COVID-19: What's New for May 29, 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Thursday Calendar 20142018
THURSDAY Five-Year Calendar Unit 2014 20152016 2017 2018 Week # 1 Jan. 2 - Jan. 9 Jan. 1 - Jan. 8 Jan. 7 - Jan. 14 Jan. 5 - Jan. 12 Jan. 4 - Jan. 11 2 Jan. 9 - Jan. 16 Jan. 8 - Jan. 15 Jan. 14 - Jan. 21 Jan. 12 - Jan. 19 Jan. 11 - Jan. 18 3 Jan. 16 - Jan. 23 Jan. 15 - Jan. 22 Jan. 21 - Jan 28 Jan. 19 - Jan. 26 Jan. 18 - Jan. 25 4 Jan. 23 - Jan. 30 Jan. 22 - Jan. 29 Jan. 28 - Feb. 4 Jan. 26 - Feb. 2 Jan. 25 - Feb. 1 5 Jan. 30 - Feb. 6 Jan. 29 - Feb. 5 Feb. 4 - Feb. 11 Feb. 2- Feb. 9 Feb. 1 - Feb. 8 6 Feb. 6 - Feb. 13 Feb. 5 - Feb. 12 Feb. 11 - Feb. 18 Feb. 9 - Feb. 16 Feb. 8 - Feb. 15 7 Feb. 13 - Feb. 20 Feb. 12 - Feb. 19 Feb. 18 - Feb. 25 Feb. 16 - Feb. 23 Feb. 15 - Feb. 22 8 Feb. 20 - Feb. 27 Feb. 19 - Feb. 26 Feb. 25 - Mar. 3 Feb. 23 - Mar. 2 Feb. 22 - Mar. 1 9 Feb. 27 - Mar. 6 Feb. 26 - Mar. 5 Mar. 3 - Mar. 10 Mar. 2 - Mar. 9 Mar. 1 - Mar. 8 10 Mar. 6 - Mar. 13 Mar. 5 - Mar. 12 Mar. 10 - Mar. 17 Mar. 9 - Mar. 16 Mar. 5 - Mar. 15 11 Mar. 13 - Mar. 20 Mar. 12 - Mar. 19 Mar. 17 - Mar. 24 Mar. 16 - Mar. 23 Mar. 15 - Mar. 22 12 Mar. 20 - Mar. 27 Mar. 19 - Mar. 26 Mar. 24 - Mar. 31 Mar. 23 - Mar. 30 Mar. 22 - Mar. -
Dose Timing Calendar.Xlsx
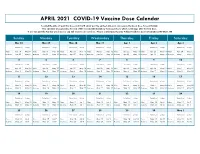
APRIL 2021 COVID-19 Vaccine Dose Calendar Located the date of your first dose and it will show you the earliest date you can receive the boost dose for each brand. This calendar also provides the end of the reccomended window for boost doses which is 42 days after the first dose. If you are past the 42 day window you can still receive a boost dose. Please contact Lane County Public Health for more information 541-682-1380 Sunday Monday Tuesday Wednesday Thursday Friday Saturday Mar 28 Mar 29 Mar 30 Mar 31 Apr 1 Apr 2 Apr 3 Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Pfizer Apr 18 May 9 Pfizer Apr 19 May 10 Pfizer Apr 20 May 11 Pfizer Apr 21 May 12 Pfizer Apr 22 May 13 Pfizer Apr 23 May 14 Pfizer Apr 24 May 15 Moderna Apr 25 May 9 Moderna Apr 26 May 10 Moderna Apr 27 May 11 Moderna Apr 28 May 12 Moderna Apr 29 May 13 Moderna Apr 30 May 14 Moderna May 1 May 15 4 5 6 7 8 9 10 Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Pfizer Apr 25 May 16 Pfizer Apr 26 May 17 Pfizer Apr 27 May 18 Pfizer Apr 28 May 19 Pfizer Apr 29 May 20 Pfizer Apr 30 May 21 Pfizer May 1 May 22 Moderna May 2 May 16 Moderna May 3 May 17 Moderna May 4 May 18 Moderna May 5 May 19 Moderna May 6 May 20 Moderna May 7 May 21 Moderna May 8 May 22 11 12 13 14 15 16 17 Earliest Boost 42 days Earliest Boost 42 days Earliest Boost 42 days Earliest Boost -
2024 7 Day Working Days Calendar
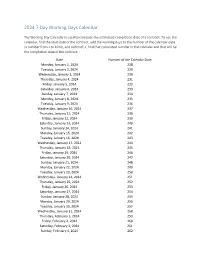
