The New Mexico Medico-Legal Malpractice Panel - an Analysis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

RMJ RESUME 2019.Indd
Ray | Peña | McChristian NOVEMBER 2019 Ray | Peña | McChristian El Paso ATTORNEYS DIRECT DIAL E-MAIL ADDRESS Rebecca H. Alvarez (915) 832-7228 [email protected] 5822 Cromo Drive Chris Borunda 2 (915) 832-7248 [email protected] El Paso, TX 79912 Toll Free (866) 832-7200 Bradley Bartlett (210 820-8439 [email protected] 3 Telephone (915) 832-7200 Merritt Clements (210) 820-8435 [email protected] Facsimile (915) 832-7333 Michael Dean 4, 5, 6 (817) 333-2823 [email protected] Robert Edwards 3 (915) 832-7230 [email protected] Jane R. Elliott 3 (505) 855-6000 [email protected] San Antonio Karl S. Furmaga (210) 820-8432 [email protected] Louis A. Gross (210) 348-1822 [email protected] 700 N. St. Mary’s Street, Daniel H. Hernandez 1,3 (915) 832-7237 [email protected] Suite 800 San Antonio, TX 78205S Jennifer Kaufman (210) 348-1816 [email protected] Toll Free (866) 832-7227 Aldo Lopez (915) 832-7283 [email protected] Telephone (210) 341-3554 Noemi Lopez (915) 832-7243 [email protected] Facsimile (210) 341-3557 Jeffrey T. Lucky 1, 3 (915) 832-7234 [email protected] John W. McChristian, Jr. 1 (817) 333-2820 [email protected] Jeffery W. McElroy 1 (915) 832-7250 [email protected] Fort Worth Kwame K. Mensah1 (915) 832-7224 [email protected] James A. (Jim) Mounts III (915) 832-7253 [email protected] Mallick Tower 101 Summit Avenue, Marissa Olsen (210) 348-1812 [email protected] Suite 705 Randall L. Ordones (210) 820-8431 [email protected] Fort Worth, TX 76102 Joseph G. -

Bostonbarjournala Publication of the Boston Bar Association
FALL 2009 BostonBarJournalA Publication of the Boston Bar Association Timely Justice Threatened by Fiscal Challenges A Move to Streamline the Civil Justice System Crawford Comes to the Lab: Melendez-Diaz and the Scope of the Confrontation Clause Residual Class Action Funds: Supreme Court Identifies IOLTA as Appropriate Beneficiary Challenges and Opportunities for New Lawyers Maintaining Client Confidences: Developments at the Supreme Judicial Court and First Circuit in 2009 If Pro Bono is Not an Option, Consider Volunteering GROW YOUR 401(k) WISELY Six things you won’t hear from other 401(k) providers... We were created as a not-for-profit 1. entity, and we exist to provide a benefit We leverage the buying power of the 2. ABA to eliminate firm expenses and minimize participant expenses Our fiduciary tools help you manage 3. your liabilities and save valuable time Our investment menu has three tiers to 4. provide options for any type of investor, and our average expense is well below the industry average for mutual funds We eliminated commissions, which erode 5. your savings, by eliminating brokers We have benefit relationships with 29 6. state bar and 2 national legal associations.* LEARN HOW No other provider has more than one. YOU CAN * Alabama State Bar Illinois State Bar Association State Bar of Nevada Rhode Island Bar Association GROW YOUR State Bar of Arizona Indiana State Bar Association New Hampshire Bar Association State Bar of Texas Arkansas Bar Association Iowa State Bar Association State Bar of New Mexico Vermont Bar Association -

