Exploiting Oncogenic Drivers Along the CCNG1 Pathway for Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chromosomal Aberrations in Head and Neck Squamous Cell Carcinomas in Norwegian and Sudanese Populations by Array Comparative Genomic Hybridization
825-843 12/9/08 15:31 Page 825 ONCOLOGY REPORTS 20: 825-843, 2008 825 Chromosomal aberrations in head and neck squamous cell carcinomas in Norwegian and Sudanese populations by array comparative genomic hybridization ERIC ROMAN1,2, LEONARDO A. MEZA-ZEPEDA3, STINE H. KRESSE3, OLA MYKLEBOST3,4, ENDRE N. VASSTRAND2 and SALAH O. IBRAHIM1,2 1Department of Biomedicine, Faculty of Medicine and Dentistry, University of Bergen, Jonas Lies vei 91; 2Department of Oral Sciences - Periodontology, Faculty of Medicine and Dentistry, University of Bergen, Årstadveien 17, 5009 Bergen; 3Department of Tumor Biology, Institute for Cancer Research, Rikshospitalet-Radiumhospitalet Medical Center, Montebello, 0310 Oslo; 4Department of Molecular Biosciences, University of Oslo, Blindernveien 31, 0371 Oslo, Norway Received January 30, 2008; Accepted April 29, 2008 DOI: 10.3892/or_00000080 Abstract. We used microarray-based comparative genomic logical parameters showed little correlation, suggesting an hybridization to explore genome-wide profiles of chromosomal occurrence of gains/losses regardless of ethnic differences and aberrations in 26 samples of head and neck cancers compared clinicopathological status between the patients from the two to their pair-wise normal controls. The samples were obtained countries. Our findings indicate the existence of common from Sudanese (n=11) and Norwegian (n=15) patients. The gene-specific amplifications/deletions in these tumors, findings were correlated with clinicopathological variables. regardless of the source of the samples or attributed We identified the amplification of 41 common chromosomal carcinogenic risk factors. regions (harboring 149 candidate genes) and the deletion of 22 (28 candidate genes). Predominant chromosomal alterations Introduction that were observed included high-level amplification at 1q21 (harboring the S100A gene family) and 11q22 (including Head and neck squamous cell carcinoma (HNSCC), including several MMP family members). -

Genome-Wide Approach to Identify Risk Factors for Therapy-Related Myeloid Leukemia
Leukemia (2006) 20, 239–246 & 2006 Nature Publishing Group All rights reserved 0887-6924/06 $30.00 www.nature.com/leu ORIGINAL ARTICLE Genome-wide approach to identify risk factors for therapy-related myeloid leukemia A Bogni1, C Cheng2, W Liu2, W Yang1, J Pfeffer1, S Mukatira3, D French1, JR Downing4, C-H Pui4,5,6 and MV Relling1,6 1Department of Pharmaceutical Sciences, The University of Tennessee, Memphis, TN, USA; 2Department of Biostatistics, The University of Tennessee, Memphis, TN, USA; 3Hartwell Center, The University of Tennessee, Memphis, TN, USA; 4Department of Pathology, The University of Tennessee, Memphis, TN, USA; 5Department of Hematology/Oncology St Jude Children’s Research Hospital, The University of Tennessee, Memphis, TN, USA; and 6Colleges of Medicine and Pharmacy, The University of Tennessee, Memphis, TN, USA Using a target gene approach, only a few host genetic risk therapy increases, the importance of identifying host factors for factors for treatment-related myeloid leukemia (t-ML) have been secondary neoplasms increases. defined. Gene expression microarrays allow for a more 4 genome-wide approach to assess possible genetic risk factors Because DNA microarrays interrogate multiple ( 10 000) for t-ML. We assessed gene expression profiles (n ¼ 12 625 genes in one experiment, they allow for a ‘genome-wide’ probe sets) in diagnostic acute lymphoblastic leukemic cells assessment of genes that may predispose to leukemogenesis. from 228 children treated on protocols that included leukemo- DNA microarray analysis of gene expression has been used to genic agents such as etoposide, 13 of whom developed t-ML. identify distinct expression profiles that are characteristic of Expression of 68 probes, corresponding to 63 genes, was different leukemia subtypes.13,14 Studies using this method have significantly related to risk of t-ML. -

