Assessment of Health Sub-Centers in Jhansi District In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
District Census Statistics, N. W. Provinces and Oudh, Jhansi, India
~hltfitt ~.enJns ~tatistits, N.-W. P,ROVINCES AND OUDH. ,JHANSI DISTRICT.. ALT.ABABAD : weaar-WJI8'tB.B.N noTUtQaa AllD 017DB QOVUNJDIIB'l' Pl\1mS. 1896. TABLE UF CONTE~TS. Serial Jlum Contents. Page. bet. 1 Preface statement .howing the variations of population in the pal'ganas and tllohails of th Jhansi 6 uistrict. 8 Stalement sllowing the variations in the population of the Police circle Jbtinsi district 6 4 Statement showing by population the number of towns and viIlnges in the Ta.bsils of tbe 7 JMnsi district. Village DU'octory, tahsil GarothAJ pa.rgana. Garotha , 10-16 6 Ditto ditto .Tb{inlli, ditto 113-25 7 Di~to ditto Moth , ditto Motb 8 Ditto ditto Mau; ditto Mau 27-83 9 Ditto ditte> Mehroni, ditto Bau1?ur 38-37 10 Ditto ditto ditto ditto Marau.ra 11 Ditto ditto ditto ditto Mehroni 12 Ditto ditto dittQ ditto Bansi 13 Ditto ditto LaJitpUf, ditto Lautpur 406-61 Ditto ditto ditto ditto Dalabehat 51-58 15 Ditto ditto ditto ditto Talhebat 53-66 16 Statement showing the figures of the Village Directory totalled for each of the thanu of tbe Jhilusi district. _ 17 Alphabetical ind x to the villages a.nd towns of the JhlInai distriot 63-67 PREFACE Tll.E census ta.bles published for the North-Western Pl'OvinMs snd Oudh, tmder the orders of the imperial government, coJl'tain no detailed statistic £01' any aren. smaller thun the district. The local government has cODsidered.- it necessary to publish in addition to these impel'ial ta.bll."s- lit-A provjncia,l suppJement to the report on tbe census of 189], oonlia:iniog certain impor~ ant statistics for tahsil, pal'gaollo, tht'na (lnd town DTOOS. -

Section-VIII : Laboratory Services
Section‐VIII Laboratory Services 8. Laboratory Services 8.1 Haemoglobin Test ‐ State level As can be seen from the graph, hemoglobin test is being carried out at almost every FRU studied However, 10 percent medical colleges do not provide the basic Hb test. Division wise‐ As the graph shows, 96 percent of the FRUs on an average are offering this service, with as many as 13 divisions having 100 percent FRUs contacted providing basic Hb test. Hemoglobin test is not available at District Women Hospital (Mau), District Women Hospital (Budaun), CHC Partawal (Maharajganj), CHC Kasia (Kushinagar), CHC Ghatampur (Kanpur Nagar) and CHC Dewa (Barabanki). 132 8.2 CBC Test ‐ State level Complete Blood Count (CBC) test is being offered at very few FRUs. While none of the sub‐divisional hospitals are having this facility, only 25 percent of the BMCs, 42 percent of the CHCs and less than half of the DWHs contacted are offering this facility. Division wise‐ As per the graph above, only 46 percent of the 206 FRUs studied across the state are offering CBC (Complete Blood Count) test service. None of the FRUs in Jhansi division is having this service. While 29 percent of the health facilities in Moradabad division are offering this service, most others are only a shade better. Mirzapur (83%) followed by Gorakhpur (73%) are having maximum FRUs with this facility. CBC test is not available at Veerangna Jhalkaribai Mahila Hosp Lucknow (Lucknow), Sub Divisional Hospital Sikandrabad, Bullandshahar, M.K.R. HOSPITAL (Kanpur Nagar), LBS Combined Hosp (Varanasi), -