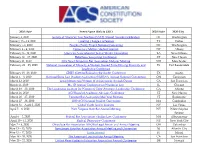
11, 2018 State Bar of New Mexico Annual Meeting
2018-2019 Date Event Name (link to URL) 2019 State 2019 City August 9 - 11, 2018 State Bar of New Mexico Annual Meeting - Bench & Bar Conference NM Bernalillo August 15 - 17, 2018 Eighth Circuit Judicial Conference IA Des Moines August 22 - 24, 2018 Ohio State Bar Association All-Ohio Legal Forum and Annual Meeting OH Columbus August 23 -26, 2018 Veterans for Peace Annual Convention MN St. Paul September 5 - 8, 2018 Hispanic National Bar Association Annual Convention PA Philadelphia September 11 -12, 2018 Congressional Hispanic Caucus Institute Leadership Conference DC Washington September 11 -12, 2018 Congressional Hispanic Caucus Institute Awards Gala DC Washington September 11 - 15, 2018 Council of State Governments West Regional Annual Meeting UT Snowbird September 13 - 15, 2018 Federal Bar Association Annual Meeting and Convention NY NYC September 13 - 15, 2018 National HBCU Pre-Law Summit GA Atlanta September 18 - 21, 2018 Wyoming State Bar Annual Meeting & Judicial Conference WY Laramie September 26 - 29, 2018 The National Association of Minority & Women Owned Law Firms Annual Meeting IL Chicago September 26 -28, 2018 Missouri Bar Annual Meeting and Judicial Conference MO St. Louis September 26 - 28, 2018 NEXT Conference (formerly Annual Meeting/Solo and Small Firm Institute) MI Grand Rapids September 27, 2018 Washington State Bar Association APEX Awards WA Seattle September 27 -29, 2018 The Texas Tribune Festival TX Austin September 28, 2018 MALDEF's San Antonio Awards Gala TX San Antonio September 28 -29, 2018 GRITS (Getting -
List of Conferences and Conventions
2020 Date Event Name (link to URL) 2020 State 2020 City January 3, 2020 Society of American Law Teachers (SALT) Annual Awards Celebration DC Washington January 15 – 19, 2020 Creating Change Conference TX Dallas February 7-9, 2020 People’s Parity Project National Convening DC Washington February 8 – 9, 2020 Democracy Matters Student Summit NY Albany February 8 – 12, 2020 American Association for Justice Winter Convention LA New Orleans February 14 – 15, 2020 Rebellious Lawyering Conference CT New Haven February 21, 2020 2019 New Hampshire Bar Association Midyear Meeting NH Manchester February 22 – 25, 2020 National Association of Minority & Women Owned Firms Driving Diversity and FL Fort Lauderdale Leadership Conference February 28 –29, 2020 GRITS (Getting Radical in the South) Conference TX Austin March 3 – 8, 2020 National Black Law Student Association (NLBSA)'s Annual National Convention OH Cincinnati March 12, 2020 Legal Momentum Women of Achievement Awards Dinner CA San Francisco March 13, 2020 Ms. JD Annual Conference on Women in Law IL Chicago March 18 – 20, 2020 The Leadership Institute for Women of Color Attorneys Leadership Conference GA Atlanta March 21, 2020 ACS Board of Academic Advisors Conference CT New Haven March 26 – 27, 2020 Vermont Bar Association Mid-Year Meeting VT Burlington March 27 – 28, 2020 2020 ACS National Student Convention MA Cambridge March 31 – April 2, 2020 Global Youth Justice Training NV Las Vegas April 5 – 6, 2020 West Virginia State Bar Annual Meeting WV White Sulphur Springs April 6 – 7, 2020 Federal -

About the Foundation
STUART R. BUTZIER President SCOT W. ANDERSON Vice President Excellence in Natural Resources Law NEIL G. WESTESEN Secretary SANDRA A. SNODGRASS Advancing understanding of the laws and issues affecting the Treasurer development of mineral, energy, and water resources since 1955. ALEX RITCHIE Executive Director CONSTITUENT ORGANIZATIONS The Rocky Mountain Mineral Law Foundation is a collaborative, educational, non-profit Law Schools organization dedicated to the scholarly and practical study of the laws and regulations University of Alberta University of Arizona relating to oil and gas, mining, energy, public lands, water, environmental protection, and Arizona State University Brigham Young University international law. Through our educational programs, we bring together lawyers, landmen, University of Calgary University of California-Davis managers, consultants, government personnel, law faculty, students, and others involved in University of Colorado Creighton University University of Denver the practice, application, and study of these areas of law. Florida State University Gonzaga University University of Houston University of Idaho Our programs include University of Kansas Lewis and Clark Law School Louisiana State University • University of Minnesota Institutes, short courses, workshops, webinars, and other virtual programs (domestic University of Montana University of Nebraska and international) focusing on relevant legal developments and issues University of Nevada–Las Vegas • University of New Mexico Online natural resources educational -

