COVID-19 Shuts Doors to Flu but Keeps Them Open to Rhinoviruses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Positive Rhinovirus/Enterovirus Detection and SARS-Cov-2 Persistence Beyond the Acute Infection Phase: an Intra-Household Surveillance Study
viruses Communication The Positive Rhinovirus/Enterovirus Detection and SARS-CoV-2 Persistence beyond the Acute Infection Phase: An Intra-Household Surveillance Study Pedro Brotons 1,2,3, Iolanda Jordan 1,3,4, Quique Bassat 3,5,6,7,8 , Desiree Henares 1,3, Mariona Fernandez de Sevilla 1,3,5, Sara Ajanovic 7, Alba Redin 1,2, Vicky Fumado 1,5, Barbara Baro 7 , Joana Claverol 9, Rosauro Varo 7 , Daniel Cuadras 9 , Jochen Hecht 10, Irene Barrabeig 3,11, Juan Jose Garcia-Garcia 1,3,5, Cristian Launes 1,3,5,† and Carmen Muñoz-Almagro 1,2,3,12,*,† 1 Pediatric Infectious Diseases Research Group, Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, 08950 Barcelona, Spain; [email protected] (P.B.); [email protected] (I.J.); [email protected] (D.H.); [email protected] (M.F.d.S.); [email protected] (A.R.); [email protected] (V.F.); [email protected] (J.J.G.-G.); [email protected] (C.L.) 2 Department of Medicine, School of Medicine, Universitat Internacional de Catalunya, Sant Cugat, 08195 Barcelona, Spain 3 Consorcio de Investigacion Biomédica en Red Epidemiologia y Salud Pública (CIBERESP), 28029 Madrid, Spain; [email protected] (Q.B.); [email protected] (I.B.) 4 Pediatric Intensive Care Unit, Hospital Sant Joan de Déu, Esplugues de Llobregat, 08950 Barcelona, Spain 5 Pediatrics Department, Hospital Sant Joan de Déu, Esplugues de Llobregat, 08950 Barcelona, Spain 6 Centro de Investigação em Saúde de Manhiça (CISM), Manhiça 1929, Mozambique Citation: Brotons, P.; Jordan, I.; 7 ISGlobal, Hospital Clínic-Universitat de Barcelona, 08036 Barcelona, Spain; [email protected] (S.A.); Bassat, Q.; Henares, D.; Fernandez de [email protected] (B.B.); [email protected] (R.V.) Sevilla, M.; Ajanovic, S.; Redin, A.; 8 Institució Catalana de Recerca i Estudis Avançats (ICREA), 08010 Barcelona, Spain Fumado, V.; Baro, B.; Claverol, J.; et al. -

Equine Rotavirus Strain Arg/E706/2008 VP7 (VP7) Gene, Partial Cds Genbank: GU373939.1 FASTA Graphics Popset
Equine rotavirus strain Arg/E706/2008 VP7 (VP7) gene, partial cds GenBank: GU373939.1 FASTA Graphics PopSet Go to: LOCUS GU373939 972 bp RNA linear VRL 25-JUL-2016 DEFINITION Equine rotavirus strain Arg/E706/2008 VP7 (VP7) gene, partial cds. ACCESSION GU373939 VERSION GU373939.1 KEYWORDS . SOURCE Equine rotavirus ORGANISM Equine rotavirus Viruses; Riboviria; Orthornavirae; Duplornaviricota; Resentoviricetes; Reovirales; Reoviridae; Sedoreovirinae; Rotavirus; unclassified Rotavirus. REFERENCE 1 (bases 1 to 972) AUTHORS Garaicoechea,L., Mino,S.O., Barrandeguy,M. and Parreno,V. TITLE Molecular Characterization of Equine rotavirus Circulating in Sport Horses of Argentina During a 17-year Period (1992-2008) JOURNAL Unpublished REFERENCE 2 (bases 1 to 972) AUTHORS Garaicoechea,L., Mino,S.O., Barrandeguy,M. and Parreno,V. TITLE Direct Submission JOURNAL Submitted (29-DEC-2009) Virology Institute, INTA, Dr Nicolas Repetto y de Los Reseros s/n, Castelar, Buenos Aires 1712, ArgentinaFEATURES Location/Qualifiers source 1..972 /organism="Equine rotavirus" /mol_type="genomic RNA" /strain="Arg/E706/2008" /isolation_source="fecal sample" /host="equine" /db_xref="taxon:10937" /country="Argentina: Buenos Aires" /collection_date="2008" /note="genotype: G14" gene 7..>972 /gene="VP7" CDS 7..>972 /gene="VP7" /codon_start=1 /product="VP7" /protein_id="AEF33475.1" /translation="MYGIEYTTILTFLISLILLNYILQLLTRIMDFIIYRFLLIIVLL SPFLNAQNYGINLPITGSMDTAYVNSTQENIFLTSTLCLYYPTEAATQIDDSSWKDTI SQLFLTKGWPTGSVYLKEYTDIASFSIDPQLYCDYNVVLMKYDEALQLDMSELADLIL NEWLCNPMDITLYYYQQTDEANKWISMGSSCTIKVCPLNTQTLGIGCLTTNVATFEEV -