IGH Rearrangement in Myeloid Neoplasms Sion and Activation
CASE REPORTS genes such as MYC and BCL2, leading to their overexpres- IGH rearrangement in myeloid neoplasms sion and activation. Here, we found two IGH rearrange- ments in myeloid tumors, including an IGH-MECOM in a Though immunoglobulin genes are typically expressed myelodysplastic syndrome (MDS) and an IGH-CCNG1 in in B lymphocytes, recent studies found ectopic an AML. Our studies provide the first evidence that a once immunoglobulin expression in non-B-cell tumor cells believed B-cell tumor-specific oncogenic mechanism is including acute myeloid leukemia (AML). The also present in myeloid tumors. immunoglobulin genes, including immunoglobulin heavy Case #1: A 60-year-old female with a history of breast chain genes (IGH), light kappa (k) chain genes (IGK) and cancer presented with fatigue, bilateral flank pain, and 9 light lambda (λ) chain genes (IGL), are frequently hematuria. Complete blood count showed 24.82x10 /L of rearranged in B-cell tumors. These rearrangements result white blood cells, 11.2 g/dL of hemoglobin, 33.9% of in a juxtaposition of IG enhancers to the vicinity of onco- hematocrit, and 68x109/L of platelets. The bone marrow A B C D E Figure 1. Acute myeloid leukemia with an IGH-CCNG1 rearrangement. (A) Chromosome analysis of the bone marrow aspirate showed a complex karyotype, including an unbalanced translocation involving chromosomes 5, 14 and 19. Arrows indicate clonal aberrations. (B) Fluorescence in situ hybridization (FISH) on abnormal metaphase showed the 3'IGH (red) remaining on the derivative chromosome 14 and the 5'IGH lost, consistent with an unbalanced IGH rearrange- ment. -

Molecular Phenotyping Using Networks, Diffusion, and Topology
www.nature.com/scientificreports OPEN Molecular phenotyping using networks, difusion, and topology: soft tissue sarcoma Received: 27 November 2018 James C. Mathews 1, Maryam Pouryahya1, Caroline Moosmüller 2, Yannis G. Kevrekidis2, Accepted: 6 September 2019 Joseph O. Deasy1 & Allen Tannenbaum3 Published: xx xx xxxx Many biological datasets are high-dimensional yet manifest an underlying order. In this paper, we describe an unsupervised data analysis methodology that operates in the setting of a multivariate dataset and a network which expresses infuence between the variables of the given set. The technique involves network geometry employing the Wasserstein distance, global spectral analysis in the form of difusion maps, and topological data analysis using the Mapper algorithm. The prototypical application is to gene expression profles obtained from RNA-Seq experiments on a collection of tissue samples, considering only genes whose protein products participate in a known pathway or network of interest. Employing the technique, we discern several coherent states or signatures displayed by the gene expression profles of the sarcomas in the Cancer Genome Atlas along the TP53 (p53) signaling network. The signatures substantially recover the leiomyosarcoma, dediferentiated liposarcoma (DDLPS), and synovial sarcoma histological subtype diagnoses, and they also include a new signature defned by activation and inactivation of about a dozen genes, including activation of serine endopeptidase inhibitor SERPINE1 and inactivation of TP53-family tumor suppressor gene TP73. Modern biological investigations ofen result in dense, high-dimensional datasets describing genes, proteins, mutations, or other variables. A near universal problem arises as the dimensionality of the data grows: how can the data be investigated in a relatively unbiased manner, to expose underlying clusters and relational structure? To date, there is a lack of robust techniques for exposing the structure of biological data in an unbiased, agnostic fashion. -