Nonlawyer Practice Within Law Firms
Shadow Lawyering: Nonlawyer Practice Within Law Firms PAUL R. TREMBLAY INTRODUCTION....................................................................................................... 654 I. A LAW FIRM STORY ............................................................................................ 661 II. ADVISORY GUIDANCE AND SUBSTANTIVE LAW REGULATING NONLAWYER PRACTICE ............................................................................................................... 663 A. ADVISORY RHETORIC ............................................................................... 663 B. AUTHORITY FROM STATE RULES OR STATUTES ....................................... 666 C. AUTHORITY FROM THE COMMON LAW ..................................................... 668 D. INSIGHTS FROM THE ATTORNEY-CLIENT PRIVILEGE CASES ...................... 671 III. A CONCEPTUAL FRAMEWORK FOR UNDERSTANDING DELEGATION TO NONLAWYERS ........................................................................................................ 673 A. INTRODUCTION AND OVERVIEW ............................................................... 673 B. RISK ASSESSMENT, INFORMED CONSENT, AND UNAUTHORIZED-PRACTICE RATIONALES ................................................................................................. 674 C. THE NONLAWYER DELEGATION FRAMEWORK AS AN ALCHEMY OF RISK MANAGEMENT, INFORMED CONSENT, AND UNAUTHORIZED-PRACTICE PROPHYLAXIS ............................................................................................... 678 IV. APPLYING THE CONCEPTUAL -

Succession Planning Handbook for New Mexico Lawyers
Succession Planning Handbook For New Mexico Lawyers Protecting Your Clients’ Interests By Providing for a Smooth Transition After Your Retirement, Death or Disability July 2014 New Mexico Supreme Court Lawyer Succession and Transition Committee State Bar of New Mexico Lawyers and Judges Assistance Program, Client Protection Fund, Senior Lawyers Division New Mexico Supreme Court Lawyer Succession and Transition Committee Justice Edward L Chávez Charles D. Noland Briggs F. Cheney William D. Slease, Chair Joseph R. Conte Richard B. Spinello Sandra Morgan Little Jill Anne Yeagley Gaelle D. McConnell Caution Regarding Sample Forms This handbook is a guide to help New Mexico lawyers protect their clients when a law practice is interrupted. The forms provided are samples only and anyone using these forms must adapt them to fit his or her individual circumstances. Further, the sample forms and the recommendations made in this handbook are not intended to excuse users’ compliance with all laws, statutes and applicable court rules, including but not limited to the Rules of Professional Conduct. If any provisions of this handbook or any terms of the sample forms conflict with New Mexico statutes, court rules or case law, the applicable legal authority shall control. Users must confirm that any forms used comply with all applicable laws and rules. Acknowledgments The Lawyer Succession and Transition Committee was established as an official Supreme Court committee effective Jan. 1, 2013. Research soon showed that the succession planning guide published by the Oregon State Bar Professional Liability Fund in 1999 was the seminal resource for several other states. The New Mexico committee gratefully acknowledges Oregon’s pioneering work in this area and its generosity in sharing its guide. -

Sue Unto Others Outline and Handouts
SUE UNTO OTHERS AS YOU WOULD HAVE THEM SUE UNTO YOU A One-Hour Webinar Covering: Professionalism Presented by: Sean Carter CA Bar# 200356 OVERVIEW Increasingly, lawyer civility and congeniality is becoming a thing of the past. Yet, it doesn’t have to be that way. In this presentation, veteran attorney and legal humorist Sean Carter will remind lawyers that zealous advocacy does not require them to be zealots. In particular, Mr. Carter will discuss practical ways to: • Reduce the hostility in interactions with even the most difficult opposing counsel; • Increase camaraderie among colleagues; • Diffuse tensions between warring clients; • Secure accommodations from opposing counsel; • Structure more mutually beneficial arrangements with clients; • Maintain proper decorum before the court; • Assist in providing pro bono legal services; • Serve the bar and the legal profession; and • Provide service to the community at large. TIMED AGENDA (60 minutes) 0:00-0:05 General Overview of State Professionalism Creeds 1. Genesis of the creeds 2. Aspiration nature Six Suggestions for Professional Behavior 0:05-0:15 Suggestion #1: Show Some Respect 1. Avoid undue familiarity with members of the judiciary 2. Avoid unfounded, unsubstantiated, or unjustified public criticism of members of the judiciary 3. Show respect by attire and demeanor 0:15-0:25 Suggestion #2: Behave Yourself 1. Consider the effect of our individual conduct on the image of the law and the profession 2. Work to improve the law 3. Defend profession against unjust criticism 4. Respect and honor the traditions of the profession and those lawyers who best uphold those traditions 0:25-0:30 Suggestion #3: Don’t Run Up the Bill 1. -
• Time to Submit Award Nominations • New
Volume 79 u No. 13 u May 10, 2008 ALSO INSIDE • Time to Submit Award Nominations • New Lawyers Admitted GROW YOUR 401(k) WISELY OBA/CLE Presents Building Your Million Dollar Practice And Six things you won’t hear Law Practice Phase Two: Building a Plan for the Next Era of Your from other 401(k) providers... Career May 29 & 30 We were created as a not-for-profit Oklahoma Bar Center, Oklahoma City 1. entity, and we exist to provide a benefit Building Your Million Dollar Practice Dustin Cole Are you ready to – President We leverage the buying power of the Double your revenues over the next five years? Attorneys Master Class 2. ABA to eliminate firm expenses and Transform your practice into a highly efficient, client-focused minimize participant expenses legal business? Speaker Dustin Cole is a Master Reduce stress and hours in the office? Practice Advisor, and is President of Lay the operational and financial groundwork for your dream Attorneys Master Class, one of the Our fiduciary tools help you manage retirement? nation’s leading attorney practice your liabilities and save valuable time – Then don’t miss this program! development organizations. Mr. Cole 3. Part One: Building the Million-Dollar Operations has trained over ten thousand Cole provides a truly unique view of how practices grow and evolve, attorneys across the United States in how to build more successful Our investment menu has three tiers to from the sole practice to the attorney with efficient, profitable legal practices and develop their dream 4. provide options for any type of investor, teams serving client needs, and provides step-by-step advice on how to retirements. -