Global Distribution of Novel Rhinovirus Genotype
DISPATCHES in resource-poor regions (1). Streptococcus pneumoniae Global Distribution and Haemophilus infl uenzae are important bacterial causes of ARI, although their impact is expected to decline with of Novel Rhinovirus increasing vaccine coverage. Collectively, however, virus- es dominate as causative agents in ARI. Viruses frequently Genotype implicated in ARI include infl uenza virus, respiratory syn- Thomas Briese,* Neil Renwick,* Marietjie Venter,† cytial virus, metapneumovirus, parainfl uenza virus, human Richard G. Jarman,‡ Dhrubaa Ghosh,§ enterovirus (HEV), and human rhinovirus (HRV). Sophie Köndgen,¶ Sanjaya K. Shrestha,# HRVs are grouped taxonomically into Human rhinovi- A. Mette Hoegh,** Inmaculada Casas,†† Edgard rus A (HRV-A) and Human rhinovirus B (HRV-B), 2 spe- Valerie Adjogoua,‡‡ cies within the family Picornaviridae (International Com- Chantal Akoua-Koffi ,‡‡ Khin Saw Myint,‡ David T. mittee on Taxonomy of Viruses database [ICTVdb]; http:// Williams,§§ Glenys Chidlow,¶¶ phene.cpmc.columbia.edu). These nonenveloped, positive- Ria van den Berg,† Cristina Calvo,## sense, single-stranded RNA viruses have been classifi ed se- Orienka Koch,† Gustavo Palacios,* rologically and on the basis of antiviral susceptibility pro- Vishal Kapoor,* Joseph Villari,* fi le, nucleotide sequence relatedness, and receptor usage (2). Samuel R. Dominguez,*** Kathryn V. Holmes,*** Phylogenetic analyses of viral protein VP4/VP2 and VP1 Gerry Harnett,¶¶ David Smith,¶¶ coding regions indicate the presence of 74 serotypes in ge- John S. Mackenzie,§§ Heinz Ellerbrok,¶ netic group A and 25 serotypes in genetic group B (2). Brunhilde Schweiger,¶ Kristian Schønning,** Isolated in the 1950s from persons with upper respi- Mandeep S. Chadha,§ Fabian H. Leendertz,¶ A.C. ratory tract symptoms (2,3), HRVs have become known Mishra,§ Robert V. -

Atomic Structure of a Rhinovirus C, a Virus Species Linked to Severe
Atomic structure of a rhinovirus C, a virus species SEE COMMENTARY linked to severe childhood asthma Yue Liua, Marchel G. Hillb, Thomas Klosea, Zhenguo Chena, Kelly Wattersb, Yury A. Bochkovc, Wen Jianga, Ann C. Palmenbergb,1, and Michael G. Rossmanna,1 aDepartment of Biological Sciences, Purdue University, West Lafayette, IN 47907; bInstitute for Molecular Virology, University of Wisconsin, Madison, WI 53706; and cDepartment of Pediatrics, School of Medicine and Public Health, University of Wisconsin, Madison, WI 53706 Edited by Peter Palese, Icahn School of Medicine at Mount Sinai, New York, NY, and approved June 7, 2016 (received for review April 25, 2016) Isolates of rhinovirus C (RV-C), a recently identified Enterovirus Picornavirus capsids are assembled from 60 copies of biolog- (EV) species, are the causative agents of severe respiratory infec- ical protomers, each composed of four proteins: VP1, VP2, VP3, tions among children and are linked to childhood asthma exacer- and VP4 (2). The three large surface polypeptides, VP1, VP2, bations. The RV-C have been refractory to structure determination and VP3, are folded into eight-stranded antiparallel “jelly rolls.” because they are difficult to propagate in vitro. Here, we report During the assembly process, autocatalytic cleavage of precursor the cryo-EM atomic structures of the full virion and native empty VP0 into VP2 and VP4 in the presence of viral RNA results in particle (NEP) of RV-C15a. The virus has 60 “fingers” on the virus the formation of full infectious virions (20). The arrangement of outer surface that probably function as dominant immunogens. jelly rolls in the virions exhibits pseudo T = 3 icosahedral sym- Because the NEPs also display these fingers, they may have utility metry with an outer diameter of ∼300 Å (2, 3). -

