Whole Exome Sequencing Analysis of Intracranial
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cow's Milk Allergy in Dutch Children
Petrus et al. Clin Transl Allergy (2016) 6:16 DOI 10.1186/s13601-016-0105-z Clinical and Translational Allergy RESEARCH Open Access Cow’s milk allergy in Dutch children: an epigenetic pilot survey Nicole C. M. Petrus1*†, Peter Henneman2†, Andrea Venema2, Adri Mul2, Femke van Sinderen2, Martin Haagmans2, Olaf Mook2, Raoul C. Hennekam1,2, Aline B. Sprikkelman1‡ and Marcel Mannens2‡ Abstract Background: Cow’s milk allergy (CMA) is a common disease in infancy. Early environmental factors are likely to con- tribute to CMA. It is known that epigenetic gene regulation can be altered by environmental factors. We have set up a proof of concept study, aiming to detect epigenetic associations specific with CMA. Methods: We studied children from the Dutch EuroPrevall birth cohort study (N 20 CMA, N 23 controls, N 10 tolerant boys), age and gender matched. CMA was challenge proven. Bisulfite converted= DNA =(blood) was analyzed= using the 450K infinium DNA-methylation array. Four groups (combined, girls, boys and tolerant boys) were analysed between CMA and controls. Statistical analysis and pathway-analysis were performed in “R” using IMA, Minfi and the global-test package. Differentially methylated regions in DHX58, ZNF281, EIF42A and HTRA2 genes were validated by quantitative amplicon sequencing (ROCHE 454®). Results: General hypermethylation was found in the CMA group compared to control children, while this effect was absent in the tolerant group. Methylation differences were, among others, found in regions of DHX58, ZNF281, EIF42A and HTRA2 genes. Several of these genes are known to be involved in immunological pathways and associated with other allergies. Conclusion: We show that epigenetic associations are involved in CMA. -

Essential Genes and Their Role in Autism Spectrum Disorder
University of Pennsylvania ScholarlyCommons Publicly Accessible Penn Dissertations 2017 Essential Genes And Their Role In Autism Spectrum Disorder Xiao Ji University of Pennsylvania, [email protected] Follow this and additional works at: https://repository.upenn.edu/edissertations Part of the Bioinformatics Commons, and the Genetics Commons Recommended Citation Ji, Xiao, "Essential Genes And Their Role In Autism Spectrum Disorder" (2017). Publicly Accessible Penn Dissertations. 2369. https://repository.upenn.edu/edissertations/2369 This paper is posted at ScholarlyCommons. https://repository.upenn.edu/edissertations/2369 For more information, please contact [email protected]. Essential Genes And Their Role In Autism Spectrum Disorder Abstract Essential genes (EGs) play central roles in fundamental cellular processes and are required for the survival of an organism. EGs are enriched for human disease genes and are under strong purifying selection. This intolerance to deleterious mutations, commonly observed haploinsufficiency and the importance of EGs in pre- and postnatal development suggests a possible cumulative effect of deleterious variants in EGs on complex neurodevelopmental disorders. Autism spectrum disorder (ASD) is a heterogeneous, highly heritable neurodevelopmental syndrome characterized by impaired social interaction, communication and repetitive behavior. More and more genetic evidence points to a polygenic model of ASD and it is estimated that hundreds of genes contribute to ASD. The central question addressed in this dissertation is whether genes with a strong effect on survival and fitness (i.e. EGs) play a specific oler in ASD risk. I compiled a comprehensive catalog of 3,915 mammalian EGs by combining human orthologs of lethal genes in knockout mice and genes responsible for cell-based essentiality. -

Genetic Analysis of Indel Markers in Three Loci Associated with Parkinson’S Disease
RESEARCH ARTICLE Genetic analysis of indel markers in three loci associated with Parkinson's disease Zhixin Huo1, Xiaoguang Luo2, Xiaoni Zhan1, Qiaohong Chu1, Qin Xu1, Jun Yao1, Hao Pang1* 1 Department of Forensic Genetics and Biology, China Medical University, Shenyang North New Area, Shenyang, P.R., China, 2 Department of Neurology, 1st Affiliated Hospital of China Medical University, Shenyang, P.R., China * [email protected] Abstract a1111111111 a1111111111 The causal mutations and genetic polymorphisms associated with susceptibility to Parkin- a1111111111 son's disease (PD) have been extensively described. To explore the potential contribution a1111111111 a1111111111 of insertion (I)/deletion (D) polymorphisms (indels) to the risk of PD in a Chinese population, we performed genetic analyses of indel loci in ACE, DJ-1, and GIGYF2 genes. Genomic DNA was extracted from venous blood of 348 PD patients and 325 age- and sex-matched controls without neurodegenerative disease. Genotyping of the indel loci was performed by fragment length analysis after PCR and DNA sequencing. Our results showed a statistically OPEN ACCESS significant association for both allele X (alleles without 5) vs. 5 (odds ratio = 1.378, 95% con- Citation: Huo Z, Luo X, Zhan X, Chu Q, Xu Q, Yao fidence interval = 1.112±1.708, P = 0.003) and genotype 5/X+X/X vs. 5/5 (odds ratio = J, et al. (2017) Genetic analysis of indel markers in three loci associated with Parkinson's disease. 1.681, 95% confidence interval = 1.174±2.407, P = 0.004) in the GIGYF2 locus; however, PLoS ONE 12(9): e0184269. https://doi.org/ no significant differences were detected for the ACE and DJ-1 indels. -