Aliquot Portion of Their Dues: a Survey of Unified Bar Compliance
"AN ALIQUOT PORTION OF THEIR DUES: " A SURVEY OF UNIFIED BAR COMPLIANCE WITH HUDSON AND KELLER By Ralph H.Brock" I. INTRODUCTION ......................................... 24 II. THE LABOR UNION-UNIFIED BAR ANALOGY ................. 27 A. Prologue.: "only the duty to pay dues."................... 28 B. The Use of Mandatory Duesfor Politicalor Ideological A ctivities .......................................... 36 C. Chargeableand NonchargeableActivities ............... 40 1. ChargeableActivities ............................ 41 2. Nonchargeable Activities .......................... 43 D. Epilogue: The DissentingMembers' Remedies ............ 45 III. HUDSON/KELLER PROCEDURES AMONG THE UNIFIED BAR A SSOCIATIONS ......................................... 47 A. Post-KellerLitigation ............................... 48 1. The Puerto Rican Litigation ...................... 48 2. The Wisconsin Litigation ......................... 48 3. The FloridaLitigation ........................... 50 4. The New Mexico Litigation ....................... 50 B. Common Misinterpretationsof Hudson and Keller ......... 51 IV. STATE-BY-STATE SURVEY .................. ............. 53 A. The Alabama State Bar .............................. 53 B. The Alaska Bar Association ........................... 53 C. The State Bar ofArizona ............................. 55 D. The State Bar of California ........................... 56 E. The District of Columbia Bar ........................ 57 F. The FloridaBar .................................... 58 G. The State Bar of Georgia ............................ -

Report of Committee on Rules of Practice Before State Boards
Wyoming Law Journal Volume 4 Number 1 Article 11 December 2019 Report of Committee on Rules of Practice before State Boards Wyoming State Bar Follow this and additional works at: https://scholarship.law.uwyo.edu/wlj Recommended Citation Wyoming State Bar, Report of Committee on Rules of Practice before State Boards, 4 WYO. L.J. 57 (1949) Available at: https://scholarship.law.uwyo.edu/wlj/vol4/iss1/11 This Special Section is brought to you for free and open access by Law Archive of Wyoming Scholarship. It has been accepted for inclusion in Wyoming Law Journal by an authorized editor of Law Archive of Wyoming Scholarship. MINUTES OF ANNUAL MEETING OF WYOMING STATE BAR 57 VIII. JURISDICTION Notbing herein contained shall be construed to create any financial liability upon any signatory hereto or to authorize the Council to make any committment of any kind or to declare any policy or position on any question on behalf of any signatory. IX. ADOPTION These Articles shall become effective upon the signing hereof by the duly authorized officers of the state bar organizations constituting the said Council. The within Articles of Association of Interstate Bar Council are sub- scribed to by officers of the undersigned professional groups first thereunto duly authorized on the date set opposite each. STATE BAR OF ARIZONA By: THE COLORADO STATE BAR By: IDAHO STATE BAR By: MONTANA BAR ASSOCIATION By: STATE BAR OF NEVADA By: STATE BAR OF NEW MEXICO By: OREGON STATE BAR By: WASHINGTON STATE BAR ASSOC. By: WYOMING STATE BAR By: UTAH STATE BAR By: THE STATE BAR OF CALIFORNIA By: REPORT OF COMMITTEE ON RULES OF PRACTICE BEFORE STATE BOARDS On September 3rd, 1948, the following members were appointed as a Com- mittee to make a study of the problem of Rules of Practice before the State Boards of the State of Wyoming: George F.