Urinalysis for Dummies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Brief Overview of Urology's Development
A brief overview of urology’s development Milestones in urology show evolutionary growth Prof. Manuel Mendes upper urinary tract diseases, namely kidney disease, Modern advances Silva with Albarran’s invention of a moveable “lever” for Advances continue to be made, not only in Former president adjusting the cystoscope, making it possible to insert fundamental aspects of the basic sciences, but also in Portuguese tubes (catheters) up into the ureters and kidneys. This new and sophisticated methods of diagnosis and Association of Urology made it possible to analyse the urine produced by treatment. These include computerised imaging Lisbon (PT) each kidney separately, thereby facilitating lateral techniques: ultrasound, computed axial tomography diagnosis. The most common diseases of the time, of (CAT), magnetic resonance imaging (MRI), digital and which tuberculosis was the most prevalent, were very Doppler angiography, radioactive isotopes; analytical, mmendessilva@ different from those we see today. immunological, genetic and pathology-based sapo.pt methods of diagnosis; sophisticated tools for studying urodynamics; new methods of endoscopic and laser “...it was only toward the end of the diagnosis and treatment, such as endourology Urinary and genital diseases have been around since century, after electricity came into (ureterorenoscopy, percutaneous surgery), internal time immemorial. We know this from the evidence and external shockwave lithotripsy, laparoscopy and left behind –urinary stones discovered in Egyptian use, that Max Nitze (1877) achieved laparoscopic surgery, and robotic surgery and mummies and alongside numerous skeletal remains- a good quality cystoscopy using a telesurgery; control of infection with vaccines and and in vestiges of ancient civilisations such as new generation antibiotics; new techniques for paintings and writing tablets. -

The Effect of Medicine, in Particular the Ideas About Renal Diseases, on the “Well-Being” of Byzantine Citizens
93 A TH A N A SIOS D I A M A N D OPOULOS The Effect of Medicine, in particular the Ideas about Renal Diseases, on the “Well-being” of Byzantine Citizens At first sight it is rather strange that a conference on “Material Culture and Well-Being in Byzantium” should include a topic about a medical specialty. Medicine, tiptoeing hesitantly between the realm of sci- ences and that of humanities, is not automatically classified as “Material Culture”. On second thoughts, there are arguments from medicine’s past and present, which plead in favour of such an inclusion. The most famous of all the existing ancient medical Greek codices is the Materia Medica, which was written by the 1st cent. AD medical writer Dioscurides, and then copied in Constantinople, at the beginning of the 6th cent1. As its title shows, medicine cannot be practised without the use of material substances, the medicaments, which are minutely listed in the text. It is tempting, however, to add, that Galen the most pro- lific and most self-assured of all ancient medical writers, found Dioscurides᾽s Greek grossly inferior, but he, at least, accepted that the medical information in Materia Medica was correct. On the other hand the over-all aim of medicine is to prevent the destruction of people’s sense of well-being and to restore it when in decline during times of a disease. Hence, I think that such a topic is relevant to the conference. Before we proceed to the specific role of nephrology (i.e. the medical specialty dealing with kidney ailments) I will present some general characteristics of Byzantine medicine, and I will outline why an interest in it has arisen3. -
Bilirubin Metabolism