Whole Exome Sequencing in Families at High Risk for Hodgkin Lymphoma: Identification of a Predisposing Mutation in the KDR Gene
Hodgkin Lymphoma SUPPLEMENTARY APPENDIX Whole exome sequencing in families at high risk for Hodgkin lymphoma: identification of a predisposing mutation in the KDR gene Melissa Rotunno, 1 Mary L. McMaster, 1 Joseph Boland, 2 Sara Bass, 2 Xijun Zhang, 2 Laurie Burdett, 2 Belynda Hicks, 2 Sarangan Ravichandran, 3 Brian T. Luke, 3 Meredith Yeager, 2 Laura Fontaine, 4 Paula L. Hyland, 1 Alisa M. Goldstein, 1 NCI DCEG Cancer Sequencing Working Group, NCI DCEG Cancer Genomics Research Laboratory, Stephen J. Chanock, 5 Neil E. Caporaso, 1 Margaret A. Tucker, 6 and Lynn R. Goldin 1 1Genetic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 2Cancer Genomics Research Laboratory, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 3Ad - vanced Biomedical Computing Center, Leidos Biomedical Research Inc.; Frederick National Laboratory for Cancer Research, Frederick, MD; 4Westat, Inc., Rockville MD; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; and 6Human Genetics Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD, USA ©2016 Ferrata Storti Foundation. This is an open-access paper. doi:10.3324/haematol.2015.135475 Received: August 19, 2015. Accepted: January 7, 2016. Pre-published: June 13, 2016. Correspondence: [email protected] Supplemental Author Information: NCI DCEG Cancer Sequencing Working Group: Mark H. Greene, Allan Hildesheim, Nan Hu, Maria Theresa Landi, Jennifer Loud, Phuong Mai, Lisa Mirabello, Lindsay Morton, Dilys Parry, Anand Pathak, Douglas R. Stewart, Philip R. Taylor, Geoffrey S. Tobias, Xiaohong R. Yang, Guoqin Yu NCI DCEG Cancer Genomics Research Laboratory: Salma Chowdhury, Michael Cullen, Casey Dagnall, Herbert Higson, Amy A. -
Supplementary Data
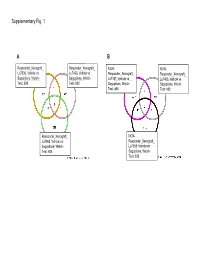
Supplementary Fig. 1 A B Responder_Xenograft_ Responder_Xenograft_ NON- NON- Lu7336, Vehicle vs Lu7466, Vehicle vs Responder_Xenograft_ Responder_Xenograft_ Sagopilone, Welch- Sagopilone, Welch- Lu7187, Vehicle vs Lu7406, Vehicle vs Test: 638 Test: 600 Sagopilone, Welch- Sagopilone, Welch- Test: 468 Test: 482 Responder_Xenograft_ NON- Lu7860, Vehicle vs Responder_Xenograft_ Sagopilone, Welch - Lu7558, Vehicle vs Test: 605 Sagopilone, Welch- Test: 333 Supplementary Fig. 2 Supplementary Fig. 3 Supplementary Figure S1. Venn diagrams comparing probe sets regulated by Sagopilone treatment (10mg/kg for 24h) between individual models (Welsh Test ellipse p-value<0.001 or 5-fold change). A Sagopilone responder models, B Sagopilone non-responder models. Supplementary Figure S2. Pathway analysis of genes regulated by Sagopilone treatment in responder xenograft models 24h after Sagopilone treatment by GeneGo Metacore; the most significant pathway map representing cell cycle/spindle assembly and chromosome separation is shown, genes upregulated by Sagopilone treatment are marked with red thermometers. Supplementary Figure S3. GeneGo Metacore pathway analysis of genes differentially expressed between Sagopilone Responder and Non-Responder models displaying –log(p-Values) of most significant pathway maps. Supplementary Tables Supplementary Table 1. Response and activity in 22 non-small-cell lung cancer (NSCLC) xenograft models after treatment with Sagopilone and other cytotoxic agents commonly used in the management of NSCLC Tumor Model Response type -

