Report Evidence That Griscelli Syndrome with Neurological
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Exophilin-5 Regulates Allergic Airway Inflammation by Controlling IL-33–Mediated Th2 Responses
The Journal of Clinical Investigation RESEARCH ARTICLE Exophilin-5 regulates allergic airway inflammation by controlling IL-33–mediated Th2 responses Katsuhide Okunishi,1 Hao Wang,1 Maho Suzukawa,2,3 Ray Ishizaki,1 Eri Kobayashi,1 Miho Kihara,4 Takaya Abe,4,5 Jun-ichi Miyazaki,6 Masafumi Horie,7 Akira Saito,7 Hirohisa Saito,8 Susumu Nakae,9 and Tetsuro Izumi1 1Laboratory of Molecular Endocrinology and Metabolism, Department of Molecular Medicine, Institute for Molecular and Cellular Regulation, Gunma University, Maebashi, Japan. 2National Hospital Organization Tokyo National Hospital, Tokyo, Japan. 3Division of Respiratory Medicine and Allergology, Department of Medicine, Teikyo University School of Medicine, Tokyo, Japan. 4Laboratory for Animal Resource Development and 5Genetic Engineering, RIKEN Center for Biosystems Dynamics Research, Kobe, Japan. 6Institute of Scientific and Industrial Research, Osaka University, Osaka, Japan. 7Department of Respiratory Medicine, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan. 8Department of Allergy and Clinical Immunology, National Research Institute for Child Health and Development, Tokyo, Japan. 9Laboratory of Systems Biology, Center for Experimental Medicine and Systems Biology, Institute of Medical Science, The University of Tokyo, Tokyo, Japan. A common variant in the RAB27A gene in adults was recently found to be associated with the fractional exhaled nitric oxide level, a marker of eosinophilic airway inflammation. The small GTPase Rab27 is known to regulate intracellular vesicle traffic, although its role in allergic responses is unclear. We demonstrated that exophilin-5, a Rab27-binding protein, was predominantly expressed in both of the major IL-33 producers, lung epithelial cells, and the specialized IL-5 and IL-13 producers in the CD44hiCD62LloCXCR3lo pathogenic Th2 cell population in mice. -

Supplementary Table S4. FGA Co-Expressed Gene List in LUAD
Supplementary Table S4. FGA co-expressed gene list in LUAD tumors Symbol R Locus Description FGG 0.919 4q28 fibrinogen gamma chain FGL1 0.635 8p22 fibrinogen-like 1 SLC7A2 0.536 8p22 solute carrier family 7 (cationic amino acid transporter, y+ system), member 2 DUSP4 0.521 8p12-p11 dual specificity phosphatase 4 HAL 0.51 12q22-q24.1histidine ammonia-lyase PDE4D 0.499 5q12 phosphodiesterase 4D, cAMP-specific FURIN 0.497 15q26.1 furin (paired basic amino acid cleaving enzyme) CPS1 0.49 2q35 carbamoyl-phosphate synthase 1, mitochondrial TESC 0.478 12q24.22 tescalcin INHA 0.465 2q35 inhibin, alpha S100P 0.461 4p16 S100 calcium binding protein P VPS37A 0.447 8p22 vacuolar protein sorting 37 homolog A (S. cerevisiae) SLC16A14 0.447 2q36.3 solute carrier family 16, member 14 PPARGC1A 0.443 4p15.1 peroxisome proliferator-activated receptor gamma, coactivator 1 alpha SIK1 0.435 21q22.3 salt-inducible kinase 1 IRS2 0.434 13q34 insulin receptor substrate 2 RND1 0.433 12q12 Rho family GTPase 1 HGD 0.433 3q13.33 homogentisate 1,2-dioxygenase PTP4A1 0.432 6q12 protein tyrosine phosphatase type IVA, member 1 C8orf4 0.428 8p11.2 chromosome 8 open reading frame 4 DDC 0.427 7p12.2 dopa decarboxylase (aromatic L-amino acid decarboxylase) TACC2 0.427 10q26 transforming, acidic coiled-coil containing protein 2 MUC13 0.422 3q21.2 mucin 13, cell surface associated C5 0.412 9q33-q34 complement component 5 NR4A2 0.412 2q22-q23 nuclear receptor subfamily 4, group A, member 2 EYS 0.411 6q12 eyes shut homolog (Drosophila) GPX2 0.406 14q24.1 glutathione peroxidase -