Brief Industrial Profile of Lalitpur District
lR;eso t;rs Government of India Ministry of MSME Brief Industrial Profile of Lalitpur District MSME -Development Institute (Ministry of MSME, Govt. of India,) Phone: 0512-2295070-73 Fax: 0512-2240143 E-mail: [email protected] Web- msmedikanpur.gov.in Compiled by – Kashi Prasad Sheel Investigator (L/F) 1 FOREWORD District Industrial Potentiality Survey Report of District Lalitpur is a key report which not only contains current industrial scenario of the district but also other useful information about the district. This report provides valuable inputs which may be useful for existing & prospective entrepreneurs of the District. It is the only source which provides the latest data on infrastructure, banking and industry of the district. It also provides information on potentials areas in manufacturing and service sector of the district. I sincerely hope that District Industrial Potentiality Survey Report of District Lalitpur will facilitate easier dissemination of information about the district to policy makers and also to the professionals working in the MSME sector. I appreciate the efforts made by Shri Jagadish Sahu, Asstt. Director (EI) in preparing the District Industrial Potentiality Survey Report of Lalitpur District. June, 2016 ( U. C. Shukla ) Kanpur Director 2 Contents S. No. Topic Page No. 1. General Characteristics of the District 03-04 1.1 Location & Geographical Area 04-05 1.2 Topography 05-06 1.3 Availability of Minerals. 06-07 1.4 Forest 07 1.5 Administrative set up 07 2. District at a glance 08-10 2.1 Existing Status of Industrial Area in the District Lalitpur 10 3. -

List of Class Wise Ulbs of Uttar Pradesh
List of Class wise ULBs of Uttar Pradesh Classification Nos. Name of Town I Class 50 Moradabad, Meerut, Ghazia bad, Aligarh, Agra, Bareilly , Lucknow , Kanpur , Jhansi, Allahabad , (100,000 & above Population) Gorakhpur & Varanasi (all Nagar Nigam) Saharanpur, Muzaffarnagar, Sambhal, Chandausi, Rampur, Amroha, Hapur, Modinagar, Loni, Bulandshahr , Hathras, Mathura, Firozabad, Etah, Badaun, Pilibhit, Shahjahanpur, Lakhimpur, Sitapur, Hardoi , Unnao, Raebareli, Farrukkhabad, Etawah, Orai, Lalitpur, Banda, Fatehpur, Faizabad, Sultanpur, Bahraich, Gonda, Basti , Deoria, Maunath Bhanjan, Ballia, Jaunpur & Mirzapur (all Nagar Palika Parishad) II Class 56 Deoband, Gangoh, Shamli, Kairana, Khatauli, Kiratpur, Chandpur, Najibabad, Bijnor, Nagina, Sherkot, (50,000 - 99,999 Population) Hasanpur, Mawana, Baraut, Muradnagar, Pilkhuwa, Dadri, Sikandrabad, Jahangirabad, Khurja, Vrindavan, Sikohabad,Tundla, Kasganj, Mainpuri, Sahaswan, Ujhani, Beheri, Faridpur, Bisalpur, Tilhar, Gola Gokarannath, Laharpur, Shahabad, Gangaghat, Kannauj, Chhibramau, Auraiya, Konch, Jalaun, Mauranipur, Rath, Mahoba, Pratapgarh, Nawabganj, Tanda, Nanpara, Balrampur, Mubarakpur, Azamgarh, Ghazipur, Mughalsarai & Bhadohi (all Nagar Palika Parishad) Obra, Renukoot & Pipri (all Nagar Panchayat) III Class 167 Nakur, Kandhla, Afzalgarh, Seohara, Dhampur, Nehtaur, Noorpur, Thakurdwara, Bilari, Bahjoi, Tanda, Bilaspur, (20,000 - 49,999 Population) Suar, Milak, Bachhraon, Dhanaura, Sardhana, Bagpat, Garmukteshwer, Anupshahar, Gulathi, Siana, Dibai, Shikarpur, Atrauli, Khair, Sikandra -

District Census Hand Book, Jhansi, Part-XIII B, Series-22, Uttar Pradesh