Hippo and Sonic Hedgehog Signalling Pathway Modulation of Human Urothelial Tissue Homeostasis
Hippo and Sonic Hedgehog signalling pathway modulation of human urothelial tissue homeostasis Thomas Crighton PhD University of York Department of Biology November 2020 Abstract The urinary tract is lined by a barrier-forming, mitotically-quiescent urothelium, which retains the ability to regenerate following injury. Regulation of tissue homeostasis by Hippo and Sonic Hedgehog signalling has previously been implicated in various mammalian epithelia, but limited evidence exists as to their role in adult human urothelial physiology. Focussing on the Hippo pathway, the aims of this thesis were to characterise expression of said pathways in urothelium, determine what role the pathways have in regulating urothelial phenotype, and investigate whether the pathways are implicated in muscle-invasive bladder cancer (MIBC). These aims were assessed using a cell culture paradigm of Normal Human Urothelial (NHU) cells that can be manipulated in vitro to represent different differentiated phenotypes, alongside MIBC cell lines and The Cancer Genome Atlas resource. Transcriptomic analysis of NHU cells identified a significant induction of VGLL1, a poorly understood regulator of Hippo signalling, in differentiated cells. Activation of upstream transcription factors PPARγ and GATA3 and/or blockade of active EGFR/RAS/RAF/MEK/ERK signalling were identified as mechanisms which induce VGLL1 expression in NHU cells. Ectopic overexpression of VGLL1 in undifferentiated NHU cells and MIBC cell line T24 resulted in significantly reduced proliferation. Conversely, knockdown of VGLL1 in differentiated NHU cells significantly reduced barrier tightness in an unwounded state, while inhibiting regeneration and increasing cell cycle activation in scratch-wounded cultures. A signalling pathway previously observed to be inhibited by VGLL1 function, YAP/TAZ, was unaffected by VGLL1 manipulation. -

"The Genecards Suite: from Gene Data Mining to Disease Genome Sequence Analyses". In: Current Protocols in Bioinformat
The GeneCards Suite: From Gene Data UNIT 1.30 Mining to Disease Genome Sequence Analyses Gil Stelzer,1,5 Naomi Rosen,1,5 Inbar Plaschkes,1,2 Shahar Zimmerman,1 Michal Twik,1 Simon Fishilevich,1 Tsippi Iny Stein,1 Ron Nudel,1 Iris Lieder,2 Yaron Mazor,2 Sergey Kaplan,2 Dvir Dahary,2,4 David Warshawsky,3 Yaron Guan-Golan,3 Asher Kohn,3 Noa Rappaport,1 Marilyn Safran,1 and Doron Lancet1,6 1Department of Molecular Genetics, Weizmann Institute of Science, Rehovot, Israel 2LifeMap Sciences Ltd., Tel Aviv, Israel 3LifeMap Sciences Inc., Marshfield, Massachusetts 4Toldot Genetics Ltd., Hod Hasharon, Israel 5These authors contributed equally to the paper 6Corresponding author GeneCards, the human gene compendium, enables researchers to effectively navigate and inter-relate the wide universe of human genes, diseases, variants, proteins, cells, and biological pathways. Our recently launched Version 4 has a revamped infrastructure facilitating faster data updates, better-targeted data queries, and friendlier user experience. It also provides a stronger foundation for the GeneCards suite of companion databases and analysis tools. Improved data unification includes gene-disease links via MalaCards and merged biological pathways via PathCards, as well as drug information and proteome expression. VarElect, another suite member, is a phenotype prioritizer for next-generation sequencing, leveraging the GeneCards and MalaCards knowledgebase. It au- tomatically infers direct and indirect scored associations between hundreds or even thousands of variant-containing genes and disease phenotype terms. Var- Elect’s capabilities, either independently or within TGex, our comprehensive variant analysis pipeline, help prepare for the challenge of clinical projects that involve thousands of exome/genome NGS analyses. -

Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva
UCSF UC San Francisco Previously Published Works Title Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva. Permalink https://escholarship.org/uc/item/95h5g8mq Journal Cell reports, 33(7) ISSN 2211-1247 Authors Saitou, Marie Gaylord, Eliza A Xu, Erica et al. Publication Date 2020-11-01 DOI 10.1016/j.celrep.2020.108402 Peer reviewed eScholarship.org Powered by the California Digital Library University of California HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Cell Rep Manuscript Author . Author manuscript; Manuscript Author available in PMC 2020 November 30. Published in final edited form as: Cell Rep. 2020 November 17; 33(7): 108402. doi:10.1016/j.celrep.2020.108402. Functional Specialization of Human Salivary Glands and Origins of Proteins Intrinsic to Human Saliva Marie Saitou1,2,3, Eliza A. Gaylord4, Erica Xu1,7, Alison J. May4, Lubov Neznanova5, Sara Nathan4, Anissa Grawe4, Jolie Chang6, William Ryan6, Stefan Ruhl5,*, Sarah M. Knox4,*, Omer Gokcumen1,8,* 1Department of Biological Sciences, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 2Section of Genetic Medicine, Department of Medicine, University of Chicago, Chicago, IL, U.S.A 3Faculty of Biosciences, Norwegian University of Life Sciences, Ås, Viken, Norway 4Program in Craniofacial Biology, Department of Cell and Tissue Biology, School of Dentistry, University of California, San Francisco, CA, U.S.A 5Department of Oral Biology, School of Dental Medicine, University at Buffalo, The State University of New York, Buffalo, NY, U.S.A 6Department of Otolaryngology, School of Medicine, University of California, San Francisco, CA, U.S.A 7Present address: Weill-Cornell Medical College, Physiology and Biophysics Department 8Lead Contact SUMMARY Salivary proteins are essential for maintaining health in the oral cavity and proximal digestive tract, and they serve as potential diagnostic markers for monitoring human health and disease. -

Deciphering the Molecular Profile of Plaques, Memory Decline And
ORIGINAL RESEARCH ARTICLE published: 16 April 2014 AGING NEUROSCIENCE doi: 10.3389/fnagi.2014.00075 Deciphering the molecular profile of plaques, memory decline and neuron loss in two mouse models for Alzheimer’s disease by deep sequencing Yvonne Bouter 1†,Tim Kacprowski 2,3†, Robert Weissmann4, Katharina Dietrich1, Henning Borgers 1, Andreas Brauß1, Christian Sperling 4, Oliver Wirths 1, Mario Albrecht 2,5, Lars R. Jensen4, Andreas W. Kuss 4* andThomas A. Bayer 1* 1 Division of Molecular Psychiatry, Georg-August-University Goettingen, University Medicine Goettingen, Goettingen, Germany 2 Department of Bioinformatics, Institute of Biometrics and Medical Informatics, University Medicine Greifswald, Greifswald, Germany 3 Department of Functional Genomics, Interfaculty Institute for Genetics and Functional Genomics, University Medicine Greifswald, Greifswald, Germany 4 Human Molecular Genetics, Department for Human Genetics of the Institute for Genetics and Functional Genomics, Institute for Human Genetics, University Medicine Greifswald, Ernst-Moritz-Arndt University Greifswald, Greifswald, Germany 5 Institute for Knowledge Discovery, Graz University of Technology, Graz, Austria Edited by: One of the central research questions on the etiology of Alzheimer’s disease (AD) is the Isidro Ferrer, University of Barcelona, elucidation of the molecular signatures triggered by the amyloid cascade of pathological Spain events. Next-generation sequencing allows the identification of genes involved in disease Reviewed by: Isidro Ferrer, University of Barcelona, processes in an unbiased manner. We have combined this technique with the analysis of Spain two AD mouse models: (1) The 5XFAD model develops early plaque formation, intraneu- Dietmar R. Thal, University of Ulm, ronal Ab aggregation, neuron loss, and behavioral deficits. (2)TheTg4–42 model expresses Germany N-truncated Ab4–42 and develops neuron loss and behavioral deficits albeit without plaque *Correspondence: formation. -