2024 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Monday, January 1, 2024 228 Tuesday, January 2, 2024 229 Wednesday, January 3, 2024 230 Thursday, January 4, 2024 231 Friday, January 5, 2024 232 Saturday, January 6, 2024 233 Sunday, January 7, 2024 234 Monday, January 8, 2024 235 Tuesday, January 9, 2024 236 Wednesday, January 10, 2024 237 Thursday, January 11, 2024 238 Friday, January 12, 2024 239 Saturday, January 13, 2024 240 Sunday, January 14, 2024 241 Monday, January 15, 2024 242 Tuesday, January 16, 2024 243 Wednesday, January 17, 2024 244 Thursday, January 18, 2024 245 Friday, January 19, 2024 246 Saturday, January 20, 2024 247 Sunday, January 21, 2024 248 Monday, January 22, 2024 249 Tuesday, January 23, 2024 250 Wednesday, January 24, 2024 251 Thursday, January 25, 2024 252 Friday, January 26, 2024 253 Saturday, January 27, 2024 254 Sunday, January 28, 2024 255 Monday, January 29, 2024 256 Tuesday, January 30, 2024 257 Wednesday, January 31, 2024 258 Thursday, February 1, 2024 259 Friday, February 2, 2024 260 Saturday, February 3, 2024 261 Sunday, February 4, 2024 262 Date Number of the Calendar Date Monday, February 5, 2024 263 Tuesday, February 6, 2024 264 Wednesday, February -

2021 Calandar
Harbortown Point Marina Resort & Club 2021 Reservation Calendar Written request can be taken at dates indicated Please note: you can only book in Prime season if you own in Prime Season and only below. The dates inform book in High Season if you own in High Season you when the 2021 weeks to the left Friday Saturday Sunday become abailable to Week No. Dates Dates Dates reserve. 1 Jan 1 - Jan 8 Jan 2 - Jan 9 Jan 3 - Jan 10 October 22, 2019 2 Jan 8 - Jan 15 Jan 9 - Jan 16 Jan 10 - Jan 17 October 29, 2019 3 Jan 15 - Jan 22 Jan 16 - Jan 23 Jan 17 - Jan 24 November 5, 2019 4 Jan 22 - Jan 29 Jan 23 - Jan 30 Jan 24 - Jan 31 November 12, 2019 5 Jan 29 - Feb 5 Jan 30 - Feb 6 Jan 31 - Feb 7 November 19, 2019 6 Feb 5 - Feb 12 Feb 6- Feb 13 Feb 7 - Feb 14 November 26, 2019 7 Feb 12 - Feb 19 Feb 13 - Feb 20 Feb 14 - Feb 21 December 3, 2019 8 Feb 19 - Feb 26 Feb 20 - Feb 27 Feb 21 - Feb 28 December 10, 2019 9 Feb 26 - Mar 5 Feb 27 - Mar 6 Feb 28 - Mar 7 December 18, 2018 HIGH 10 Mar 5 - Mar 12 Mar 6 - Mar 13 Mar 7 - Mar 14 December 17, 2019 11 Mar 12 - Mar 19 Mar 13 - Mar 20 Mar 14 - Mar21 December 24, 2019 12 Mar 19 - Mar 26 Mar 20 - Mar 27 Mar 21 - Mar 28 December 31, 2019 13 Mar 26 - Apr 2 Mar 27 - Apr 3 Mar 28 - Apr 4 January 7, 2020 14 April 2 - April 9 April 3 - April 10 April 4 - April 11 January 14, 2020 15 April 9 - April 16 Apr 10 - Apr 17 Apr 11 - Apr 18 January 21, 2020 16 April 16 - April 23 Apr 17 - Apr 24 Apr 18 - Apr 25 January 28, 2020 17 April 23 - April 30 Apr 24 - May 1 Apr 25 - May 2 February 4, 2020 18 Apr 30 - May 7 May 1 - May -