CENSUS 1981 "'ff XIII - if J)"l1/S ER I E S- 22 ~T,"qCfi ifif''lQfifl ..... 'iTl,{ S1~ m~ UTTA.R PRADESH Part XIII .. B PRIMARY CEiSUS ABSTRACt ftf~l ~l Itm \iff111'OT~ T DISTRICT ~~f~~ JHANSI DISTRICT CENSUS HANDBOOK ~f'I ~ srvr.mr. "' f~ ~Ifr qf(".e", ~rivl .,." lIUSTllHCT JHANSI 'I- 1+- ~ ~ :; " 'I- .l. 3g' 1.1- I :1: A '} r;;E,o. I BOUNDARIE5;-STAT£ • DISTRICT • TAHSIL ,1IH<A5KHAND. • •• __,-._._._, •••••••••••• HlGHWAYS:- NATIONAL. STATE. ,,,,,PORTA,,r «TALL ED ROAD. RAIL.WAY LINES WITH STJ,TION:_ BROAD GAUGE RIVER ANO STREAIII HEAOQfJARTERS:- DISTRICT. TAHSIL I VIKASKHAND • • • sih Clen 01 urba Cent,., UR(!AN CENTRE. • • ~- '~LAGE HAVING .5000&' AIIOVE POfIIUV\TlDN 1II1TH "'AlE • •• .51ori tIoOST' ~"'D TEl£GRAPH OFFICE', •• , .. P70 \io)I- -- DEGREE COLLE6£. • CJ T£CHNfCAL INSTITUTION. • • G;I OWIGALOW5:-DAK I TRAVELLERS. III'.PECTIOII • f). ~ TB • lB REST HOUSE RH --L--. ~ ~T "l'T ~ ~ ~IlFrr ~fJOif sTU ~'Ff;:;ro ~ "A'rrurrrT ~~ffirifiT, ~rrUfifT i:fiT ~ifi 31ClRf +tWq~ 'SI"f1J!1I'i ~ I ~ G1'i~lol'il ~~ffCt"fll iflT ~Tlf '1:flG1'iI"flI{if>I, '5f!lf~ifiT, fcnrTrrT ~ ~aff iF irm 0fUCl'{ f.t;<:rT G1lCfT ~ I frrcrT"f'i' ~~ iF f'"laY{o(, til{ l;:fTlf ~ ~1<r ~raiT it; SfrrR ~T fGrffi' 51 !ill ~FT it WCfiT fcriTq- ~01 ~ I fG1\1T ~orrrT {ffi:!R=aiflT ~"fI1fr:f itm srifirnif ~ ~ f1.fi 5fT~q-"I' ,ifiFTIlfi'IT «n: ~ ~, IDlftur ~T iii;;m:r ~ q-'{ ~ 'i<T'{ ~~ ~ qri ~T'{ ~ ~f ~ I ;;rr+rl ~ct 'i'lTU if ~q~;;;cr WqmarT «HT"'eft O1i"fl~ anf~ \it ~ ~8' ~ orr:; ~ r ~ ~rr~r ~f«r<flT ~.~ ifJr sr~ 1 95 1 <Fr 'iAlTorrrr it gaIT I '!i~ f~ if; 5f~~ qrr:r Oi'h: 'Pf'{ itl fu~ 5I~"fI" GF"I"IOI<'lT «R CfI!fT GAtT1l1'iT ctT ~ «mUf1:fT Slifilfuo' cpT trf' IItfT I 1961 iflT \ififOfUfifT it ~T Gj";::rtT11fi1l ~f~T CfIT ~ f~Cf "fI"'{ f~~ ~P:rr 0I!fT ~ <fiT m,{UfRififl ~ smmtir"fl"~, GI<'I'Ij OIi1T 'El1'(f\J[lIi Cf€fT IDl1 ~ if<r"< f.:J~fllTCflr mit 5fT~fl1cf} GfiFTlIT'iT ID'{ ~T w:rr, 51 ... -
CUG No. / Email ID of JAIL OFFICIALS of up Sl.N Name of Institution Designation Mobile N0
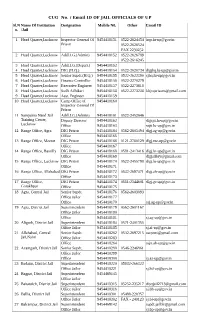
CUG No. / Email ID OF JAIL OFFICIALS OF UP Sl.N Name Of Institution Designation Mobile N0. Other Email ID o. /Jail 1 Head Quarter,Lucknow Inspector General Of 9454418151 0522-2624454 [email protected] Prison 0522-2626524 FAX 2230252 2 Head Quarter,Lucknow Addl.I.G.(Admin) 9454418152 0522-2626789 0522-2616245 3 Head Quarter,Lucknow Addl.I.G.(Depart.) 9454418153 4 Head Quarter,Lucknow DIG (H.Q.) 9454418154 0522-2620734 [email protected] 5 Head Quarter,Lucknow Senior Supdt.(H.Q.) 9454418155 0522-2622390 [email protected] 6 Head Quarter,Lucknow Finance Controller 9454418156 0522-2270279 7 Head Quarter,Lucknow Executive Engineer 9454418157 0522-2273618 8 Head Quarter,Lucknow Sodh Adhikari 9454418158 0522-2273238 [email protected] 9 Head Quarter,Lucknow Asst. Engineer 9454418159 10 Head Quarter,Lucknow Camp Office of 9454418160 Inspector General Of Prison 11 Sampurna Nand Jail Addl.I.G.(Admin) 9454418161 0522-2452646 Training Center, Deputy Director 9454418162 [email protected] Lucknow Office 9454418163 [email protected] 12 Range Office, Agra DIG Prison 9454418164 0562-2605494 [email protected] Office 9454418165 13 Range Office, Meerut DIG Prison 9454418166 0121-2760129 [email protected] Office 9454418167 14 Range Office, Bareilly DIG Prison 9454418168 0581-2413416 [email protected] Office 9454418169 [email protected] 15 Range Office, Lucknow DIG Prison 9454418170 0522-2455798 [email protected] Office 9454418171 16 Range Office, Allahabad DIG Prison 9454418172 0532-2697471 [email protected] Office 9454418173 17 Range Office, DIG Prison 9454418174 0551-2344601 [email protected] Gorakhpur Office 9454418175 18 Agra, Central Jail Senior Supdt. -
