy (bladder removal) with Ileal Conduit Urinary Diversion Here is important information about your treatment for bladder cancer. Your doctor has recommended surgery to remove your bladder. This handout gives you information about your surgery. What does my urinary system look like? The urinary system has two kidneys, two ureters, one bladder and one urethra. The kidneys are bean shaped organs that filter your blood and removes water and waste through the urine. Connected to each kidney are narrow tubes called ureters. Ureters carry urine to the bladder. The bladder stores urine until you are ready to urinate. Urine leaves the bladder through a narrow tube called the urethra. The female urethra is just above the vagina. The male urethra passes through the prostate gland and penis. This handout is for informational purposes only. Talk with your doctor or health care team if you have any questions about your care. © August 19, 2021. The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute. Cystectomy (bladder removal) with Ileal Conduit Urinary Diversion A cystectomy is surgery to remove the bladder. In men, the prostate, seminal vesicles and lymph nodes may also be removed. In women, the ovaries, fallopian tubes, uterus, cervix, vagina, urethra and lymph nodes may be removed. Your doctor will talk with you about the surgery and what is best for you. After the bladder is removed, your doctor will make a new urinary system. One option is an ileal conduit, also called a urostomy. This will direct your urine to drain through a small opening in your abdomen (belly) called a “stoma”. -
Clinical Usefulness of Urine Cytology in the Detection of Bladder Tumors in Patients with Neurogenic Lower Urinary Tract Dysfunction
Journal name: Research and Reports in Urology Article Designation: ORIGINAL RESEARCH Year: 2017 Volume: 9 Research and Reports in Urology Dovepress Running head verso: Pannek et al Running head recto: Cytology for bladder tumor detection in neurogenic bladder open access to scientific and medical research DOI: http://dx.doi.org/10.2147/RRU.S148429 Open Access Full Text Article ORIGINAL RESEARCH Clinical usefulness of urine cytology in the detection of bladder tumors in patients with neurogenic lower urinary tract dysfunction Jürgen Pannek Introduction: Screening for bladder cancer in patients with neurogenic lower urinary tract Franziska Rademacher dysfunction is a challenge. Cystoscopy alone is not sufficient to detect bladder tumors in this Jens Wöllner patient group. We investigated the usefulness of combined cystoscopy and urine cytology. Materials and methods: By a systematic chart review, we identified all patients with neuro- Neuro-Urology, Swiss Paraplegic Center, Nottwil, Switzerland genic lower urinary tract dysfunction who underwent combined cystoscopy and urine cytology testing. In patients with suspicious findings either in cytology or cystoscopy, transurethral resection was performed. Results: Seventy-nine patients (age 54.8±14.3 years, 38 female, 41 male) were identified; 44 of these used indwelling catheters. Cystoscopy was suspicious in 25 patients and cytology was suspicious in 17 patients. Histologically, no tumor was found in 15 patients and bladder cancer was found in 6 patients. Sensitivity for both cytology and cystoscopy was 83.3%; specificity was 43.7% for cytology and 31.2% for cystoscopy. One bladder tumor was missed by cytology and three tumors were missed by cystoscopy. If a biopsy was taken only if both findings were suspicious, four patients would have been spared the procedure, and one tumor would not have been diagnosed. -

Complications of Urinary Diversion
Complications of Urinary Diversion Jennifer L. Dodson, M.D. Department of Urology Johns Hopkins University Types of Diversion Conduit Diversions Ileal conduit Colon conduit Continent Diversions Continent catheterizable reservoir Continent rectal pouch 1 Overview of Complications Mechanical Stoma problems Bowel obstruction Ureteral obstruction Reservoir perforation Metabolic Altered absorption Altered bone metabolism Growth delay Stones Cancer Conduit Diversions Ileal Conduit: Technically simplest Segment of choice Colon Conduit: Transverse or sigmoid Used when ileum not appropriate (eg: concomitant colon resection, abdominal radiation, short bowel syndrome, IBD) Early complications (< 30 days): 20-56% Late complications : 28-81% Risks: abdominal