Rab27a and Rab27b Control Different Steps of the Exosome Secretion Pathway
ARTICLES Rab27a and Rab27b control different steps of the exosome secretion pathway Matias Ostrowski1,2, Nuno B. Carmo3,12, Sophie Krumeich1,2,12, Isabelle Fanget10,12, Graça Raposo4,2, Ariel Savina1,2, Catarina F. Moita3, Kristine Schauer4,2, Alistair N. Hume5, Rui P. Freitas3, Bruno Goud4,2, Philippe Benaroch1,2, Nir Hacohen8,9, Mitsunori Fukuda11, Claire Desnos10, Miguel C. Seabra5,6,7, François Darchen10, Sebastian Amigorena1,2, Luis F. Moita3,13 and Clotilde Thery1,2,13 Exosomes are secreted membrane vesicles that share structural and biochemical characteristics with intraluminal vesicles of multivesicular endosomes (MVEs). Exosomes could be involved in intercellular communication and in the pathogenesis of infectious and degenerative diseases. The molecular mechanisms of exosome biogenesis and secretion are, however, poorly understood. Using an RNA interference (RNAi) screen, we identified five Rab GTPases that promote exosome secretion in HeLa cells. Among these, Rab27a and Rab27b were found to function in MVE docking at the plasma membrane. The size of MVEs was strongly increased by Rab27a silencing, whereas MVEs were redistributed towards the perinuclear region upon Rab27b silencing. Thus, the two Rab27 isoforms have different roles in the exosomal pathway. In addition, silencing two known Rab27 effectors, Slp4 (also known as SYTL4, synaptotagmin-like 4) and Slac2b (also known as EXPH5, exophilin 5), inhibited exosome secretion and phenocopied silencing of Rab27a and Rab27b, respectively. Our results therefore strengthen the link between MVEs and exosomes, and introduce ways of manipulating exosome secretion in vivo. Exosomes are membrane vesicles secreted into the extracellular space membrane of MVEs into the lumen of these endosomes14. -
The Genetics of Intellectual Disability: Whole Exome Sequencing to Find Causative Variants in Severe Cases
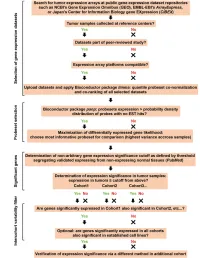
Master’s Project in Medicine No 4362 The Genetics of Intellectual Disability: whole exome sequencing to find causative variants in severe cases Student Winteler Florence Supervisor Prof. Reymond Alexandre, Ph.D. Center for Integrative Genomics, UNIL Co-Supervisor Gueneau Lucie, Ph.D. Center for Integrative Genomics, UNIL Expert Prof. Draganski Bogdan, Dr. méd Département des neurosciences cliniques, CHUV Lausanne, 25.11.2017 Abstract Intellectual disability (ID) affects 1-3% of the population. A genetic origin is estimated to account for about half of the currently undiagnosed cases, and despite recent successes in identifying some of the genes, it has been suggested that hundreds more genes remain to be identified. ID can be isolated or part of a more complex clinical picture –indeed other symptoms are often found in patients with severe genetic ID, such as developmental delay, organ malformations or seizures. In this project, we used whole exome sequencing (WES) to analyse the coding regions of the genes (exons) of patients with undiagnosed ID and that of their families. The variants called by our algorithm were then grossly sorted out using criteria such as frequency in the general population and predicted pathogenicity. A second round of selection was made by looking at the relevant literature about the function of the underlying genes and pathways involved. The selected variants were then Sanger-sequenced for confirmation. This strategy allowed us to find the causative variant and give a diagnosis to the first family we analysed, as the patient was carrying a mutation in the Methyl-CpG binding protein 2 gene (MECP2), already known to cause Rett syndrome. -