B H I N D D a T I a J a L a U N Jhansi Lalitpur
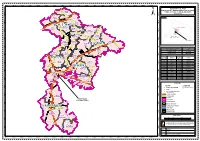
77°30'0"E 77°40'0"E 77°50'0"E 78°0'0"E 78°10'0"E 78°20'0"E 78°30'0"E 78°40'0"E 78°50'0"E 79°0'0"E 79°10'0"E 79°20'0"E 79°30'0"E 79°40'0"E 79°50'0"E 80°0'0"E 80°10'0"E 80°20'0"E 80°30'0"E ¤£2A GEOGRAPHICAL AREA JHANSI (EXCEPT AREA ALREADY AUTHORIZED), ¤£2 CA-10 N ! N BHIND, JALAUN, LALITPUR AND DATIA " ATER " 0 0 ' Chomho 719 ' 0 ¤£ 0 4 4 DISTRICTS ° ° 6 Sukand ! (! Phuphkalan 6 2 ! Para ± 2 Jawasa ! CA-11 Seoda ! ! KEY MAP BÁhind ! Kachogara GORMI (! ! (! Á! !. Bhind Kanavar Manhad ! Akoda Gormi Á! ! N Endori ( N " ! ! Umri " 0 Á 0 ' ! ' 0 Babedi ! 0 3 Sherpur Á! (! ! 3 ° ! Mehgaon Nunahata ° 6 Goara CA-09 6 2 Á! ! ! 2 Bilaw BHIND Á! ! (! GohadB H I N D Á Jagammanpur CA-12 ! CA-13 MEHGAON U T TA R P R A D E S H N CA-08 Kuthond ! N " Rampura " Malanpur (! ! 0 Gaheli (! Umri 0 ' GOHAD ! Roan ! ' 0 ( 0 Amayan RON Machhand 2 ! 2 ° ! CA-04 Ajitapur ° 6 ! 6 2 Sirsakalar 2 Mihona (! MADHOGARH ! Mau Rahawali (! ! ( Ubari Madhogarh ! Gopalpura Saravan CA-07 ! ! CA-03 MIHONA ! M A D H Y A N (! N " Bangra JALAUN " 0 0 P R A D E S H ' Lahar ' 0 Seondha 70 0 1 ¤£ 1 ° (! Khaksis ! ° 6 Aswar (! 6 2 ! !. Jalaun 2 Musmirya (!!Kalpi Area Excluded Nadigaon ! Á (Part Jhansi District) CA-14 CA-06 (! CA-01 ! SEONDHA LAHAR KALPÁI ¤£91 CA-05 J A L A U N Á!! Aata N Alampur (! N " KONCH ! Akbarpur " 0 ! 0 ' Tharet (! ! Babina ' 0 0 ° (!! (! ° 6 Daboh ÁKonch !Orai ! (! Kadaura 6 2 45 Á 2 ¤£ Margaya ! Parsan Total Geographical Area (Sq Km) 21,888 Á ! Lohagarh CA-02 ! No. -

Brief Industrial Profile of Jhansi District
lR;eso t;rs Government of India Ministry of MSME Brief Industrial Profile of Jhansi District MSME-Development Institute,Kanpur (Ministry of MSME, Govt. of India,) Phone: 0512-2295070-73 Fax: 0512-2240143 E-mail : [email protected] Web- msmedikanpur.gov.in Compiled by – Kashi Prasad Sheel Investigator (L/F) 1 Contents S. No. Topic Page No. 1. General Characteristics of the District 03 1.1 Location & Geographical Area 03-04 1.2 Topography 04-05 1.3 Availability of Minerals. 05 1.4 Forest 05 1.5 Administrative set up 06 2. District at a glance 06-08 2.1 Existing Status of Industrial Area in the District Jhansi 09 3. Industrial Scenario Of Jhansi 09 3.1 Industry at a Glance 10 3.2 Year Wise Trend Of Units Registered 10 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units In The 11 District 3.4 Large Scale Industries / Public Sector undertakings 11 3.5 Major Exportable Item 12 3.6 Growth Trend 12 3.7 Vendorisation / Ancillarisation of the Industry 12 3.8 Medium Scale Enterprises 12 3.8.1 List of the units in Jhansi & near by Area 12 3.8.2 Major Exportable Item 12 3.9 Service Enterprises 12 3.9.1 Coaching Industry 12 3.9.2 Potentials areas for service industry 12 3.10 Potential for new MSMEs 13 4. Existing Clusters of Micro & Small Enterprise 13 4.1 Detail Of Major Clusters 13 4.1.1 Manufacturing Sector 13 4.1.2 Service Sector 13 4.2 Details of Identified cluster 13 5. -

Districts Visited by Joint Inspecti and Other Central Scheme