Marriage Valid Dates
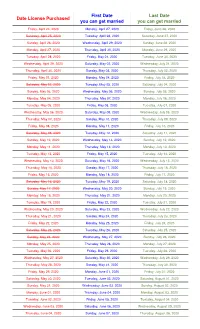
First Date Last Date Date License Purchased you can get married you can get married Friday, April 24, 2020 Monday, April 27, 2020 Friday, June 26, 2020 Saturday, April 25, 2020 Tuesday, April 28, 2020 Saturday, June 27, 2020 Sunday, April 26, 2020 Wednesday, April 29, 2020 Sunday, June 28, 2020 Monday, April 27, 2020 Thursday, April 30, 2020 Monday, June 29, 2020 Tuesday, April 28, 2020 Friday, May 01, 2020 Tuesday, June 30, 2020 Wednesday, April 29, 2020 Saturday, May 02, 2020 Wednesday, July 01, 2020 Thursday, April 30, 2020 Sunday, May 03, 2020 Thursday, July 02, 2020 Friday, May 01, 2020 Monday, May 04, 2020 Friday, July 03, 2020 Saturday, May 02, 2020 Tuesday, May 05, 2020 Saturday, July 04, 2020 Sunday, May 03, 2020 Wednesday, May 06, 2020 Sunday, July 05, 2020 Monday, May 04, 2020 Thursday, May 07, 2020 Monday, July 06, 2020 Tuesday, May 05, 2020 Friday, May 08, 2020 Tuesday, July 07, 2020 Wednesday, May 06, 2020 Saturday, May 09, 2020 Wednesday, July 08, 2020 Thursday, May 07, 2020 Sunday, May 10, 2020 Thursday, July 09, 2020 Friday, May 08, 2020 Monday, May 11, 2020 Friday, July 10, 2020 Saturday, May 09, 2020 Tuesday, May 12, 2020 Saturday, July 11, 2020 Sunday, May 10, 2020 Wednesday, May 13, 2020 Sunday, July 12, 2020 Monday, May 11, 2020 Thursday, May 14, 2020 Monday, July 13, 2020 Tuesday, May 12, 2020 Friday, May 15, 2020 Tuesday, July 14, 2020 Wednesday, May 13, 2020 Saturday, May 16, 2020 Wednesday, July 15, 2020 Thursday, May 14, 2020 Sunday, May 17, 2020 Thursday, July 16, 2020 Friday, May 15, 2020 Monday, May 18, 2020 -

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -
Payroll Calendar 2021
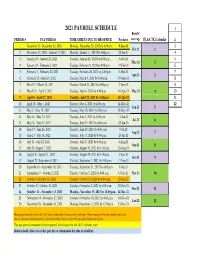
2021 PAYROLL SCHEDULE 1 Benefit PERIOD # PAY PERIOD TIME SHEETS DUE TO HR OFFICE Paydates coverage FLSA 7K Calendar 2 1 December 13- December 26, 2020 Monday, December 28, 2020 by 4:00 p.m. 8-Jan-21 3 Feb-21 1 2 December 27, 2020 - Janurary 9, 2021 Monday, January 11, 2021 by 4:00 p.m. 22-Jan-21 4 3 January 10 - January 23, 2021 Tuesday, January 26, 2021 by 4:00 p.m. 5-Feb-21 5 Mar-21 2 4 January 24 - February 6, 2021 Tuesday, February 9, 2021 by 4:00 p.m. 19-Feb-21 6 5 February 7 - February 20, 2021 Tuesday, February 26, 2021 by 4:00 p.m. 5-Mar-21 7 Apr-21 3 6 February 21 - March 6, 2021 Tuesday, March 9, 2021 by 4:00 p.m. 19-Mar-21 8 7 March 7 - March 20, 2021 Tuesday, March 23, 2021 by 4:00 p.m. 2-Apr-21 9 8 March 21 - April 3, 2021 Tuesday, April 6, 2021 by 4:00 p.m. 16-Apr-21 May-21 4 10 9 April 4 - April 17, 2021 Tuesday, April 20, 2021 by 4:00 p.m. 30-Apr-21 11 10 April 18 - May 1, 2021 Tuesday, May 4, 2021 by 4:00 p.m. 14-May-21 12 Jun-21 5 11 May 2 - May 15, 2021 Tuesday, May 18, 2021 by 4:00 p.m. 28-May-21 12 May 16 - May 29, 2021 Tuesday, June 1, 2021 by 4:00 p.m. 11-Jun-21 Jul-21 6 13 May 30 - June 12, 2021 Tuesday, June 15, 2021 by 4:00 p.m. -