radiation abdominal surgery poor nutrition chronic steroids Farnham & Cookson, World J Urol, 2004 2 Complications of Ileal Conduit Campbell’s Urology, 8th Edition, 2002 Conduit: Bowel Complications Paralytic ileus 18-20% Conservative management vs NGT Consider TPN Bowel obstruction 5-10% Causes: Adhesions, internal hernia Evaluation: CT scan, Upper GI series Anastomotic leak 1-5 % Risk factors: bowel ischemia, radiation, steroids, IBD, technical error Prevention: Pre-operative bowel prep Attention to technical detail Stapled small-bowel Anastomosis (Campbell’s Blood supply, tension-free anastomosis, Urology, 8th Ed, 2004) realignment of mesentery Farnham & Cookson, World J Urol, 2004 3 Conduit Complications Conduit necrosis: Acute ischemia to bowel -

EAU Guidelines on Bladder Stones 2019
EAU Guidelines on Bladder Stones C. Türk (Chair), A. Skolarikos (Vice-chair), J.F. Donaldson, A. Neisius, A. Petrik, C. Seitz, K. Thomas Guidelines Associate: Y. Ruhayel © European Association of Urology 2019 TABLE OF CONTENTS PAGE 1. INTRODUCTION 3 1.1 Aims and Scope 3 1.2 Panel Composition 3 1.3 Available Publications 3 1.4 Publication History and Summary of Changes 3 1.4.1 Publication History 3 2. METHODS 3 2.1 Data Identification 3 2.2 Review 4 3. GUIDELINES 4 3.1 Prevalence, aetiology and risk factors 4 3.2 Diagnostic evaluation 4 3.2.1 Diagnostic investigations 5 3.3 Disease Management 5 3.3.1 Conservative treatment and Indications for active stone removal 5 3.3.2 Medical management of bladder stones 5 3.3.3 Bladder stone interventions 5 3.3.3.1 Suprapubic cystolithotomy 5 3.3.3.2 Transurethral cystolithotripsy 5 3.3.3.2.1 Transurethral cystolithotripsy in adults: 5 3.3.3.2.2 Transurethral cystolithotripsy in children: 6 3.3.3.3 Percutaneous cystolithotripsy 6 3.3.3.3.1 Percutaneous cystolithotripsy in adults: 6 3.3.3.3.2 Percutaneous cystolithotripsy in children: 6 3.3.3.4 Extracorporeal shock wave lithotripsy (SWL) 6 3.3.3.4.1 SWL in Adults 6 3.3.3.4.2 SWL in Children 6 3.3.4 Treatment for bladder stones secondary to bladder outlet obstruction (BOO) in adult men 7 3.3.5 Urinary tract reconstructions and special situations 7 3.3.5.1 Neurogenic bladder 7 3.3.5.2 Bladder augmentation 7 3.3.5.3 Urinary diversions 7 4. -
Urinary Sample Collection Methods in Ileal Conduit Urinary Diversion Patients a Randomized Control Trial Markku H
Ostomy Care Ostomy Care J Wound Ostomy Continence Nurs. 2018;45(1):59-62. Published by Lippincott Williams & Wilkins Urinary Sample Collection Methods in Ileal Conduit Urinary Diversion Patients A Randomized Control Trial Markku H. Vaarala ABSTRACT PURPOSE: The purpose of this study was to compare bacteriological urinalysis findings using 3 urinary sample collection methods (clean stoma catheterization, urine dripping from the stoma, urine collected from the clean urostomy pouch) in ileal conduit urinary diversion patients. DESIGN: Randomized controlled trial. SAMPLE AND SETTING: Twenty-seven patients with ileal conduit urinary diversion from an outpatient urology clinic were enrolled; 9 patients were seen twice, for a total of 36 subjects and comparisons. METHODS: Data were collected during a clinic visit by a trained research nurse. Patients were randomized into 2 groups: group A had the first urine sample collected by clean stoma catheterization, followed by sample collection by urine dripping from the stoma; group B had the first urine sample collection by urine dripping from the stoma, followed by sample collected by clean stoma catheterization. All patients had a third urine sample collected from a factory-clean urostomy pouch. Bacteriological urinalysis findings were compared among methods. Descriptive analyses were summarized using mean, percentage, and frequency. The mean ages of the patients between the groups were compared with the t test. Other between-group comparisons were performed using the Fisher exact test. Urinary culture finding differences among the same patients were evaluated using the McNemar test. Sensitivity and specificity of the different urine sample collection methods were calculated assuming urine sample collection by catheterization as a reference method. -

EAU Guidelines on the Diagnosis and Treatment of Urothelial Carcinoma in Situ Adrian P.M