Viewed and Approved by the Quencing (RRBS) Kit (Diagenode) Following Manufacturer’S Institutional Animal Care and Use Committee of University Instruction
BASIC RESEARCH www.jasn.org DNMT1 in Six2 Progenitor Cells Is Essential for Transposable Element Silencing and Kidney Development Szu-Yuan Li,1,2,3,4 Jihwan Park ,1,2 Yuting Guan,1,2 Kiwung Chung,1,2 Rojesh Shrestha,1,2 Matthew B. Palmer,5 and Katalin Susztak 1,2 1Renal-Electrolyte and Hypertension Division, Department of Medicine, 2Department of Genetics, and 5Department of Pathology and Laboratory Medicine, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania; 3Division of Nephrology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; and 4School of Medicine, National Yang-Ming University, Taipei, Taiwan ABSTRACT Background Cytosine methylation of regulatory regions, such as promoters and enhancers, plays a key role in regulating gene expression, however, its role in kidney development has not been analyzed. Methods To identify functionally important epigenome-modifying enzymes and genome regions where methylation modifications are functionally important for kidney development, we performed genome- wide methylation analysis, expression profiling, and systematic genetic targeting of DNA methyltrans- ferases (Dnmt1, Dnmt3a,andDnmt3b) and Ten-eleven translocation methylcytosine hydroxylases (Tet2) in nephron progenitor cells (Six2Cre)inmice. Results Genome-wide methylome analysis indicated dynamic changes on promoters and enhancers dur- ing development. Six2CreDnmt3af/f, Six2CreDnmt3bf/f, and Six2CreTet2f/f mice showed no significant struc- tural or functional renal abnormalities. In contrast, Six2CreDnmt1f/f mice died within 24 hours of birth, from a severe kidney developmental defect. Genome-wide methylation analysis indicated a marked loss of methylation of transposable elements. RNA sequencing detected endogenous retroviral transcripts. Expression of intracellular viral sensing pathways (RIG-I), early embryonic, nonrenal lineage genes and increased cell death contributed to the phenotype development. -

A High-Throughput Approach to Uncover Novel Roles of APOBEC2, a Functional Orphan of the AID/APOBEC Family
Rockefeller University Digital Commons @ RU Student Theses and Dissertations 2018 A High-Throughput Approach to Uncover Novel Roles of APOBEC2, a Functional Orphan of the AID/APOBEC Family Linda Molla Follow this and additional works at: https://digitalcommons.rockefeller.edu/ student_theses_and_dissertations Part of the Life Sciences Commons A HIGH-THROUGHPUT APPROACH TO UNCOVER NOVEL ROLES OF APOBEC2, A FUNCTIONAL ORPHAN OF THE AID/APOBEC FAMILY A Thesis Presented to the Faculty of The Rockefeller University in Partial Fulfillment of the Requirements for the degree of Doctor of Philosophy by Linda Molla June 2018 © Copyright by Linda Molla 2018 A HIGH-THROUGHPUT APPROACH TO UNCOVER NOVEL ROLES OF APOBEC2, A FUNCTIONAL ORPHAN OF THE AID/APOBEC FAMILY Linda Molla, Ph.D. The Rockefeller University 2018 APOBEC2 is a member of the AID/APOBEC cytidine deaminase family of proteins. Unlike most of AID/APOBEC, however, APOBEC2’s function remains elusive. Previous research has implicated APOBEC2 in diverse organisms and cellular processes such as muscle biology (in Mus musculus), regeneration (in Danio rerio), and development (in Xenopus laevis). APOBEC2 has also been implicated in cancer. However the enzymatic