A Genomics Approach Reveals Insights Into the Importance of Gene Losses for Mammalian Adaptations
Corrected: Publisher correction ARTICLE DOI: 10.1038/s41467-018-03667-1 OPEN A genomics approach reveals insights into the importance of gene losses for mammalian adaptations Virag Sharma1,2,3, Nikolai Hecker1,2,3, Juliana G. Roscito1,2,3, Leo Foerster1,2,3, Bjoern E. Langer1,2,3 & Michael Hiller1,2,3 1234567890():,; Identifying the genomic changes that underlie phenotypic adaptations is a key challenge in evolutionary biology and genomics. Loss of protein-coding genes is one type of genomic change with the potential to affect phenotypic evolution. Here, we develop a genomics approach to accurately detect gene losses and investigate their importance for adaptive evolution in mammals. We discover a number of gene losses that likely contributed to morphological, physiological, and metabolic adaptations in aquatic and flying mammals. These gene losses shed light on possible molecular and cellular mechanisms that underlie these adaptive phenotypes. In addition, we show that gene loss events that occur as a consequence of relaxed selection following adaptation provide novel insights into species’ biology. Our results suggest that gene loss is an evolutionary mechanism for adaptation that may be more widespread than previously anticipated. Hence, investigating gene losses has great potential to reveal the genomic basis underlying macroevolutionary changes. 1 Max Planck Institute of Molecular Cell Biology and Genetics, Pfotenhauerstr. 108, 01307 Dresden, Germany. 2 Max Planck Institute for the Physics of Complex Systems, Noethnitzer Str. 38, 01187 Dresden, Germany. 3 Center for Systems Biology Dresden, Pfotenhauerstr. 108, 01307 Dresden, Germany. Correspondence and requests for materials should be addressed to M.H. (email: [email protected]) NATURE COMMUNICATIONS | (2018) 9:1215 | DOI: 10.1038/s41467-018-03667-1 | www.nature.com/naturecommunications 1 ARTICLE NATURE COMMUNICATIONS | DOI: 10.1038/s41467-018-03667-1 ne of the most fascinating aspects of nature is the a b % conserved genes diversity of life. -

Transdifferentiation of Human Mesenchymal Stem Cells
Transdifferentiation of Human Mesenchymal Stem Cells Dissertation zur Erlangung des naturwissenschaftlichen Doktorgrades der Julius-Maximilians-Universität Würzburg vorgelegt von Tatjana Schilling aus San Miguel de Tucuman, Argentinien Würzburg, 2007 Eingereicht am: Mitglieder der Promotionskommission: Vorsitzender: Prof. Dr. Martin J. Müller Gutachter: PD Dr. Norbert Schütze Gutachter: Prof. Dr. Georg Krohne Tag des Promotionskolloquiums: Doktorurkunde ausgehändigt am: Hiermit erkläre ich ehrenwörtlich, dass ich die vorliegende Dissertation selbstständig angefertigt und keine anderen als die von mir angegebenen Hilfsmittel und Quellen verwendet habe. Des Weiteren erkläre ich, dass diese Arbeit weder in gleicher noch in ähnlicher Form in einem Prüfungsverfahren vorgelegen hat und ich noch keinen Promotionsversuch unternommen habe. Gerbrunn, 4. Mai 2007 Tatjana Schilling Table of contents i Table of contents 1 Summary ........................................................................................................................ 1 1.1 Summary.................................................................................................................... 1 1.2 Zusammenfassung..................................................................................................... 2 2 Introduction.................................................................................................................... 4 2.1 Osteoporosis and the fatty degeneration of the bone marrow..................................... 4 2.2 Adipose and bone -

The Interaction of Obesity and Age and Their Effect on Adipose Tissue Metabolism in the Mouse
The Interaction of Obesity and Age and their effect on Adipose Tissue Metabolism in the Mouse A dissertation submitted for the degree of Doctor of Philosophy at the University of Cambridge Ke-di Liu King’s College Declaration This thesis is a summary of research conducted in the Department of Biochemistry, University of Cambridge, between October 2013 and September 2017. This dissertation is the result of my own work and includes nothing which is the outcome of work done in collaboration, except where specially indicated in the text. None of the research described, in its entirety or in part, has been submitted for a degree, diploma or other qualification at any other University. This thesis does not exceed 60,000 words. Abstract Numerous studies have investigated how bulk lipid metabolism is influenced in obesity and in particular how the composition of triglycerides found in the cytosol change with increased adipocyte expansion. However, in part reflecting the analytical challenge the composition of cell membranes, and in particular glycerophospholipids, an important membrane component, have been seldom investigated. Cell membrane components contribute to a variety of cellular processes including maintaining organelle functionality, providing an optimized environment for numerous proteins and providing important pools for metabolites, such as choline for one- carbon metabolism and S-adenosylmethionine for DNA methylation. Here, I have conducted a comprehensive lipidomic and transcriptomic study of white adipose tissue in mice that become obese either through genetic modification (ob/ob genotype), diet (high-fat diet) or a combination of the two across the life course. Specifically, I demonstrated that the changes in triglyceride metabolism that dominate the overall lipid composition of white adipose tissue were distinct from the compositional changes of glycerophospholipids.