MRP-An Exploration of Strategies for an Uncertain Future for CNIB
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DISCLAIMER This Presentation Reflects the Views of the Authors
DISCLAIMER This presentation reflects the views of the authors only and does not reflect the views or policies of Transport Canada. Neither Transport Canada, nor its employees, makes any warranty, express or implied, or assumes any legal liability or responsibility for the accuracy or completeness of any information contained in this presentation, or process described herein, and assumes no responsibility for anyone’s use of the information. Cette présentation est disponible en anglais seulement. Looking Forward: Autonomous Vehicles and Accessibility The landscape from an accessibility perspective About CNIB • Celebrating 100 years in 2018, the CNIB Foundation is a non-profit organization driven to change what it is to be blind today. • We deliver innovative programs and powerful advocacy that empowers people impacted by blindness to live their dreams and tear down barriers to inclusion. • Now, as CNIB enters our second century of operation, we're going to be even bolder in tackling the issues before us. Sight loss in Canada • According to Statistics Canada’s 2017 Survey on Disability, 1.5 million Canadians have a vision impairment • An estimated 5.59 million more have an eye disease that could cause sight loss Sight loss in Canada – continued • The four leading causes of sight loss in Canada are: • Cataracts: 3,541,000 people • Age-related macular degeneration: 1,574,000 people • Glaucoma: 294,000 people • Diabetic retinopathy: 749,800 CNIB Research on CAV Technology CNIB, with partial funding from Transport Canada, completed a report and provided the following 7 recommendations: • Accessibility and usability of onboard vehicle interfaces; • Avoiding adoption of signals which rely exclusively on visual queuing to indicate a vehicle's state. -

Summary of Experience
SUMMARY OF EXPERIENCE A. PARALYMPIAN (defined as having competed at a Paralympic Games) ☒ Yes or No ☐ B. CAREER List your 3 most recent positions of employment (paid/volunteer) below: 1. Legal Counsel, Office of the Chief Division, Calgary Police Service; 2. Associate Litigation Lawyer, McCarthy Tétrault 3. Articling Student, McCarthy Tétrault C. BOARD EXPERIENCE (not-for-profit, for profit) List your 3 most recent Board positions below: 1. CNIB Foundation Board of Directors: I currently chair the Risk Committee and serve as a member of the Strategy Committee. I was the Chair of the Investment Committee for two years, and also served as a member of the Finance and Risk Management Committee and the Advocacy Committee. In these roles, I have assisted CNIB in moving to an Outsourced Chief Investment Officer model for overseeing the organization’s investments on a day-to-day basis. In the risk area, I have assisted the organization in re- designing its risk register to account for risks in its regular operations and helped to build a special register which addresses risks unique to the current Covid-19 pandemic. Since the Risk Committee was a new committee formed in 2018, I assisted in the drafting of the Terms of Reference and in developing a risk assessment tool to be used by staff in assessing both the frequency and severity of risks that may arise when the organization assesses whether to offer specific programs to the public. 2. Vice-President, International Blind Sports Association: I have held this position since 2017 after serving as Special Advisor to the President for two years. -

CNIB's Guide Dog Program
CNIB’s Guide Dog Program Mobility. Independence. Partnership. Sight Loss Changes Everything In Canada today, more than two million people are living with a “I am more sight-threatening eye disease (age-related macular degeneration, cataracts, diabetic retinopathy and glaucoma) and are at serious engaged in the risk of losing their sight. With almost 100 years of history serving world, and my blind and partially sighted Canadians, CNIB can help to meet these guide dog Tiffany challenges and ensure Canadians with sight loss have the support they need to live connected, rewarding and independent lives – has given me a but only with your support. freedom of spirit For people who are blind or partially sighted, mobility is a cornerstone that I hadn’t had of independence. The ability to participate fully in life and in the since before I community is intrinsically linked to the ability to navigate one’s surroundings safely and with confidence. Safe mobility can be started using facilitated through in-depth training and the use of different tools, my cane. I have from the widely-used and recognized white cane to innovative, always loved to high-tech devices. be active and Guide dogs, which are specially bred and trained to provide mobility move around assistance to people who are blind or partially sighted, are more than just a tool – rather, they are a partner in independence that can open quickly, and up the world in a profoundly different way. For many people, the use working with of a guide dog can instill greater confidence in exploring unfamiliar Tiffany has given environments, knowing the dog is also trained to avoid obstacles and hazards. -