2020 Taxonomic Update for Phylum Negarnaviricota (Riboviria: Orthornavirae), Including the Large Orders Bunyavirales and Mononegavirales
Archives of Virology https://doi.org/10.1007/s00705-020-04731-2 VIROLOGY DIVISION NEWS 2020 taxonomic update for phylum Negarnaviricota (Riboviria: Orthornavirae), including the large orders Bunyavirales and Mononegavirales Jens H. Kuhn1 · Scott Adkins2 · Daniela Alioto3 · Sergey V. Alkhovsky4 · Gaya K. Amarasinghe5 · Simon J. Anthony6,7 · Tatjana Avšič‑Županc8 · María A. Ayllón9,10 · Justin Bahl11 · Anne Balkema‑Buschmann12 · Matthew J. Ballinger13 · Tomáš Bartonička14 · Christopher Basler15 · Sina Bavari16 · Martin Beer17 · Dennis A. Bente18 · Éric Bergeron19 · Brian H. Bird20 · Carol Blair21 · Kim R. Blasdell22 · Steven B. Bradfute23 · Rachel Breyta24 · Thomas Briese25 · Paul A. Brown26 · Ursula J. Buchholz27 · Michael J. Buchmeier28 · Alexander Bukreyev18,29 · Felicity Burt30 · Nihal Buzkan31 · Charles H. Calisher32 · Mengji Cao33,34 · Inmaculada Casas35 · John Chamberlain36 · Kartik Chandran37 · Rémi N. Charrel38 · Biao Chen39 · Michela Chiumenti40 · Il‑Ryong Choi41 · J. Christopher S. Clegg42 · Ian Crozier43 · John V. da Graça44 · Elena Dal Bó45 · Alberto M. R. Dávila46 · Juan Carlos de la Torre47 · Xavier de Lamballerie38 · Rik L. de Swart48 · Patrick L. Di Bello49 · Nicholas Di Paola50 · Francesco Di Serio40 · Ralf G. Dietzgen51 · Michele Digiaro52 · Valerian V. Dolja53 · Olga Dolnik54 · Michael A. Drebot55 · Jan Felix Drexler56 · Ralf Dürrwald57 · Lucie Dufkova58 · William G. Dundon59 · W. Paul Duprex60 · John M. Dye50 · Andrew J. Easton61 · Hideki Ebihara62 · Toufc Elbeaino63 · Koray Ergünay64 · Jorlan Fernandes195 · Anthony R. Fooks65 · Pierre B. H. Formenty66 · Leonie F. Forth17 · Ron A. M. Fouchier48 · Juliana Freitas‑Astúa67 · Selma Gago‑Zachert68,69 · George Fú Gāo70 · María Laura García71 · Adolfo García‑Sastre72 · Aura R. Garrison50 · Aiah Gbakima73 · Tracey Goldstein74 · Jean‑Paul J. Gonzalez75,76 · Anthony Grifths77 · Martin H. Groschup12 · Stephan Günther78 · Alexandro Guterres195 · Roy A. -

Understanding Human Astrovirus from Pathogenesis to Treatment
University of Tennessee Health Science Center UTHSC Digital Commons Theses and Dissertations (ETD) College of Graduate Health Sciences 6-2020 Understanding Human Astrovirus from Pathogenesis to Treatment Virginia Hargest University of Tennessee Health Science Center Follow this and additional works at: https://dc.uthsc.edu/dissertations Part of the Diseases Commons, Medical Sciences Commons, and the Viruses Commons Recommended Citation Hargest, Virginia (0000-0003-3883-1232), "Understanding Human Astrovirus from Pathogenesis to Treatment" (2020). Theses and Dissertations (ETD). Paper 523. http://dx.doi.org/10.21007/ etd.cghs.2020.0507. This Dissertation is brought to you for free and open access by the College of Graduate Health Sciences at UTHSC Digital Commons. It has been accepted for inclusion in Theses and Dissertations (ETD) by an authorized administrator of UTHSC Digital Commons. For more information, please contact [email protected]. Understanding Human Astrovirus from Pathogenesis to Treatment Abstract While human astroviruses (HAstV) were discovered nearly 45 years ago, these small positive-sense RNA viruses remain critically understudied. These studies provide fundamental new research on astrovirus pathogenesis and disruption of the gut epithelium by induction of epithelial-mesenchymal transition (EMT) following astrovirus infection. Here we characterize HAstV-induced EMT as an upregulation of SNAI1 and VIM with a down regulation of CDH1 and OCLN, loss of cell-cell junctions most notably at 18 hours post-infection (hpi), and loss of cellular polarity by 24 hpi. While active transforming growth factor- (TGF-) increases during HAstV infection, inhibition of TGF- signaling does not hinder EMT induction. However, HAstV-induced EMT does require active viral replication. -