RAB27A Promotes Melanoma Cell Invasion and Metastasis Via Regulation of Pro
RAB27A promotes melanoma cell invasion and metastasis via regulation of pro- invasive exosomes Dajiang Guo1,2*, Goldie Y. L. Lui1,2*, Siew Li Lai1, James S. Wilmott2,3, Shweta Tikoo1,2, Louise A. Jackett2,3,4, Camelia Quek3, Darren L. Brown5, Danae M. Sharp1,2, Rain Y.Q. Kwan1,2, Diego Chacon6,7, Jason H. Wong7,8, Dominik Beck6,7, Michelle van Geldermalsen1,2, Jeff Holst1,2, John F. Thompson2,3,4, Graham J. Mann3,9, Richard A. Scolyer2,3,4, Jennifer L. Stow5, Wolfgang Weninger1,10,11#, Nikolas K. Haass1,10,12#, Kimberley A. Beaumont1,2# 1The Centenary Institute, The University of Sydney, Newtown, NSW, Australia; Article 2Sydney Medical School, The University of Sydney, Camperdown, NSW, Australia; 3Melanoma Institute Australia, The University of Sydney, North Sydney, NSW, Australia; 4Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 5The Institute for Molecular Bioscience, The University of Queensland, Brisbane, QLD, Australia; 6Centre for Health Technologies and the School of Biomedical Engineering, University of Technology, Sydney, NSW, Australia; 7Adult Cancer Program, Lowy Cancer Research Centre, Prince of Wales Clinical School, University of New South Wales, Sydney, NSW, Australia; 8School of Biomedical Sciences, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pok Fu Lam, Hong Kong; 9Centre for Cancer Research, Westmead Institute for Medical Research, The University of Sydney, Westmead, NSW, Australia; 10Discipline of Dermatology, The Accepted University of Sydney, Camperdown, NSW, Australia; 11Department of Dermatology, Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 12The University of This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. -

Blueprint Genetics Comprehensive Immune and Cytopenia Panel
Comprehensive Immune and Cytopenia Panel Test code: IM0901 Is a 642 gene panel that includes assessment of non-coding variants. Is ideal for patients with a clinical suspicion of an inborn error of immunity, such as, Primary Immunodeficiency, Bone Marrow Failure Syndrome, Dyskeratosis Congenita, Neutropenia, Thrombocytopenia, Hemophagocytic Lymphohistiocytosis, Autoinflammatory Disorders, Complement System Disorder, Leukemia, or Chronic Granulomatous Disease. This panel includes most genes from Primary Immunodeficiency, Severe Combined Immunodeficiency, Complement System Disorder, Bone Marrow Failure Syndrome, Hemophagocytic Lymphohistiocytosis, Congenital Neutropenia, Thrombocytopenia, Congenital Diarrhea, Chronic Granulomatous Disease, Diamond-Blackfan Anemia, Fanconi Anemia, Dyskeratosis Congenita, Autoinflammatory Syndrome, and Hereditary Leukemia Panels as well as many other genes associated with inborn errors of immunity. Please note that unlike our other panels, this panel is on our Whole Exome Sequencing platform and cannot be customized. Pricing may vary from our regular panel pricing. About immunodeficiency and cytopenia disorders There is an enormous amount of phenotypic overlap between immunological and hematological disorders, which makes it challenging to know which of these two systems is not functioning properly. Knowing the underlying genetic cause of a person’s clinical diagnosis, especially immunodeficiency, bone marrow failure, neutropenia, thrombocytopenia, autoinflammatory disease, or bone marrow failure can sometime -