European Urology European Urology 48 (2005) 363–371 EAU Guidelines EAU Guidelines on the Diagnosis and Treatment of Urothelial Carcinoma in Situ Adrian P.M. van der Meijdena,*, Richard Sylvesterb, Willem Oosterlinckc, Eduardo Solsonad, Andreas Boehlee, Bernard Lobelf, Erkki Rintalag for the EAU Working Party on Non Muscle Invasive Bladder Cancer aDepartment of Urology, Jeroen Bosch Hospital, Nieuwstraat 34, 5211 NL ’s-Hertogenbosch, The Netherlands bEORTC Data Center, Brussels, Belgium cDepartment of Urology, University Hospital Ghent, Ghent, Belgium dDepartment of Urology, Instituto Valenciano de Oncologia, Valencia, Spain eDepartment of Urology, Helios Agnes Karll Hospital, Bad Schwartau, Germany fDepartment of Urology, Hopital Ponchaillou, Rennes, France gDepartment of Urology, Helsinki University Hospital, Helsinki, Finland Accepted 13 May 2005 Available online 13 June 2005 Abstract Objectives: On behalf of the European Association of Urology (EAU), guidelines for the diagnosis, therapy and follow-up of patients with urothelial carcinoma in situ (CIS) have been established. Method: The recommendations in these guidelines are based on a recent comprehensive overview and meta-analysis in which two panel members have been involved (RS and AVDM). A systematic literature search was conducted using Medline, the US Physicians’ Data Query (PDQ), the Cochrane Central Register of Controlled Trials, and reference lists in trial publications and review articles. Results: Recommendations are provided for the diagnosis, conservative and radical surgical treatment, and follow- up of patients with CIS. Levels of evidence are influenced by the lack of large randomized trials in the treatment of CIS. # 2005 Elsevier B.V. All rights reserved. Keywords: Bladder cancer; Carcinoma in situ; Bacillus Calmette-Guerin; Chemotherapy; Diagnosis; Treatment; Follow up 1. -

The Morbidity Due to Lower Urinary Tract Function in Spinal Cord Injury Patients
Paraplegia 31 (1993) 320-329 © 1993 International Medical Society of Paraplegia The morbidity due to lower urinary tract function in spinal cord injury patients P E V Van Kerrebroeck MD PhD, E L Koldewijn MD, S Scherpcnhuizen, F M J Debruyne MD PhD Department of Urology, Unit for Neurourology and Urodynamics, University Hospital St Radboud, Geert Grooteplein Zuid 16, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. A review is given of 105 patients with a traumatic spinal cord injury. In 93 patients with a minimum follow up of one year the morbidity due to lower urinary tract function was evaluated, based on the situation at their last control visit. The relation was studied between bladder behaviour and the type of urine evacuation and their influence on upper urinary tract problems, urinary tract infections, stone formation and incontinence. Based on the results of this study the most appropriate method for control of bladder behaviour and urine evacuation in spinal cord injured patients is discussed in view of new treatment modalities such as dorsal rhizotomies and the implantation of an anterior sacral root stimulator. Keywords: spinal cord injuries; neurogenic lower urinary tract dysfunction; morbidity. Introduction daily practice proves that the control of individual patients tends to be less scrupul Great progress has been made during the ous with time. Even in the published pros last 25 years in the urological rehabilitation pective series the incidence of urological of patients with a spinal cord injury. problems varies much depending on the Nevertheless these patients continue to follow up, the composition of the patient develop complications such as urinary groups and the treatment(s) that were prop tract infections, stones of the upper and osed. -
Ucsf Urology Transitional Urology Clinic
UCSF UROLOGY TRANSITIONAL UROLOGY CLINIC Thank you for choosing the UCSF Transitional Urology Clinic. This clinic was created to serve patients with urologic conditions diagnosed in childhood as they become adults and need to transition to an adult urology practice. Our clinic is jointly run by pediatric and adult urology to provide comprehensive urologic follow-up and healthcare for adults with congenital urologic conditions. This clinic specializes in treating people with congenital urologic conditions like: • Spina bifida • Vesicoureteral reflux • Neurogenic bladder • Hypospadias • Bladder exstrophy/epispadias • Prune belly syndrome • Disorders of sex development • Posterior urethral valves • Cloacal anomalies • Childhood urologic cancers At the