activity, substrate or physiological target(s) of APOBEC2 are unknown. For this thesis, I have combined Next Generation Sequencing (NGS) techniques with state-of-the-art molecular biology to determine the physiological targets of APOBEC2. Using a cell culture muscle differentiation system, and RNA sequencing (RNA-Seq) by polyA capture, I demonstrated that unlike the AID/APOBEC family member APOBEC1, APOBEC2 is not an RNA editor. Using the same system combined with enhanced Reduced Representation Bisulfite Sequencing (eRRBS) analyses I showed that, unlike the AID/APOBEC family member AID, APOBEC2 does not act as a 5-methyl-C deaminase. -

Cell Cycle Checkpoint Control: the Cyclin G1/Mdm2/P53 Axis Emerges
MOLECULAR AND CLINICAL ONCOLOGY 9: 115-134, 2018 Cell cycle checkpoint control: The cyclin G1/Mdm2/p53 axis emerges as a strategic target for broad‑spectrum cancer gene therapy ‑ A review of molecular mechanisms for oncologists ERLINDA M. GORDON1-3, JOSHUA R. RAVICZ1, SEIYA LIU4, SANT P. CHAWLA1 and FREDERICK L. HALL2,3 1Cancer Center of Southern California/Sarcoma Oncology Center, Santa Monica, CA 90403; 2Aveni Foundation and 3DELTA Next‑Gen, LLC, Santa Monica, CA 90405; 4Department of Cell Biology, Harvard University, Cambridge, MA 02138, USA Received April 16, 2018; Accepted June 14, 2018 DOI: 10.3892/mco.2018.1657 Abstract. Basic research in genetics, biochemistry and cell progression; ii) is supported by studies of inhibitory microRNAs biology has identified the executive enzymes and protein kinase linking CCNG1 expression to the mechanisms of carcinogenesis activities that regulate the cell division cycle of all eukaryotic and viral subversion; and iii) provides a mechanistic basis for organisms, thereby elucidating the importance of site‑specific understanding the broad‑spectrum anticancer activity and protein phosphorylation events that govern cell cycle progression. single‑agent efficacy observed with dominant‑negative cyclin Research in cancer genomics and virology has provided G1, whose cytocidal mechanism of action triggers programmed meaningful links to mammalian checkpoint control elements cell death. Clinically, the utility of companion diagnostics for with the characterization of growth‑promoting proto‑oncogenes cyclin G1 pathways is anticipated in the staging, prognosis encoding c‑Myc, Mdm2, cyclins A, D1 and G1, and opposing and treatment of cancers, including the potential for rational tumor suppressor proteins, such as p53, pRb, p16 INK4A and p21WAF1, combinatorial therapies. -

Variation in Protein Coding Genes Identifies Information Flow
bioRxiv preprint doi: https://doi.org/10.1101/679456; this version posted June 21, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Animal complexity and information flow 1 1 2 3 4 5 Variation in protein coding genes identifies information flow as a contributor to 6 animal complexity 7 8 Jack Dean, Daniela Lopes Cardoso and Colin Sharpe* 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Institute of Biological and Biomedical Sciences 25 School of Biological Science 26 University of Portsmouth, 27 Portsmouth, UK 28 PO16 7YH 29 30 * Author for correspondence 31 [email protected] 32 33 Orcid numbers: 34 DLC: 0000-0003-2683-1745 35 CS: 0000-0002-5022-0840 36 37 38 39 40 41 42 43 44 45 46 47 48 49 Abstract bioRxiv preprint doi: https://doi.org/10.1101/679456; this version posted June 21, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Animal complexity and information flow 2 1 Across the metazoans there is a trend towards greater organismal complexity. How 2 complexity is generated, however, is uncertain. Since C.elegans and humans have 3 approximately the same number of genes, the explanation will depend on how genes are 4 used, rather than their absolute number. -