Health & Wellbeing
HEALTH & WELLBEING TTY: 780.427.1570 Chapter Contents www.alberta.ca/aish.aspx •Alberta Aids to Daily Living • AISH Health Benefits may assist eligible AISH clients with their essential medical •Home Health Care and needs. Medical Equipment Suppliers See FINANCE - Provincial Financial •Medical Equipment Loans Programs & Benefits for complete listing. •Alberta Health Services -Health Link Alberta Alberta Health -Continuing Care- Home Care 10th Floor, Milner Building, -Day Programs 10040 104 St. NW T5J 0Z2 -CHOICE Phone: 780.427.0731 -Rehabilitation Toll Free outside of Edmonton: 310.0000 -Mental Health then 780.427.0731 -Palliative Care Website: www.alberta.ca/alberta-aidsto- -Hospitals daily-living.aspx • Alberta Aids to Daily Living (AADL) -Finding a Doctor funds basic medical equipment -Medical Clinics and supplies to help Albertans with -After Hours Care longterm disabilities, chronic and -Public Health Centres terminal illnesses, stay independent in •Caregiver Support their communities. •Counselling • AADL is a cost-share program. Clients pay 25% of the benefit cost up to •Dental Services a maximum of $500 per family per •Fall Prevention year. If you receive provincial income •Health Benefit Plans assistance, or if your income is below •Health Service Organizations qualifying thresholds, you may be •Home Health Care Agencies exempt from cost-share payments. •Podiatry and Foot Care • To obtain AADL funding, you must be •Optometry assessed by an approved healthcare professional. That person determines •Addictions Recovery what equipment and supplies you •Pets can get through the AADL program. If you are eligible, they will give you an authorization for products from AADL’s ALBERTA AIDS TO DAILY product list. -

2018/19 Ontario & Quebec Annual Report
2018-19 Annual Report CNIB Foundation (Ontario & Quebec) Leadership Team Angela Bonfanti Suzanne Decary-van den Broek David Demers Vice-President Executive Director Executive Director Ontario & Quebec Ontario South (GTA) Québec Robert Gaunt Duane Morgan Monique Pilkington Executive Director Executive Director National Director, CNIB Eye Van & Ontario North & Ontario West Ontario East Executive Director, CNIB Lake Joe CNIB Foundation (Ontario & Quebec) Board of Directors Monica Lowe Menecola, Chair; Jack McCormick, Vice Chair; Sath Dosanjh; Dr. Louise Hale; Venkat Iyer; Jason Mitschele; Scott Seiler; Alison Simpson; Glen Wade and Richard Wise. Values Empowerment | Inclusiveness | Innovation | Passion | Collaboration | Integrity Making the future bright Life is a beautiful, wonderful, complicated A CNIB Community Hub isn’t just a physical thing. Life with blindness should be no space; it’s a unique programming concept different. Together, we’re empowering people where participants connect with others. with sight loss to lead independent, active lives Whether it’s kids and parents having and chase their dreams – and we’re smashing playgroups with tactile toys, teens trying out the stigma and barriers that stand in their way. virtual reality rooms, or adults reviewing the latest bestseller in braille book clubs, there’s Recent research confirms what we’ve been something for everyone! hearing for years: employment levels are a serious problem facing people with sight loss. At CNIB Lake Joe, attendance reached a five- With all the technological advancements and year high – 660 participants – a 34 per cent educational opportunities available, people increase over 2017. We introduced new youth with sight loss shouldn’t be disadvantaged programs, including English immersion for when trying to find a job. -
Career Support and Employment Programs
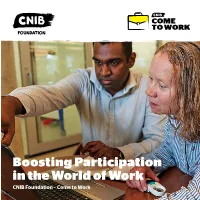
COME TO WORK Boosting Participation in the World of Work CNIB Foundation – Come to Work We’re changing the employment reality for those with sight loss • Only 28%1 of working-age adults with sight loss are employed full time, compared to the national employment rate of 65.5%2 • Those with sight loss are almost twice as likely to be employed if they have a post-secondary degree, compared with peers who only completed high school • The household income for working-age Canadians with sight loss is two-thirds the national average of the general population • $15.3 billion is the estimated annual cost to the national economy of un-and under-employed Canadians with sight loss 1International Levels of Employment Survey (ILES), 2018, CNIB 2International Levels of Employment Study (ILES), 2018, CNIB. Presented at 11th Annual Accessibility Conference, May 2019, University of Guelph In Canada, the number of working age adults with sight loss who are employed full time is half that of the general population.3 Many of those individuals with sight loss who are employed, are struggling to make ends meet. Nearly 1.5 million Canadians live with some form of sight loss, representing a significant talent pool for employers in diverse fields including science, law, engineering, creative arts, technology and broadcasting, amongst many others. The Canadian economy benefits when all skilled, well-qualified Canadians are employed and contributing. Employers report that candidates who are blind or partially sighted, while educated, often need to develop pre-employment skills. Due to misconceptions, a lack of understanding and the stigma associated with sight loss, those with sight loss tend to be excluded from the social, emotional, physical, educational and employment opportunities that are aforded to those with sight. -
Enabling Change for Retailers: Make Your Store Accessible
DECEMBER 2019 MARCHGuidebook 2019 SpecialFor Edition WhiteRetailers Paper EnAbling Change for Retailers: Make your Store Accessible Table of Contents 1. Accessible stores ......................................................................... 7 1.1 People with disabilities: facts and figures ...................................................................... 7 1.2 Types of disabilities ................................................................................................................. 8 1.3 Legislation ..................................................................................................................................10 1.4 Skilled talent pool .................................................................................................................... 11 2. Accessible customer service ...................................................... 13 2.1 Barriers to accessible customer service ....................................................................... 23 2.2 Support persons ..................................................................................................................... 23 2.3 Guide dogs and other service animals .......................................................................... 24 2.4 Assistive devices .................................................................................................................... 27 2.5 Customer service policy ..................................................................................................... 30 3. Accessible -