Bilirubin Metabolism By Aseel .j.abdullah Introduction • Bilirubin is the orange-yellow pigment derived from senescent red blood cells. • It is a toxic waste product in the body. • It is extracted and biotransformed mainly in the liver, and excreted in bile and urine. • It is a bile pigment • Elevations in serum and urine bilirubin levels are normally associated with Jaundice. Erythrocytes become “old” as they lose their flexibility and increasingly rigid and fragile,they easily destruct during passage through tight circulation spots, especially in spleen, where the intra-capillary space is about 3 micron as compared to 8 micron of cell size RBCs useful life span is 100 to 120 days,After which they become trapped and fragment in smaller circulatory channels, particularly in those of the spleen. For this reason, the spleen is sometimes called the “red blood cell graveyard.” Dying erythrocytes are engulfed and destroyed by macrophages. Formation of Bilirubin • Primary site of synthesis:- SPLEEN : The Graveyard of Red Blood Cells • Secondary site of synthesis:- LIVER & BONE MARROW Pathophysiology RBCs Breakdown Hemoglobin Produces & Breakdown Heme Heme Oxygenase Biliverdin Biliverdin Reductase Bilirubin In Blood Unconjugated bilirubin • The bilirubin synthesized in – Lipid soluble spleen, liver & bone marrow – : limits excretion is unconjugated bilirubin. – 1 gm albumin binds 8.5 mg bilirubin • It is hydrophobic in nature so – Fatty acids & drugs can it is transported to the liver displace bilirubin as a complex with the – Indirect positive reaction plasma protein, albumin. in van den Bergh test • Most of the reabsorbed urobilinogen is taken up by the liver & is re-excreted in the bile. -

Medieval Uroscopy and Its Representation on Misericords – Part 1: Uroscopy
n MEDICAL HISTORY Medieval uroscopy and its representation on misericords – Part 1: uroscopy Henry Connor ABSTRACT– The art of uroscopy involved the recognise these differences, and thereby make a diag- Henry Connor MD visual inspection of urine in a specially shaped nosis, by reference to instructions and charts which FRCP, Consultant flask called a matula. By the fourteenth century it were initially in manuscript and later in printed Physician, County had become an integral part of the assessment of form3,4,6,7 (Figure 1). The original texts were in Latin, Hospital, Hereford the patient’s humoral balance, which was the and therefore only comprehensible to the educated, linchpin of both diagnosis and management in but from about 1375 there was an explosion of Clin Med JRCPL medieval medical practice, and the matula vernacular medical texts written in Medieval 2001;1:507–9 became the symbol of a physician. However, the English7,8. One of those on uroscopy was probably practice was open to abuse by unscrupulous the work of John Lelamour, a master at the cathedral physicians, who offered treatment solely on the school in Hereford, who in 1373 had translated a basis of uroscopy without even seeing the Latin Herbal 9,10 which also served as one of the patient. Further abuse occurred as Latin texts on earliest English texts on gardening 11. the subject were translated into the vernacular by unqualified imposters. Although more orthodox practitioners and the College of Physicians tried hard to distance themselves from the practice, the matula became a symbol of ridicule. Inspection of urine was recorded in the clay tablets of Sumerian and Babylonian physicians of 4000 BC 1, and was advocated by Hippocrates (460–355 BC) and by Galen (AD 129–c200) though, as Hoeniger has emphasised, both limited their diagnostic deduc- tions from examinations of the urine to conditions affecting the kidneys, bladder and urethra 2. -

History of Urinalysis in in Iran
CIN2011 History of Urinalysis by Razi and Avicenna in Iran and Their Clinical Judgment from Urinalysis Behrooz Broumand,M.D.,F.A.C.P. Professor of Medicine IUMS Permanent member Iranian Academy of Medical Sciences Past President Iranian Society of Nephrology Abstract : Urinalysis (Uroscopy) has been performed by physicians from 500 BC. Evidence of this diagnostic procedure can be found in the works of Hippocrates, Aristotle, Galen and a few others. Liquid Gold described as “ one’s water used to be considered a divine fluid, a window into the body and soul.” [1] Meanwhile, uroscopy had become a tool in the hands of uneducated people for fortune telling, to the point that Thomas Brian published the book titled “The Piss Prophet”, a book against abuses of uroscopy. [2] Abu Baker Muhammad ibn Zakariy ā R āzī (Rhazes or Rasis, 865 AD-925 AD) and Ab ū Al ī al- Ḥusayn ibn Abd All āh ibn S īnā (Avicenna 980 to 1037 AD) were amongst a few scientists who pioneered in performing urinalysis in scientific methods very similar to what is customary in the 21st century, except they did not have access to microscopes to examine for the presence of different cells or crystals. These scientists were not only examining the urine for the detection and diagnosis of renal diseases, but in their interpretation they would also judge the function of other organs and their relation to the quality of urine. Key words: Iran, History of medicine, Medieval, Ancient, Urinalysis Preface: Medical notes, from several thousands years ago, have revealed that examination and observation of urine was the first tool for diagnosis of illness and management of patients. -