Discordant Gene Responses to Radiation in Humans and Mice and the Role of Hematopoietically Humanized Mice in the Search for Radiation Biomarkers Shanaz A
www.nature.com/scientificreports OPEN Discordant gene responses to radiation in humans and mice and the role of hematopoietically humanized mice in the search for radiation biomarkers Shanaz A. Ghandhi *, Lubomir Smilenov, Igor Shuryak, Monica Pujol-Canadell & Sally A. Amundson The mouse (Mus musculus) is an extensively used model of human disease and responses to stresses such as ionizing radiation. As part of our work developing gene expression biomarkers of radiation exposure, dose, and injury, we have found many genes are either up-regulated (e.g. CDKN1A, MDM2, BBC3, and CCNG1) or down-regulated (e.g. TCF4 and MYC) in both species after irradiation at ~4 and 8 Gy. However, we have also found genes that are consistently up-regulated in humans and down- regulated in mice (e.g. DDB2, PCNA, GADD45A, SESN1, RRM2B, KCNN4, IFI30, and PTPRO). Here we test a hematopoietically humanized mouse as a potential in vivo model for biodosimetry studies, measuring the response of these 14 genes one day after irradiation at 2 and 4 Gy, and comparing it with that of human blood irradiated ex vivo, and blood from whole body irradiated mice. We found that human blood cells in the hematopoietically humanized mouse in vivo environment recapitulated the gene expression pattern expected from human cells, not the pattern seen from in vivo irradiated normal mice. The results of this study support the use of hematopoietically humanized mice as an in vivo model for screening of radiation response genes relevant to humans. Most in vivo studies in which efects of external stimuli on human health are assessed require a model organism, and the mouse (Mus musculus) is the best studied small animal model system. -

Open Moore Sarah P53network.Pdf
THE PENNSYLVANIA STATE UNIVERSITY SCHREYER HONORS COLLEGE DEPARTMENT OF BIOCHEMISTRY AND MOLECULAR BIOLOGY A SYSTEMATIC METHOD FOR ANALYZING STIMULUS-DEPENDENT ACTIVATION OF THE p53 TRANSCRIPTION NETWORK SARAH L. MOORE SPRING 2013 A thesis submitted in partial fulfillment of the requirements for a baccalaureate degree in Biochemistry and Molecular Biology with honors in Biochemistry and Molecular Biology Reviewed and approved* by the following: Dr. Yanming Wang Associate Professor of Biochemistry and Molecular Biology Thesis Supervisor Dr. Ming Tien Professor of Biochemistry and Molecular Biology Honors Advisor Dr. Scott Selleck Professor and Head, Department of Biochemistry and Molecular Biology * Signatures are on file in the Schreyer Honors College. i ABSTRACT The p53 protein responds to cellular stress, like DNA damage and nutrient depravation, by activating cell-cycle arrest, initiating apoptosis, or triggering autophagy (i.e., self eating). p53 also regulates a range of physiological functions, such as immune and inflammatory responses, metabolism, and cell motility. These diverse roles create the need for developing systematic methods to analyze which p53 pathways will be triggered or inhibited under certain conditions. To determine the expression patterns of p53 modifiers and target genes in response to various stresses, an extensive literature review was conducted to compile a quantitative reverse transcription polymerase chain reaction (qRT-PCR) primer library consisting of 350 genes involved in apoptosis, immune and inflammatory responses, metabolism, cell cycle control, autophagy, motility, DNA repair, and differentiation as part of the p53 network. Using this library, qRT-PCR was performed in cells with inducible p53 over-expression, DNA-damage, cancer drug treatment, serum starvation, and serum stimulation. -

Modulation of Cell Cycle and Gene