Download CGT Exome V2.0
CGT Exome version 2. -

Essential Role of Microphthalmia Transcription Factor for DNA Replication, Mitosis and Genomic Stability in Melanoma
Oncogene (2011) 30, 2319–2332 & 2011 Macmillan Publishers Limited All rights reserved 0950-9232/11 www.nature.com/onc ORIGINAL ARTICLE Essential role of microphthalmia transcription factor for DNA replication, mitosis and genomic stability in melanoma T Strub1,4, S Giuliano2,4,TYe1, C Bonet2, C Keime1, D Kobi1, S Le Gras1, M Cormont3, R Ballotti2, C Bertolotto2 and I Davidson1 1Institut de Ge´ne´tique et de Biologie Mole´culaire et Cellulaire, CNRS, INSERM, Universite´ de Strasbourg, Illkirch, France; 2INSERM U895 Team 1 and Department of Dermatology, CHU Nice, France and 3INSERM U895 Team 7, Nice, France Malignant melanoma is an aggressive cancer known use of internal promoters (Steingrimsson, 2008). The for its notorious resistance to most current therapies. MITF-M isoform (hereafter designated simply as The basic helix-loop-helix microphthalmia transcription MITF) is the major form produced specifically in the factor (MITF) is the master regulator determining the melanocyte lineage from an intronic promoter (Goding, identity and properties of the melanocyte lineage, and is 2000b). MITF is essential for the survival of melano- regarded as a lineage-specific ‘oncogene’ that has a blasts and postnatal melanocytes (McGill et al., 2002; critical role in the pathogenesis of melanoma. MITF Hou and Pavan, 2008), in which it also controls the promotes melanoma cell proliferation, whereas sustained expression of genes required for the melanin synthesis supression of MITF expression leads to senescence. (Bertolotto et al., 1998). By combining chromatin immunoprecipitation coupled to In addition to regulating multiple aspects of normal high throughput sequencing (ChIP-seq) and RNA sequen- melanocyte function, MITF also has a critical role in cing analyses, we show that MITF directly regulates a melanoma, in which it is required for survival, and set of genes required for DNA replication, repair and controls the proliferation, invasive and metastatic mitosis. -

Supplemental Figures 04 12 2017
Jung et al. 1 SUPPLEMENTAL FIGURES 2 3 Supplemental Figure 1. Clinical relevance of natural product methyltransferases (NPMTs) in brain disorders. (A) 4 Table summarizing characteristics of 11 NPMTs using data derived from the TCGA GBM and Rembrandt datasets for 5 relative expression levels and survival. In addition, published studies of the 11 NPMTs are summarized. (B) The 1 Jung et al. 6 expression levels of 10 NPMTs in glioblastoma versus non‐tumor brain are displayed in a heatmap, ranked by 7 significance and expression levels. *, p<0.05; **, p<0.01; ***, p<0.001. 8 2 Jung et al. 9 10 Supplemental Figure 2. Anatomical distribution of methyltransferase and metabolic signatures within 11 glioblastomas. The Ivy GAP dataset was downloaded and interrogated by histological structure for NNMT, NAMPT, 12 DNMT mRNA expression and selected gene expression signatures. The results are displayed on a heatmap. The 13 sample size of each histological region as indicated on the figure. 14 3 Jung et al. 15 16 Supplemental Figure 3. Altered expression of nicotinamide and nicotinate metabolism‐related enzymes in 17 glioblastoma. (A) Heatmap (fold change of expression) of whole 25 enzymes in the KEGG nicotinate and 18 nicotinamide metabolism gene set were analyzed in indicated glioblastoma expression datasets with Oncomine. 4 Jung et al. 19 Color bar intensity indicates percentile of fold change in glioblastoma relative to normal brain. (B) Nicotinamide and 20 nicotinate and methionine salvage pathways are displayed with the relative expression levels in glioblastoma 21 specimens in the TCGA GBM dataset indicated. 22 5 Jung et al. 23 24 Supplementary Figure 4. -
Supplementary Data
SUPPLEMENTAL INFORMATION A study restricted to chemokine receptors as well as a genome-wide transcript analysis uncovered CXCR4 as preferentially expressed in Ewing's sarcoma (Ewing's sarcoma) cells of metastatic origin (Figure 4). Transcriptome analyses showed that in addition to CXCR4, genes known to support cell motility and invasion topped the list of genes preferentially expressed in metastasis-derived cells (Figure 4D). These included kynurenine 3-monooxygenase (KMO), galectin-1 (LGALS1), gastrin-releasing peptide (GRP), procollagen C-endopeptidase enhancer (PCOLCE), and ephrin receptor B (EPHB3). KMO, a key enzyme of tryptophan catabolism, has not been linked to metastasis. Tryptophan and its catabolites, however, are involved in immune evasion by tumors, a process that can assist in tumor progression and metastasis (1). LGALS1, GRP, PCOLCE and EPHB3 have been linked to tumor progression and metastasis of several cancers (2-4). Top genes preferentially expressed in L-EDCL included genes that suppress cell motility and/or potentiate cell adhesion such as plakophilin 1 (PKP1), neuropeptide Y (NPY), or the metastasis suppressor TXNIP (5-7) (Figure 4D). Overall, L-EDCL were enriched in gene sets geared at optimizing nutrient transport and usage (Figure 4D; Supplementary Table 3), a state that may support the early stages of tumor growth. Once tumor growth outpaces nutrient and oxygen supplies, gene expression programs are usually switched to hypoxic response and neoangiogenesis, which ultimately lead to tumor egress and metastasis. Accordingly, gene sets involved in extracellular matrix remodeling, MAPK signaling, and response to hypoxia were up-regulated in M-EDCL (Figure 4D; Supplementary Table 4), consistent with their association to metastasis in other cancers (8, 9). -