The Judgement of Urines
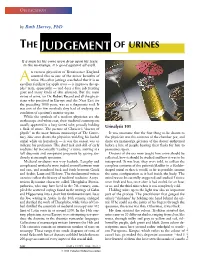
OBFUSCATION by Ruth Harvey, PhD THE JUDGEMENT OF URINES If a man let his owne uryn drop upon his feete in the mornynge, it is good agaynst all evyll. n earnest physician of Renaissance England counted this as one of the minor benefits of A urine. His other jottings concluded that it is an excellent fertilizer for apple trees — it improves the ap- ples’ taste, apparently — and does a fine job treating gout and many kinds of skin ailments. But the main virtue of urine, for Dr. Robert Record and all the physi- cians who practised in Europe and the Near East for the preceding 1000 years, was as a diagnostic tool. It was one of the few methods they had of studying the condition of a patient’s interior organs. While the symbols of a modern physician are the stethoscope and white coat, their medieval counterparts usually appeared in a long furred robe, proudly holding Urinalysis 101 a flask of urine. The picture of Chaucer’s “doctor of physik” in the most famous manuscript of The Canter- It was axiomatic that the first thing to be shown to bury Tales even shows the physician wielding his loaded the physician was the contents of the chamber pot, and urinal while on horseback — it was the easiest way to there are manuscript pictures of the doctor enthroned indicate his profession. The chief task and skill of early before a line of people bearing their flasks for him to medicine lay in correctly “reading” a urine: arriving at a pronounce upon. full diagnosis and competent prognosis by gazing stu- Doctors of the era were taught how urine should be diously at an ample specimen. -
Fate of Rbc's
HEMOGLOBIN AND HEMOGLOBINOPATHIES LECTURE 01 FATE OF RBCS AND JAUNDICE LECTURE 02 & 03 HEMOGLOBIN FIRST YEAR MBBS 2020 Features of a Mature RBC • Biconcave disc • Mean Diameter 7.8 um • Can deform easily. • Bag of fluid with dissolved substances and hemoglobin • No sub cellular particles • Metabolism – Anaerobic respiration- Glycolysis – Pentose phosphate pathway. RBC Count • Remains remarkably constant although there are some variations. • MALE : 5.2 ± 0.3 x 106 /uL. • FEMALE : 4.7 ± 0.3 x 106 /uL. • Life span : 120 Days HEMOGLOBIN HEME-CONTAINING PROTEINS Hemoglobin Myoglobin Cytochromes Catalase Some peroxidases HEMOGLOBIN • Metallo-conjugate protein • Molecular weight is 64,500 • One hemoglobin molecule is composed of four heme groups (subunits) attached with globin (having four polypeptide chains) • One hemoglobin molecule binds with it four oxygen molecules (eight oxygen atoms) • 1 gm hemoglobin carries 1.34 ml of oxygen • Heme synthesis occurs in the mitochondria of bone marrow erythroblasts HEMOGLOBIN FORMATION 2 succinyl-CoA + 2 glycine Pyrrole 4 pyrrole Protoporphyrin IX Protoporphyrin IX + Fe++ Heme Heme + Polypeptide Hemoglobin chain (α β) 2 α chains + 2 β chains Hemoglobin A Types of Hemoglobin • Variations in Hb subunit chains – W.r.t amino acid composition of polypeptide portion – Alpha, beta, gamma, delta Type of Hb Chain Fraction of total composition Hb HbA α2 β2 90% HbF α2 γ2 < 2% HbA2 α2 δ2 2-5 % HbA1C α2 β2 - Glucose 3-9% Embryonic Hemoglobins • Gower 1 Two zeta & two epsilon chains • Gower 2 Two alpha & two epsilon chains • Portland Two zeta & two gamma chains Embryonic/Minor Hemoglobins Organization of Hemoglobin Genes Developmental changes in Hb Hemoglobin F • Blood of the human fetus normally contains fetal hemoglobin • Its structure is similar to that of hemoglobin A except that the β chains are replaced by γ chains • hemoglobin F is α2γ2. -

Porphyrins and Bile Pigments: Metabolism and Disorders Dr