Canada's National Visually Impaired Paratriathlon Team
The Voice of WHITEthe Blind™ in Canada CANE MAGAZINE2011 ISSUE SWIM BIKE RUN Canada’s National Visually Impaired Paratriathlon Team DISCOVER PARticipate GET INVOLVED Won with One is the Canadian Council Won with One is focused on Access to sport for the blind and of the Blind’s newest program which is empowering individuals via sport and visually impaired community is not focused on the personal development providing assistance and resources based on lack of ability, but rather a of the blind and visually impaired vital for our triathletes to achieve a lack of opportunity. Won with One using triathlon as the catalyst for slot on the 2016 Canadian Paralympics strives to provide opportunities so change. Along with their sighted team. We are determined to show the all persons are able to compete as guides athletes swim, bike and run as abilities of the blind and how they can equals. You can be part of that change! equals on and off the course. be regarded as equals in sport and in www.wonwithone.com life. Novartis Pharmaceuticals Canada Inc. is one of the world’s leading healthcare companies committed to improving vision health. Innovation is the heart of our research strategy. We discover and develop medicines that make a real difference. There can be no delay. Patients are waiting. Client: SANOFI-AVENTIS Brand: Lovenox Lovenox TearPad 9147 EN Ad No: 9147 Lovenox Colour: 4/c process Trim: 8.5" x 14” www.novartis.ca140957/2009/09/04/SC 140957_9147_Lovenox_TearPad_EN Client: SANOFI-AVENTIS Brand: Lovenox Client: NOVARTIS Lovenox TearPad 9147 -

Barney Bentall Rewire Your Brain Towards Positivity Going Above & Beyond During a Global Pandemic Fall/Winter 2020 Fashion Trends
INSPIRED 55+ lifestyle magazine JULY 2020 BARNEY BENTALL REWIRE YOUR BRAIN TOWARDS POSITIVITY GOING ABOVE & BEYOND DURING A GLOBAL PANDEMIC FALL/WINTER 2020 FASHION TRENDS Inspiration for people over 55 • www.seniorlivingmag.com INSPIRED | JULY 2020 1 The Gulf War in the early 1990s was followed by the exodus of 1.5 million Iraqi Kurds. Some refugees, including these children, were able to Live your best life. return home within weeks. Trust in Berwick. We empower our residents to live their best life with us. Our homes are adaptive to whatever changes may come and the safety of our communities and our people is paramount. Join one of our vibrant communities today and enjoy a safe, active and healthy lifestyle. “These are challenging times and Berwick deserves kudos for all of their efforts and measures taken to keep us well and safe. Thank you to each and every one of you. You are all so wonderful and that helps brighten the days.” BerwickRetirement.com CAMPBELL RIVER | COMOX | KAMLOOPS | NANAIMO VICTORIA: GORDON HEAD & ROYAL OAK QUALICUM BEACH | PARKSVILLE (COMING SOON) Your legacy could be their childhood YOU CAN BE THEIR REFUGE ©UNHCR/A.Roulet You know the importance of estate planning to make sure With a gift to UNHCR in your loved ones are taken care of. Did you also know you your Will, you can offer can make a lasting and significant impact to save and protect We didn’t expect a pandemic. the lives of the most vulnerable refugees—and give them the Amelie, 2 Judah, 2 Ben, 4 Olivia, 7 refugees fleeing violence, opportunity of a brighter future? “We joined the Legacy Circle and Neither did the animals. -