2019-2022 Calendar of Major Jewish Holidays
2019-2022 CALENDAR OF MAJOR JEWISH HOLIDAYS Please note: Jewish students may not be able to participate in school activities that take place on the days marked with an *. 2019 2020 2021 2022 PURIM Celebrates the defeat of the plot to destroy March 21 March 10 February 26 March 17 the Jews of Persia. PASSOVER Deliverance of the Jewish people from Egypt. The first *Eve. of April 19 *Eve. of April 8 *Eve. of March 27 *Eve of April 15 and last two days are observed as full holidays. There are *April 20 *April 9 *March 28 *April 16 dietary restrictions against leavened products (such as *April 21 *April 10 *March 29 *April17 bread, pastries, pasta, certain legumes and more) during *April 26 *April 15 *April 3 *April 21 all eight days of the holiday. *April 27 *April 16 *April 4 *April 22 SHAVUOT *Eve. of June 8 *Eve. of May 28 *Eve. of May 16 *Eve of June 3 Feast of Weeks, marks the giving of the Law (Torah) *June 9 *May 29 *May 17 *June 4 at Mt. Sinai. (Often linked with the Confirmation *June 10 *May 30 *May 18 *June 5 of teenagers.) ROSH HASHANAH *Eve. of Sept. 29 *Eve. of Sept. 18 *Eve. of Sept. 6 *Eve of Sept 25 The Jewish New Year; start of the Ten Days of Penitence. *Sept. 30 *Sept. 19 *Sept. 7 *Sept. 26 The first two days are observed as full holidays. *Oct. 1 *Sept. 20 *Sept. 8 *Sept. 27 YOM KIPPUR Day of Atonement; the most solemn day *Eve. -
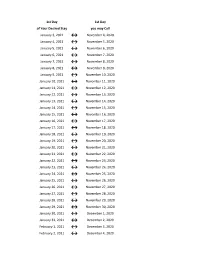
Flex Dates.Xlsx
1st Day 1st Day of Your Desired Stay you may Call January 3, 2021 ↔ November 4, 2020 January 4, 2021 ↔ November 5, 2020 January 5, 2021 ↔ November 6, 2020 January 6, 2021 ↔ November 7, 2020 January 7, 2021 ↔ November 8, 2020 January 8, 2021 ↔ November 9, 2020 January 9, 2021 ↔ November 10, 2020 January 10, 2021 ↔ November 11, 2020 January 11, 2021 ↔ November 12, 2020 January 12, 2021 ↔ November 13, 2020 January 13, 2021 ↔ November 14, 2020 January 14, 2021 ↔ November 15, 2020 January 15, 2021 ↔ November 16, 2020 January 16, 2021 ↔ November 17, 2020 January 17, 2021 ↔ November 18, 2020 January 18, 2021 ↔ November 19, 2020 January 19, 2021 ↔ November 20, 2020 January 20, 2021 ↔ November 21, 2020 January 21, 2021 ↔ November 22, 2020 January 22, 2021 ↔ November 23, 2020 January 23, 2021 ↔ November 24, 2020 January 24, 2021 ↔ November 25, 2020 January 25, 2021 ↔ November 26, 2020 January 26, 2021 ↔ November 27, 2020 January 27, 2021 ↔ November 