Porphyrins and bile pigments: metabolism and disorders Dr. Jaya Chaturvedi Porphyrins • Porphyrins are cyclic compounds formed by the linkage of four pyrrole rings through methyne (ÓHC—) bridges.In the naturally occurring porphyrins, various side chains replace the eight numbered hydrogen atoms of the pyrroles. • Porphyrins have had different structures depend on side chains that are attached to each of the four pyrrole rings. For example; Uroporphyrin, coporporphyyrin and protoporphyrin IX (heme). • The most prevalent metalloporphyrin in humans is heme, which consists of one ferrous (Fe2+) iron ion coordinated at the center of the tetrapyrrole ring of protoporphyrin IX. What is bilirubin? •Bilirubin is a yellowish pigment found in bile, a fluid made by the liver. •The breakdown product of Hgb from injured RBCs and other heme containing proteins. •Produced by reticuloendothelial system •Released to plasma bound to albumin •Hepatocytes conjugate it and excrete through bile channels into small intestine. Bilirubin di-glucoronid Structure of heme: • Heme structure: a porphyrin ring coordinated with an atom of iron side chains: methyl, vinyl, propionyl • Heme is complexed with proteins to form: • Hemoglobin, myoglobin and cytochromes Pathway of Heme Biosynthesis. Heme biosynthesis begins in the mitochondria from glycine and succinyl- CoA, continues in the cytosol, and ultimately is completed within the mitochondria. The heme that it produced by this biosynthetic pathway is identified as heme b. PBG: porphobilinogen; ALA: δ- aminolevulinic -

In Vitro DNA-Damaging Effects of Intestinal and Related Tetrapyrroles in Human Cancer Cells
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector EXPERIMENTAL CELL RESEARCH 319 (2013) 536–545 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/yexcr Research Article In vitro DNA-damaging effects of intestinal and related tetrapyrroles in human cancer cells Christine Mo¨lzera,Ã, Barbara Pflegera, Elisabeth Putza, Antonia Roßmanna, Ursula Schwarza, Marlies Wallnera, Andrew C. Bulmerb, Karl-Heinz Wagnera,b aDepartment of Nutritional Sciences, Emerging Field Oxidative Stress and DNA Stability, Faculty of Life Sciences, University of Vienna, Althanstraße 14, 1090 Vienna, Austria bHeart Foundation Research Centre, Griffith Health Institute, Griffith University (Gold Coast Campus), Queensland 4222, Australia article information abstract Article Chronology: Epidemiological studies report a negative association between circulating bilirubin concentra- Received 4 September 2012 tions and the risk for cancer and cardiovascular disease. Structurally related tetrapyrroles also Received in revised form possess in vitro anti-genotoxic activity and may prevent mutation prior to malignancy. 3 December 2012 Furthermore, few data suggest that tetrapyrroles exert anti-carcinogenic effects via induction Accepted 4 December 2012 of cell cycle arrest and apoptosis. To further investigate whether tetrapyrroles provoke DNA- Available online 13 December 2012 damage in human cancer cells, they were tested in the single cell gel electrophoresis assay Keywords: (SCGE). Eight tetrapyrroles (unconjugated bilirubin, bilirubin ditaurate, biliverdin, biliverdin-/ Stercobilin bilirubin dimethyl ester, urobilin, stercobilin and protoporphyrin) were added to cultured Caco2 Urobilin and HepG2 cells and their effects on comet formation (% tail DNA) were assessed. Flow Protoporphyrin cytometric assessment (apoptosis/necrosis, cell cycle, intracellular radical species generation) SCGE assisted in revealing underlying mechanisms of intracellular action. -

Conversion of Amino Acids to Specialized Products
Conversion of Amino Acids to Specialized Products First Lecture Second lecture Fourth Lecture Third Lecture Structure of porphyrins Porphyrins are cyclic compounds that readily bind metal ions (metalloporphyrins)—usually Fe2+ or Fe3+. Porphyrins vary in the nature of the side chains that are attached to each of the four pyrrole rings. - - Uroporphyrin contains acetate (–CH2–COO )and propionate (–CH2–CH2–COO ) side chains; Coproporphyrin contains methyl (–CH3) and propionate groups; Protoporphyrin IX (and heme) contains vinyl (–CH=CH2), methyl, and propionate groups Structure of Porphyrins Distribution of side chains: The side chains of porphyrins can be ordered around the tetrapyrrole nucleus in four different ways, designated by Roman numerals I to IV. Only Type III porphyrins, which contain an asymmetric substitution on ring D are physiologically important in humans. Physiologically important In humans Heme methyl vinyl 1) Four Pyrrole rings linked together with methenyle bridges; 2) Three types of side chains are