Article Download (79)
wjpls, 2020, Vol. 6, Issue 6, 152-161 Review Article ISSN 2454-2229 Pratik et al. World Journal of Pharmaceutical World Journaland Life of Pharmaceutica Sciencesl and Life Science WJPLS www.wjpls.org SJIF Impact Factor: 6.129 THE NOVEL CORONAVIRUS (COVID-19) CAUSATIVE AGENT FOR HUMAN RESPIRATORY DISEASES Pratik V. Malvade1*, Rutik V. Malvade2, Shubham P. Varpe3 and Prathamesh B. Kadu3 1Pravara Rural College of Pharmacy, Pravaranagar, 413736, Dist. - Ahmednagar (M.S.) India. 2Pravara Rural Engineering College, Loni, 413736, Dist. - Ahmednagar (M.S.) India. 3Ashvin College Of Pharmacy, Manchi Hill, Ashvi Bk., 413714, Dist.- Ahmednagar (M.S.) India. *Corresponding Author: Pratik V. Malvade Pravara Rural College of Pharmacy, Pravaranagar, 413736, Dist. - Ahmednagar (M.S.) India. Article Received on 08/04/2020 Article Revised on 29/04/2020 Article Accepted on 19/05/2020 ABSTRACT The newly founded human coronavirus has named as Covid-19. The full form of Covid-19 is “Co-Corona, vi- virus and d- disease”. The Covid-19 is also named as 2019-nCoV because of it was firstly identified at the end of 2019. The coronavirus are the group of various types of viruses i.e. some have positive-sense, single stranded RNA and they are covered within the envelope made up of protein. Still now days seven human coronaviruses are identified are Nl 63, 229E, OC43, HKU1, SARS-CoV, MERS-CoV and latest Covid-19 also known as SARS-CoV-2. From above all, the SARS-CoV and MERS-CoV causes the highest outbreak but the outbreak of Covid-19 is much more than the other any virus. -
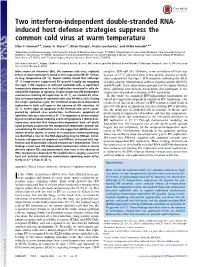
Two Interferon-Independent Double-Stranded RNA-Induced Host
Two interferon-independent double-stranded RNA- induced host defense strategies suppress the common cold virus at warm temperature Ellen F. Foxmana,b, James A. Storera,1, Kiran Vanajac, Andre Levchenkoc, and Akiko Iwasakia,d,2 aDepartment of Immunobiology, Yale University School of Medicine, New Haven, CT 06520; bDepartment of Laboratory Medicine, Yale University School of Medicine, New Haven, CT 06520; cDepartment of Biomedical Engineering, Systems Biology Institute, Yale University, Yale University School of Medicine, New Haven, CT 06520; and dHoward Hughes Medical Institute, New Haven, CT 06520 Edited by Jonathan C. Kagan, Children’s Hospital Boston, Boston, MA, and accepted by Editorial Board Member Tadatsugu Taniguchi June 6, 2016 (received for review February 4, 2016) Most strains of rhinovirus (RV), the common cold virus, replicate receptor, IFN-αβR (4). However, some restriction of viral rep- better at cool temperatures found in the nasal cavity (33–35 °C) than lication at 37 °C persisted even in the genetic absence of mole- at lung temperature (37 °C). Recent studies found that although cules required for the type 1 IFN response, including the RLR 37 °C temperature suppressed RV growth largely by engaging signaling adaptor, mitochondrial antiviral signaling protein (MAVS), the type 1 IFN response in infected epithelial cells, a significant and IFN-αβR. These observations promptedustoexplorewhether temperature dependence to viral replication remained in cells de- other additional host defense mechanisms also participate in the void of IFN induction or signaling. To gain insight into IFN-independent temperature-dependent restriction of RV replication. mechanisms limiting RV replication at 37 °C, we studied RV infec- In this study, we examined IFN-independent mechanisms in- tion in human bronchial epithelial cells and H1-HeLa cells. -