first visit, you will be seen jointly by Dr. Copp (a pediatric urologist) and Dr. Hampson (an adult reconstructive urologist). The goal is to thoroughly review your urologic care to-date, and to establish a plan moving forward. Part of this includes understanding your goals as well, so please let us know if there are particular issues you would like addressed at your visit. Follow-up visits will be with Dr. Hampson, with pediatric urologists involved on an as-needed basis. We ask that you complete the following new patient questionnaire to give us the necessary information to provide you with the best possible care. Your answers will help us better understand your situation and guide our decisions about what treatments are best for you. GENERAL INFORMATION: Patient Name: Date of appointment: -

Urine Cytological Examination
F1000Research 2019, 8:1878 Last updated: 28 JUL 2021 RESEARCH ARTICLE Urine cytological examination: an appropriate method that can be used to detect a wide range of urinary abnormalities [version 1; peer review: 1 approved, 1 approved with reservations] Emmanuel Edwar Siddig 1-3, Nouh S. Mohamed 4-6, Eman Taha Ali7,8, Mona A. Mohamed4, Mohamed S. Muneer 9-11, Abdulla Munir6, Ali Mahmoud Mohammed Edris8,12, Eiman S. Ahmed1, Lubna S. Elnour2, Rowa Hassan 1,13 1Mycetoma Research Center, University of Khartoum, Sudan, Khartoum, 11111, Sudan 2Faculty of Medical Laboratoy Sciences, University of Khartoum, Sudan, Khartoum, 11111, Sudan 3School of Medicine, Nile University, Sudan, Khartoum, 11111, Sudan 4Department of Parasitology and Medical Entomology, Nile university, Sudan, Khartoum, 11111, Sudan 5Department of Parasitology and Medical Entomology, Sinnar University, Sinnar, Sinnar, 11111, Sudan 6National University Research Institute, National University, Sudan, Khartoum, 11111, Sudan 7Department of Histopathology and Cytology, National University, Sudan, Khartoum, 11111, Sudan 8Department of Histopathology and Cytology, University of Khartoum, Sudan, Khartoum, 11111, Sudan 9Department of Neurology, Mayo Clinic in Florida, USA, Fl, USA 10Department of Radiology, Mayo Clinic in Florida, USA, USA 11Department of Internal Medicine, University of Khartoum, Sudan, Khartoum, 11111, Sudan 12Faculty of Applied Medical Sciences, University of Bisha, Saudi Arabia, Bisha, Saudi Arabia 13Global Health and Infection Department, Brighton and Sussex Medical School, United Kingdom, UK v1 First published: 07 Nov 2019, 8:1878 Open Peer Review https://doi.org/10.12688/f1000research.20276.1 Latest published: 07 Nov 2019, 8:1878 https://doi.org/10.12688/f1000research.20276.1 Reviewer Status Invited Reviewers Abstract Background: Urine cytology is a method that can be used for the 1 2 primary detection of urothelial carcinoma, as well as other diseases related to the urinary system, including hematuria and infectious version 1 agents. -
1 an Ileal Conduit Urinary Diversion Some Practical Questions
An Ileal Conduit Urinary Diversion Some practical questions & answers with Nancy, a bladder cancer survivor with an Ileal Conduit. An ileal conduit is a system of urinary drainage which a surgeon creates using the small intestine after removing the bladder. To do this, the surgeon takes a short segment of the small intestine and places it at an opening he has made on the surface of the abdomen to create a mouth, or stoma. The ureters, which normally carry urine from the kidneys to the bladder, are then attached to the other end of the segment of intestine. The urine now travels from the kidneys, via the ureters and the newly formed ileal conduit, to the stoma and out into a collecting pouch known as an ostomy bag (or urostomy.) This is worn outside the body around the stoma 24 hours a day. Because the nerves and blood supply are preserved, the new conduit is able to propel the urine out of the body and into the urostomy. Tell us about Recuperation after the Surgery Nancy: One of the advantages of the ileal conduit is that it requires less surgical time than other, more complex, diversions. This procedure was developed during the 1940’s and is still the most used technique for urinary diversion. When I was released from the hospital, I came home with no tubes or catheters. I had no diet restrictions because only a small part of the intestine is used. However, I understand many doctors will recommend a low residue diet for the first few weeks post op.