attached to the rings; arrangement of these side chains determines the activity; 3) Asymmetric molecule 3) Porphyrins bind metal ions to form metalloporphyrins. propionyl Heme is a prosthetic group for hemoglobin, myoglobin, the cytochromes, catalase and trptophan pyrrolase Biosynthesis of Heme The major sites of heme biosynthesis are the liver, which synthesizes a number of heme proteins (particularly cytochrome P450), and the erythrocyte-producing cells of the bone marrow, which are active in hemoglobin synthesis. Heme synthesis occurs in all cells due to the requirement for heme as a prosthetic group on enzymes and electron transport chain. The initial reaction and the last three steps in the formation of porphyrins occur in mitochondria, whereas the intermediate steps of the biosynthetic pathway occur in the cytosol. -

Recent Studies Ofthe Urobilin Problem1
J Clin Pathol: first published as 10.1136/jcp.16.1.1 on 1 January 1963. Downloaded from J. clin. Path. (1963), 16, 1 --Recent studies of the urobilin problem1 C. J. WATSON2 From the Department of Medicine, University of Minnesota Hospital, Minneapolis, Minn. It is now almost a century since Jaffe (1868, 1869) 1961). Sjostrand (1949) demonstrated that this is described urobilin. It would manifestly be an imposi- lost as CO, an important observation not yet tion on your patience if I were to attempt any com- exploited to any extent by clinical investigators. It is prehensive treatment of the ensuing history of this intriguing that the opening of the porphyrin ring to topic, but I shall strive to bring together for you a form bile pigment involves only the ix bridge carbon. few of what seem to me the more important mile- A number of years ago Schwartz and I (Watson and stones in their relation to recent studies. For reasons Schwartz, 1942) converted the bilirubins from each that will become apparent, the term urobilin, both of a series of human fistula biles to urobilinogen, on historical and clinical chemical grounds, is best thence to a crystalline urobilin, which was shown to applied to a group of closely related substances. be the same in all instances, i.e., 9, ax in type. Gray, Under ordinary circumstances the urobilin group is Nicholson, and Nicolaus (1958) at King's College related mainly to destruction of the haemoglobin of Hospital, using a much more elegant and precise circulating red cells. Other possible sources will be method depending on oxidation to monopyrrolic referred to later. -

Nomenclature of Tetrapyrroles
Pure & Appi. Chem. Vol.51, pp.2251—2304. 0033-4545/79/1101—2251 $02.00/0 Pergamon Press Ltd. 1979. Printed in Great Britain. PROVISIONAL INTERNATIONAL UNION OF PURE AND APPLIED CHEMISTRY and INTERNATIONAL UNION OF BIOCHEMISTRY JOINT COMMISSION ON BIOCHEMICAL NOMENCLATURE*t NOMENCLATURE OF TETRAPYRROLES (Recommendations, 1978) Prepared for publication by J. E. MERRITT and K. L. LOENING Comments on these proposals should be sent within 8 months of publication to the Secretary of the Commission: Dr. H. B. F. DIXON, Department of Biochemistry, University of Cambridge, Tennis Court Road, Cambridge CB2 1QW, UK. Comments from the viewpoint of languages other than English are encouraged. These may have special significance regarding the eventual publication in various countries of translations of the nomenclature finally approved by IUPAC-IUB. PROVISIONAL IUPAC—ITJB Joint Commission on Biochemical Nomenclature (JCBN), NOMENCLATUREOF TETRAPYRROLES (Recommendations 1978) CONTENTS Preface 2253 Introduction 2254 TP—O General considerations 2256 TP—l Fundamental Porphyrin Systems 1.1 Porphyrin ring system 1.2 Numbering 2257 1.3 Additional fused rings 1.4 Skeletal replacement 2258 1.5 Skeletal replacement of nitrogen atoms 2259 1.6Fused porphyrin replacement analogs 2260 1.7Systematic names for substituted porphyrins 2261 TP—2 Trivial names and locants for certain substituted porphyrins 2263 2.1 Trivial names and locants 2.2 Roman numeral type notation 2265 TP—3 Semisystematic porphyrin names 2266 3.1 Semisystematic names in substituted porphyrins 3.2 Subtractive nomenclature 2269 3.3 Combinations of substitutive and subtractive operations 3.4 Additional ring formation 2270 3.5 Skeletal replacement of substituted porphyrins 2271 TP—4 Reduced porphyrins including chlorins 4.1 Unsubstituted reduced porphyrins 4.2 Substituted reduced porphyrins.