28, 2020 January 28, 2021 ↔ November 29, 2020 January 29, 2021 ↔ November 30, 2020 January 30, 2021 ↔ December 1, 2020 January 31, 2021 ↔ December 2, 2020 February 1, 2021 ↔ December 3, 2020 February 2, 2021 ↔ December 4, 2020 1st Day 1st Day of Your Desired Stay you may Call February 3, 2021 ↔ December 5, 2020 February 4, 2021 ↔ December 6, 2020 February 5, 2021 ↔ December 7, 2020 February 6, 2021 ↔ December 8, 2020 February 7, 2021 ↔ December 9, 2020 February 8, 2021 ↔ December 10, 2020 February 9, 2021 ↔ December 11, 2020 February 10, 2021 ↔ December 12, 2020 February 11, 2021 ↔ December 13, 2020 -

2020-2021 Academic Calendar Revised 9.18.20
FRANCISCAN UNIVERSITY OF STEUBENVILLE 2020-2021 ACADEMIC CALENDAR REVISED 9.18.20 FALL 2020 SEMESTER SPRING 2021 SEMESTER August 24 25-December 11 January 11-May 5 New Student Orientation August 20-23 (Thurs-Sun) January 7-10 (Thurs-Sun) Convocation & Opening of School Mass August 24 (Mon) (4 pm; 3 pm classes January 11 (Mon) (mass only, 10:30 am) shortened & 4:30 pm classes cancelled) Classes begin August 24 (Mon) January 11 (Mon) (10 a.m. classes shortened) Last day for late registration August 28 (Fri) January 15 (Fri) Last day for adding/dropping courses September 2 (Wed) January 20 (Wed) Labor Day (class day) September 7 (Mon) (class day) N/A March for Life N/A January 29 (no day classes) Last day for audit changes September 11 (Fri) January 22 (Fri) Incomplete grades due to registrar September 25 (Fri) February 12 (Fri) Feast of St. Francis October 4 (Sun) N/A Homecoming weekend October 2-4 (Fri-Sun) N/A Midterm deficiencies due to registrar October 14 (Wed) March 5 (Fri) Spring Break N/A March 8-12 (Mon-Fri) (classes resume Mon, March 15) Last day for course withdrawal November 2 (Mon) March 26 (Fri) Tentative Class Make-up Days November 14, 21 (Sat) Thanksgiving vacation November 25-29 (Wed-Sun) N/A (classes resume Mon, Nov 30) Holy Thursday April 1 (no evening classes) Easter recess (Friday & Monday day classes N/A April 2-April 5 (day) canceled; *Monday evening classes do meet) (classes resume Mon evening, April 5, Tuesday day, April 6) Classes Resume Evening: Mon, April 5; Day: Tues, April 6 Last day of classes December 1 (Tues) -

Pay Week Begin: Saturdays Pay Week End: Fridays Check Date
Pay Week Begin: Pay Week End: Due to UCP no later Check Date: Saturdays Fridays than Monday 7:30am week 1 December 10, 2016 December 16, 2016 December 19, 2016 December 30, 2016 week 2 December 17, 2016 December 23, 2016 December 26, 2016 week 1 December 24, 2016 December 30, 2016 January 2, 2017 January 13, 2017 week 2 December 31, 2016 January 6, 2017 January 9, 2017 week 1 January 7, 2017 January 13, 2017 January 16, 2017 January 