Districts Visited By Joint Inspection Team to Review of NHM and other Central Scheme of Horticulture Supported for Uttar Pradesh for the year 2010 . Chitrakoot Jhansi Banda Allahabad Kaushambi Bareilly Sultanpur Lucknow Varanasi Moradabad Barabanki Report of Joint Inspection Team to Review N ational Horticulture Mission and other Central Scheme of Horticulture Supported for Uttar Pradesh for the year 2010 National Horticulture Mission Department of Agriculture and Cooperation JIT Team members to evaluate Horticultural programmes: The Joint Inspection Team was constituted of Dr R.C Upadhyaya Chief Consultant NHM; Dr. V. K. Singh, Principal Scientist (crop production), CISH (ICAR) Rahmenkhera, Kokoni, Lucknow- 227107(U.P). Dr. H. S. Shukla, Head of Horticulture Dept. CSA University of Agri. Tech. Kanpur- 208002(U.P).team Coordinator Sri S. P. Joshi, Joint Director (Hort.), Govt. of U.P. Deputy Director/District Horticulture Officer of the respective Divisions/Districts are also member of the JIT team. Visit Schedule: Dates Districts visited 21 st Oct to 27 th Oct Jhansi, Banda & Chitrakoot 2010 22 nd Nov to 27 th Nov Allahabad, Banaras & Kaushambi 2010 27 th Dec to 31 st Dec Lucknow, Barabanki, Sultanpur, Bareilly & Moradabad 2010 Meeting with state level of NHM officials: On 22 nd Nov., 2010 a meeting was held in the office of the Joint Director Horticulture and Nodal Officer SHM, Govt. of U.P., Lucknow with the deputy Directors and District Horticulture Officers of the visiting districts and discussed the scheme progress of their districts. The team also reviewed the progress of work done including financial details. JIT selected randomly the field visit programme of few selected sites at Allahabad, Kausambi and Banaras and discussed the work done report of Jhansi, Banda and Chitrakoot. -

Integrated Area Devdopment Plan for District Jhansi
Integrated Area Devdopment Plan for District Jhansi N IE PA D C D00348 AREA PLANNING DIVISION STATE PLANNING INSTITUTE UTTAR PRADESH SEPTEMBER, 1980 \> Sub. Nationsl Systems KaHonal Institute of Edncatioiiat Planning pr. i ministration 17-B,SriAurt.; M .NewDelhi-110016 Date...... Ihe fifth Jive Year PlaA had recommended the formulation 3f location ^scifLc integrated area developnait-pl^ for each dLs- trlct in the countiy. Ihe present stacfy, **Integrated ^Area Develop- ment Plan f»r QLstilct JhansL** i s "ttie first attempt made in this State. The studfer under-taken by the State Planning Institute sati'^fies some of the main criteria laid dovn by the Planning Commission, Govem4ent of India* Ihou^ the integrated area deve lopment plan h;as been prepared for the district Jhgglai it s implica tions are much vdder and, the methodology adopted i s replicable in other distilcts of the State with seme modifications, Ihe-present stac^ i s , thus, an im port^t step in the foimulation of the integrated area p l^s , Ihe stu<%- provides necessary locational guid^nes for establi^ng various institu- tions ^ d facilities in specific areas of the district end suggests impl on citation of in t ^ _ sectoral programmes in an integrated manner. In fact, area planning has beoi recognised as an indLsensible tech nique for comprdiensive development of ?si area based on integration of functional ^ d spatial factors vhich msy furtLier ensure proper linkages in the inter-sectoral pmgr^Emes to derive an optimum benefit for -fche inhabitants of tiie area on -ttieir impl an station. Ihe methodology pursued in the study i s bound to improve in the subsequent exercises vhich be under-taken in other district of the State. -