“Hire the Handicapped!” Disability Rights, Economic Integration and Working Lives in Toronto, Ontario, 1962-2005
i “HIRE THE HANDICAPPED!” DISABILITY RIGHTS, ECONOMIC INTEGRATION AND WORKING LIVES IN TORONTO, ONTARIO, 1962-2005 DUSTIN GALER A THESIS SUBMITTED IN CONFORMITY WITH THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY GRADUATE DEPARTMENT OF HISTORY IN THE UNIVERSITY OF TORONTO © by Dustin Galer JUNE 2014 ii “Hire the Handicapped!” Disability Rights, Economic Integration and Working Lives in Toronto, Ontario, 1962-2005 Dustin Galer Doctor of Philosophy Department of History University of Toronto 2014 Abstract This dissertation, “‘Hire the Handicapped!’: Disability Rights, Economic Integration and Working Lives in Toronto, Ontario, 1962-2005,” argues that work significantly shaped the experience of disability during this period. Barriers to mainstream employment opportunities gave rise to multiple disability movements that challenged the social and economic framework which marginalized generations of people with disabilities. Using a critical analysis of disability in archival records, personal collections, government publications and a series of interviews, I demonstrate how demands for greater access among disabled people to paid employment stimulated the development of a new discourse of disability in Canada. Including disability as a variable in historical research reveals how family advocates helped people living in institutions move out into the community and rehabilitation professionals played an increasingly critical role in the lives of working-age adults with disabilities, civil rights activists crafted a new consumer- led vision of social and economic integration. Separated by different philosophies and bases of support, disability activists and allies found a common purpose in their pursuit of economic integration. iii The focus on employment issues among increasingly influential disability activists during this period prompted responses from three key players in the Canadian labour market. -

Overcoming Barriers to Adoption and Implementation of Web Accessibility
Access Denied 1 Access Denied: Overcoming Barriers to Adoption and Implementation of Web Accessibility by Glen Farrelly A thesis submitted in partial fulfillment of the requirements for the degree of MASTER OF ARTS in PROFESSIONAL COMMUNICATION We accept the thesis as conforming to the required standard ________________________________________________ Dr. Michael Real, Thesis Supervisor Date School of Communication & Culture Royal Roads University ________________________________________________ Dr. Phillip Vannini, Thesis Co-ordinator Date School of Communication & Culture Royal Roads University ________________________________________________ Dr. David Black, Internal Committee Member Date School of Communication & Culture Royal Roads University ________________________________________________ Dr. Gerry Nixon, External Committee Member Date School of Leadership Studies Royal Roads University ________________________________________________ Dr. Joshua Guilar, Director Date School of Communication & Culture Royal Roads University Royal Roads University, July 2009 © Glen Farrelly 2009 [email protected] Library and Archives Bibliothèque et Canada Archives Canada Published Heritage Direction du Branch Patrimoine de l’édition 395 Wellington Street 395, rue Wellington Ottawa ON K1A 0N4 Ottawa ON K1A 0N4 Canada Canada Your file Votre référence ISBN: 978-0-494-58696-9 Our file Notre référence ISBN: 978-0-494-58696-9 NOTICE: AVIS: The author has granted a non- L’auteur a accordé une licence non exclusive exclusive license allowing Library -

About the CNIB Foundation Celebrating 100 Years in 2018, the CNIB Foundation Is a Non-Profit Organization Driven to Change What It Is to Be Blind Today
About the CNIB Foundation Celebrating 100 years in 2018, the CNIB Foundation is a non-profit organization driven to change what it is to be blind today. We deliver innovative programs and powerful advocacy that empowers people impacted by blindness to live their dreams and tear down barriers to inclusion. Now, as CNIB enters our second century of operation, we're going to be even bolder in tackling the issues before us. Background The CNIB Foundation thanks the Advisory Committee to the Open Banking Review for an opportunity to provide recommendations regarding a Canadian Open Banking system. Our recommendations are intended to provide the committee with an understanding of potential barriers that would limit access to open banking for all Canadians if interfaces are not designed with accessibility at their core. This submission represents one of several made by the CNIB Foundation over recent years. Our goal in each of these public consultations is to provide the government with suggestions for removing the barriers that exist within the financial services sector for Canadians who are blind or partially sighted. The Finance Canada public consultations to which CNIB has provided input include: 1. Disability Component to the Official Development Assistance Accountability Act – January 2011 2. The Development of a Comprehensive Financial Consumer Code – February 2014 3. Balancing Oversight and Innovation in the ways we pay – 2015 4. Positioning Canada's Financial Sector for the Future – November 2016 We consent to this submission being shared publicly without any reservation. Sight Loss in Canada According to the 2017 Statistics Canada Survey on Disability, five percent of Canadians report a vision related disability.