27, 2017 week 2 January 14, 2017 January 20, 2017 January 23, 2017 January 21, 2017 January 27, 2017 week 1 January 30, 2017 February 10, 2017 week 2 January 28, 2017 February 3, 2017 February 6, 2017 week 1 February 4, 2017 February 10, 2017 February 13, 2017 February 24, 2017 week 2 February 11, 2017 February 17, 2017 February 20, 2017 March 3, 2017 week 1 February 18, 2017 February 24, 2017 February 27, 2017 ***1 Week Pay Period Transition*** week 1 February 25, 2017 March 3, 2017 March 6, 2017 March 17, 2017 week 2 March 4, 2017 March 10, 2017 March 13, 2017 week 1 March 11, 2017 March 17, 2017 March 20, 2017 March 31, 2017 week 2 March 18, 2017 March 24, 2017 March 27, 2017 week 1 March 25, 2017 March 31, 2017 April 3, 2017 April 14, 2017 week 2 April 1, 2017 April 7, 2017 April 10, 2017 week 1 April 8, 2017 April 14, 2017 April 17, 2017 April 28, 2017 week 2 April 15, 2017 April 21, 2017 April 24, 2017 week 1 April 22, 2017 April 28, 2017 May 1, 2017 May 12, 2017 week 2 April 29, 2017 May 5, 2017 May 8, 2017 week 1 May 6, 2017 May 12, 2017 May 15, 2017 May 26, 2017 week 2 May 13, 2017 May 19, 2017 May -

60-Day Calendar Timeline Chart
60-DAY CALENDAR TIMELINE CHART Assessments to be conducted and IEP meetings to be held within 60 days of the Request for Assessment being signed. (Calendar does not reflect school breaks for holidays.) JAN FEB FEB MAR MAR APR APR MAY MAY JULY Jan 1 = Mar 2 Feb 7 = Apr 8 Mar 15 = May 14 Apr 21 = Jun 20 May 28 = Jul 27 Jan 2 = Mar 3 Feb 8 = Apr 9 Mar 16 = May 15 Apr 22 = Jun 21 May 29 = Jul 28 Jan 3 = Mar 4 Feb 9 = Apr 10 Mar 17 = May 16 Apr 23 = Jun 22 May 30 = Jul 29 Jan 4 = Mar 5 Feb 10 = Apr 11 Mar 18 = May 17 Apr 24 = Jun 23 May 31 = Jul 30 Jan 5 = Mar 6 Feb 11 = Apr 12 Mar 19 = May 18 Apr 25 = Jun 24 Jun 1 = Jul 31 Jan 6 = Mar 7 Feb 12 = Apr 13 Mar 20 = May 19 Apr 26 = Jun 25 Jun 2 = Aug 1 Jan 7 = Mar 8 Feb 13 = Apr 14 Mar 21 = May 20 Apr 27 = Jun 26 Jun 3 = Aug 2 Jan 8 = Mar 9 Feb 14 = Apr 15 Mar 22 = May 21 Apr 28 = Jun 27 Jun 4 = Aug 3 Jan 9 = Mar 10 Feb 15 = Apr 16 Mar 23 = May 22 Apr 29 = Jun 28 Jun 5 = Aug 4 Jan 10 = Mar 11 Feb 16 = Apr 17 Mar 24 = May 23 Apr 30 = Jun 29 Jun 6 = Aug 5 Jan 11 = Mar 12 Feb 17 = Apr 18 Mar 25 = May 24 May 1 = Jun 30 Jun 7 = Aug 6 Jan 12 = Mar 13 Feb 18 = Apr 19 Mar 26 = May 25 May 2 = Jul 1 Jun 8 = Aug 7 Jan 13 = Mar 14 Feb 19 = Apr 20 Mar 27 = May 26 May 3 = Jul 2 Jun 9 = Aug 8 Jan 14 = Mar 15 Feb 20 = Apr 21 Mar 28 = May 27 May 4 = Jul 3 Jun 10 = Aug 9 Jan 15 = Mar 16 Feb 21 = Apr 22 Mar 29 = May 28 May 5 = Jul 4 Jun 11 = Aug 10 Jan 16 = Mar 17 Feb 22 = Apr 23 Mar 30 = May 29 May 6 = Jul 5 Jun 12 = Aug 11 Jan 17 = Mar 18 Feb 23 = Apr 24 Mar 31 = May 30 May 7 = Jul 6 Jun 13 = Aug 12 Jan 18 = Mar