United Provinces of Agra and Oudh, Vol-XVI, Uttar Pradesh
CENSUS OF INDIA, 1921 UI'JITED PROVINCES OF AGRA AND OUDH Volume XVI Part I-REPORT fly E. H. H. EDYE, I.GS., StTPERINTENDENT, CENSUS OPERATIQ;'oIS ALLAHABAD: Soperintendent, Government Press. United Provinces 1 923 LIST OF ERRATA. Owing to a clerical error due to acres having been entered as square miles, Pilibhit district bu.;; wrongly been credited in the text of the Introduction and Cha.pter I with an additional 203 square miles. This error makes no di t1erence to the cOllclusions drawn, but for the sake of accuracy tho following emendation:! are necessary :- (1) Intra luction, page I.-Substitute for inset, .. additions '1 square miles, popula tioD 5,213, deductions 109 square miles, population 2l,929, differenctl-l02 sq. miles, population 16,'116. ~21 Chapter I, page 7, I.-Area is 112,244 sq. miles (102 sq. miles less than in 1911). Of these 106,295 belong to Bricish districts and 5,949 to states. At foot of page. Delete" Pilibhit, ecc.", and substitute (ia C( area subtracted" column) ,. minor changes 15 sq. miles, population 767." ,3) au page 8 in inset substitute in " percentage of provincial area" column in (2) 9'3; in (4 21'3; in (6) 4.-1. (4) Page 13, footnote I.-Substitute" Public Health figures are for the calendar year, Administration Report figures for the financial year-1st April to 31st March. (5) On page 17.-Inset., opposite Sub-Himalaya, West,jor'( 399" read" 407." (6) On page 19, line 1, subst Ltu.te .. lU densit.y sub-Himalaya West and Western Plain h~ve decreased most (30)." TABLE OF CONTENTS. -

Brief Industrial Profile
MINISTRY OF MICRO, SMALL & MEDIUM ENTERPRISES GOVERNMENT OF INDIA Brief Industrial Profile of District Jhansi U.P. Prepared by MSME-DEVELOPMENT INSTITUTE (Ministry of MSME, Govt.of India) 107, Industrial Estate, Kalpi Road, Fazalganj, Kanpur-208012 Phone: 0512-2295070-73, Fax: 0512-2240143 E-mail : [email protected] Web- msmedikanpur.gov.in CONTENTS S.No. Topic Page No. 1. General Characteristics of the District 3 1.1 Location & Geographical Area 3 1.2 Topography 4 1.3 Availability of Minerals. 5 1.4 Forest 5 1.5 Administrative Set Up 6 2. District at a Glance 6 2.1 Existing Status of Industrial Area in the District Jhansi 9 3. Industrial Scenario of Jhansi 10 3.1 Year Wise Trend of Units Registered 10 3.2 Details of Existing Manufacturing Enterprises with 2 Digit National 11 Industry Classification Code 3.3 Details of Existing Service Enterprises with 2 Digit National Industry 13 Classification Code 3.4 Large Scale Industries / Public Sector undertakings 14 3.5 Major Exportable Item 15 3.6 Growth Trend 16 3.7 Vendorisation / Ancillarisation of the Industry 16 3.8 Service Enterprises 16 3.9 Potential for New MSMEs 17 3.9.1 Potentials Areas for Service Sectors 17 3.9.2 Potentials Areas for Manufacturing Sectors 17 3.10 One District One Product Scheme of Uttar Pradesh 17 4. Existing Clusters of Micro & Small Enterprise 18 4.1 Detail of Major Clusters 18 4.1.1 Manufacturing Sector 18 4.1.2 Service Sector 18 4.2 Details of Identified Cluster 18 5. General Issues Raised by Industry Associations During the course of 19 Meeting 6 Programmes Conducted During 2017-18 19 7.