Astrovirus MLB2, a New Gastroenteric Virus Associated with Meningitis and Disseminated Infection Samuel Cordey,1 Diem-Lan Vu,1 Manuel Schibler, Arnaud G
RESEARCH Astrovirus MLB2, a New Gastroenteric Virus Associated with Meningitis and Disseminated Infection Samuel Cordey,1 Diem-Lan Vu,1 Manuel Schibler, Arnaud G. L’Huillier, Francisco Brito, Mylène Docquier, Klara M. Posfay-Barbe, Thomas J. Petty, Lara Turin, Evgeny M. Zdobnov, Laurent Kaiser Next-generation sequencing has identified novel astrovi- observed in community healthcare centers (2,3). Symp- ruses for which a pathogenic role is not clearly defined. toms are generally mild, with patient hospitalization We identified astrovirus MLB2 infection in an immunocom- usually not required; asymptomatic carriage has been petent case-patient and an immunocompromised patient described in 2% of children (4). who experienced diverse clinical manifestations, notably, Screening of fecal samples from persons with diarrhea meningitis and disseminated infection. The initial case-pa- and control samples in different parts of the world by un- tient was identified by next-generation sequencing, which revealed astrovirus MLB2 RNA in cerebrospinal fluid, biased next-generation sequencing (NGS) or reverse tran- plasma, urine, and anal swab specimens. We then used scription PCR (RT-PCR) has revealed the sporadic pres- specific real-time reverse transcription PCR to screen 943 ence of members of the Astroviridae family, previously fecal and 424 cerebrospinal fluid samples from hospital- unrecognized in humans, that are phylogenetically substan- ized patients and identified a second case of meningitis, tially distant from classic HAstVs (3,5–9). These viruses with positive results for the agent in the patient’s feces have been named HAstV-VA/HMO and HAstV-MLB, for and plasma. This screening revealed 5 additional positive Virginia, human-mink-ovine, and Melbourne, respectively, fecal samples: 1 from an infant with acute diarrhea and according to the place where they were first identified and 4 from children who had received transplants. -
Latest Ncbi-Taxonomist Docker Image Can Be Pulled from Registry.Gitlab.Com/Janpb/ Ncbi-Taxonomist:Latest
ncbi-taxonomist Documentation Release 1.2.1+8580b9b Jan P Buchmann 2020-11-15 Contents: 1 Installation 3 2 Basic functions 5 3 Cookbook 35 4 Container 39 5 Frequently Asked Questions 49 6 Module references 51 7 Synopsis 63 8 Requirements and Dependencies 65 9 Contact 67 10 Indices and tables 69 Python Module Index 71 Index 73 i ii ncbi-taxonomist Documentation, Release 1.2.1+8580b9b 1.2.1+8580b9b :: 2020-11-15 Contents: 1 ncbi-taxonomist Documentation, Release 1.2.1+8580b9b 2 Contents: CHAPTER 1 Installation Content • Local pip install (no root required) • Global pip install (root required) ncbi-taxonomist is available on PyPi via pip. If you use another Python package manager than pip, please consult its documentation. If you are installing ncbi-taxonomist on a non-Linux system, consider the propsed methods as guidelines and adjust as required. Important: Please note If some of the proposed commands are unfamiliar to you, don’t just invoke them but look them up, e.g. in man pages or search online. Should you be unfamiliar with pip, check pip -h Note: Python 3 vs. Python 2 Due to co-existing Python 2 and Python 3, some installation commands may be invoked slighty different. In addition, development and support for Python 2 did stop January 2020 and should not be used anymore. ncbi-taxonomist requires Python >= 3.8. Depending on your OS and/or distribution, the default pip command can install either Python 2 or Python 3 packages. Make sure you use pip for Python 3, e.g. -