Investigating Developmental and Epileptic Encephalopathy Using Drosophila Melanogaster
International Journal of Molecular Sciences Review Investigating Developmental and Epileptic Encephalopathy Using Drosophila melanogaster Akari Takai 1 , Masamitsu Yamaguchi 2,3, Hideki Yoshida 2 and Tomohiro Chiyonobu 1,* 1 Department of Pediatrics, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto 602-8566, Japan; [email protected] 2 Department of Applied Biology, Kyoto Institute of Technology, Matsugasaki, Sakyo-ku, Kyoto 603-8585, Japan; [email protected] (M.Y.); [email protected] (H.Y.) 3 Kansai Gakken Laboratory, Kankyo Eisei Yakuhin Co. Ltd., Kyoto 619-0237, Japan * Correspondence: [email protected] Received: 15 August 2020; Accepted: 1 September 2020; Published: 3 September 2020 Abstract: Developmental and epileptic encephalopathies (DEEs) are the spectrum of severe epilepsies characterized by early-onset, refractory seizures occurring in the context of developmental regression or plateauing. Early infantile epileptic encephalopathy (EIEE) is one of the earliest forms of DEE, manifesting as frequent epileptic spasms and characteristic electroencephalogram findings in early infancy. In recent years, next-generation sequencing approaches have identified a number of monogenic determinants underlying DEE. In the case of EIEE, 85 genes have been registered in Online Mendelian Inheritance in Man as causative genes. Model organisms are indispensable tools for understanding the in vivo roles of the newly identified causative genes. In this review, we first present an overview of epilepsy and its genetic etiology, especially focusing on EIEE and then briefly summarize epilepsy research using animal and patient-derived induced pluripotent stem cell (iPSC) models. The Drosophila model, which is characterized by easy gene manipulation, a short generation time, low cost and fewer ethical restrictions when designing experiments, is optimal for understanding the genetics of DEE. -

A Mutation in Rab27a Causes the Vesicle Transport Defects Observed in Ashen Mice
A mutation in Rab27a causes the vesicle transport defects observed in ashen mice Scott M. Wilson*, Richard Yip*, Deborah A. Swing*, T. Norene O’Sullivan*, Yuke Zhang†, Edward K. Novak†, Richard T. Swank†, Liane B. Russell‡, Neal G. Copeland*, and Nancy A. Jenkins*§ *Mouse Cancer Genetics Program, National Cancer Institute–Frederick Cancer Research and Development Center, Frederick, MD 21702; †Department of Molecular and Cell Biology, Roswell Park Cancer Institute, Buffalo, NY 14263; and ‡Biology Division, Oak Ridge National Laboratory, Oak Ridge, TN 37831 Contributed by Liane B. Russell, May 11, 2000 The dilute (d), leaden (ln), and ashen (ash) mutations provide a cells (9, 10). The absence of SER in spines probably disrupts unique model system for studying vesicle transport in mammals. the regulation of intracellular Ca2ϩ and postsynaptic signal All three mutations produce a lightened coat color because of transduction. defects in pigment granule transport. In addition, all three muta- A retroviral integration into the d gene in mice carrying the tions are suppressed by the semidominant dilute-suppressor (dsu), dilute-viral (dv) allele allowed the cloning of the d gene and the providing genetic evidence that these mutations function in the demonstration that d encodes an unconventional myosin heavy- same or overlapping transport pathways. Previous studies showed chain, myosin Va (MyoVa) (11, 12). MyoVa is expressed at high that d encodes a major vesicle transport motor, myosin-VA, which levels in nearly all tissues in the adult (12) and has the expected is mutated in Griscelli syndrome patients. Here, using positional structure for a member of this family—i.e., a globular head cloning and bacterial artificial chromosome rescue, we show that domain containing the ATP- and actin-binding sites, a ‘‘neck’’ ash encodes Rab27a.