1338 Modulation of cell cycle and gene expression in pancreatic tumor cell lines by methionine deprivation (methionine stress): implications to the therapy of pancreatic adenocarcinoma Demetrius M. Kokkinakis, XiaoYan Liu, regulation and LMNB1, AREG, RhoB, CCNG, TYMS, F3, and Russell D. Neuner and MGMT down-regulation suggest that methionine stress sensitizes the tumor cells to DNA-alkylating drugs, Department of Pathology and the Cancer Institute, University of 5-fluorouracil, and radiation. Increased sensitivity of Pittsburgh, Pittsburgh, Pennsylvania pancreatic tumor cell lines to temozolomide is shown under methionine stress conditions and is attributed in part 6 Abstract to diminished O -methylguanine-DNA methyltransferase and possibly to inhibition of the cell cycle progression. [Mol The effect of methionine deprivation (methionine stress) on Cancer Ther 2005;4(9):1338–48] the proliferation, survival, resistance to chemotherapy, and regulation of gene and protein expression in pancreatic tumor lines is examined. Methionine stress prevents Introduction successful mitosis and promotes cell cycle arrest and Pancreatic adenocarcinoma is the fourth leading cause of accumulation of cells with multiple micronuclei with death in the United States, with an estimated incident of decondensed chromatin. Inhibition of mitosis correlates 30,000 victims annually. Most patients who are diagnosed with CDK1 down-regulation and/or inhibition of its function with this tumor die within a year and the 5-year survival is 15 161 by Tyr phosphorylation or Thr dephosphorylation. <5%. Only a very few tumors are as aggressive as pancreatic Inhibition of cell cycle progression correlates with loss of cancer, and unlike many other cancers, early discovery does hyperphosphorylated Rb and up-regulation of p21 via p53 not always lead to improved survival (1). -
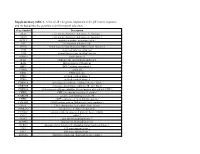
Supplementary Table 1. a List of All 142 Genes Important in the P53 Stress Response and Included Into the Genomic Scan for Natural Selection
Supplementary table 1. A list of all 142 genes important in the p53 stress response and included into the genomic scan for natural selection. Gene Symbol Description AKT1 v-akt murine thymoma viral oncogene homolog 1 AKT2 v-akt murine thymoma viral oncogene homolog 2 APAF1 apoptotic peptidase activating factor 1 APC adenomatous polyposis coli APEX1 APEX nuclease (multifunctional DNA repair enzyme) 1 ATM ataxia telangiectasia mutated ATR ataxia telangiectasia and Rad3 related AURKA aurora kinase A BAI1 brain-specific angiogenesis inhibitor 1 BAX BCL2-associated X protein BBC3 BCL2 binding component 3 CCNG1 cyclin G1 CD82 CD82 molecule CDK2 cyclin-dependent kinase 2 CDK8 cyclin-dependent kinase 8 CDKN1A cyclin-dependent kinase inhibitor 1A (p21, Cip1) CDKN1B cyclin-dependent kinase inhibitor 1B (p27, Kip1) CDKN2A cyclin-dependent kinase inhibitor 2A (melanoma, p16, inhibits CDK4) CHEK2 CHK2 checkpoint homolog (S. pombe) CORO1B coronin, actin binding protein, 1B CREB1 cAMP responsive element binding protein 1 CREBBP CREB binding protein (Rubinstein-Taybi syndrome) CSE1L CSE1 chromosome segregation 1-like (yeast) CSNK2A1 casein kinase 2, alpha 1 polypeptide CTNNB1 catenin (cadherin-associated protein), beta 1, 88kDa CUL7 cullin 7 DUSP1 dual specificity phosphatase 1 DUSP16 dual specificity phosphatase 16 DYRK2 dual-specificity tyrosine-(Y)-phosphorylation regulated kinase 2 E2F1 E2F transcription factor 1 E4F1 E4F transcription factor 1 EEF1A1 eukaryotic translation elongation factor 1 alpha 1 EIF4EBP1 eukaryotic translation initiation factor 4E binding protein 1 ESR1 estrogen receptor 1 ESR2 estrogen receptor 2 (ER beta) FAS Fas (TNF receptor superfamily, member 6) FCGR1A Fc fragment of IgG, high affinity Ia, receptor (CD64) FHL2 four and a half LIM domains 2 FLT1 fms-related tyrosine kinase 1 (vasc.