Cold and Flu Fact Sheet
Cold and Flu Fact Sheet The common cold, including chest colds, head colds, and the seasonal flu are caused by viruses that can put a damper on your holiday spirit. While Cold and Flu season can start as early as October and can last as late as May, activity peaks during Christmas time and will want to make you say Bah-Humbug! General Information Virology Clinical manifestations Cold - The common cold is a viral infection of the upper Cold - Symptoms of a common cold usually appear about respiratory tract. The most commonly implicated virus is a one to three days after exposure to a cold-causing virus. rhinovirus. Other commonly implicated viruses include Signs and symptoms typically include a runny/stuffy nose, human coronavirus, influenza viruses, and adenovirus. itchy/sore throat, cough, congestion, slight body aches and Frequently, more than one virus is present. The difficultly mild headache, sneezing, water eyes, and mild fatigue. with pathogens associated with the common cold is that some viruses are enveloped, meaning they are easy to kill Flu - Symptoms of seasonal influenza are very similar to (such as influenza) while others are non-enveloped, those of the common cold, except the flu can be meaning they are harder to kill (such as rhinovirus). This distinguished by a high fever and more severe symptoms emphasizes the importance of choosing disinfectant of the common cold. products with the ability to kill both enveloped and non- enveloped viruses. Pandemics and Outbreaks A pandemic is a global disease outbreak. It is determined Flu - Influenza (commonly known as the flu) are influenza by how the disease spreads, not by how many deaths it viruses which are enveloped, RNA viruses that make up causes. -

Avian Orthoreovirus Segment S4, Complete Genome NCBI Reference Sequence: NC 015135.1
Avian orthoreovirus segment S4, complete genome NCBI Reference Sequence: NC_015135.1 FASTA Graphics Go to: LOCUS NC_015135 1192 bp RNA linear VRL 13-AUG-2018 DEFINITION Avian orthoreovirus segment S4, complete genome. ACCESSION NC_015135 VERSION NC_015135.1 DBLINK BioProject: PRJNA485481 KEYWORDS RefSeq. SOURCE Avian orthoreovirus ORGANISM Avian orthoreovirus Viruses; Riboviria; Orthornavirae; Duplornaviricota; Resentoviricetes; Reovirales; Reoviridae; Spinareovirinae; Orthoreovirus. REFERENCE 1 AUTHORS Banyai,K., Dandar,E., Dorsey,K.M., Mato,T. and Palya,V. TITLE The genomic constellation of a novel avian orthoreovirus strain associated with runting-stunting syndrome in broilers JOURNAL Virus Genes 42 (1), 82-89 (2011) PUBMED 21116842 REFERENCE 2 (bases 1 to 1192) CONSRTM NCBI Genome Project TITLE Direct Submission JOURNAL Submitted (11-FEB-2011) National Center for Biotechnology Information, NIH, Bethesda, MD 20894, USA REFERENCE 3 (bases 1 to 1192) AUTHORS Banyai,K. TITLE Direct Submission JOURNAL Submitted (29-SEP-2010) Banyai K., Hungarian Academy of Sciences, Veterinary Medical Research Institute, Hungaria krt. 21., Budapest, H-1143, HUNGARY COMMENT PROVISIONAL REFSEQ: This record has not yet been subject to final NCBI review. The reference sequence is identical to FR694200. COMPLETENESS: full length. FEATURES Location/Qualifiers source 1..1192 /organism="Avian orthoreovirus" /mol_type="genomic RNA" /strain="AVS-B" /db_xref="taxon:38170" /segment="S4" /country="USA" gene 24..1127 /gene="sigma-NS" /locus_tag="AOrVsS4_gpp1" /db_xref="GeneID:10220435"