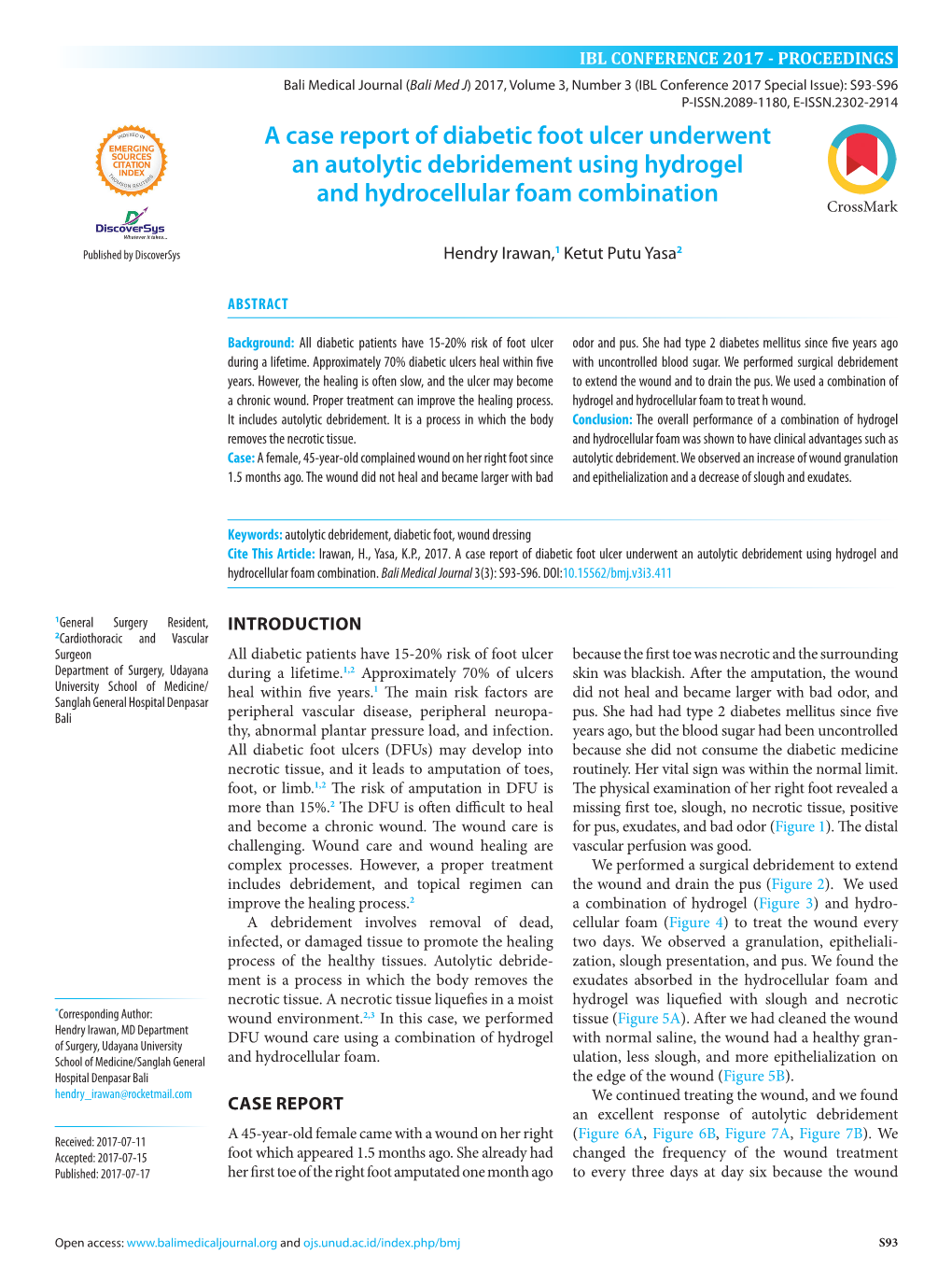
A Case Report of Diabetic Foot Ulcer Underwent an Autolytic Debridement Using Hydrogel and E-ISSN.2302-2914 Hydrocellular Foam Combination
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gonorrhea Can Be Easily Cured with Antibiotics from a If You Are Pregnant, It Is Even More Important to Get Health Care Provider
GET YOURSELF TESTED Testing is confidential. If you are under 18 years old, you can consent to be checked and treated for STIs. What if I don’t get treated? What if I am pregnant? Gonorrhea can be easily cured with antibiotics from a If you are pregnant, it is even more important to get health care provider. tested by your health care provider and treated if you have gonorrhea. Left untreated, gonorrhea can be However, if gonorrhea is not treated, it can cause Gonorrhea passed to your baby during vaginal delivery and can permanent damage: cause serious health problems. • Your risk of getting other STIs, like gonorrhea or • Babies are usually treated with an antibiotic HIV increases. shortly after birth. If a baby with gonorrhea isn’t • In females, untreated gonorrhea can increase the treated, they may become blind. chances of getting pelvic inflammatory disease (PID), an infection of the reproductive organs, which can make it hard to get pregnant or carry a To learn more baby full-term. Contact a health care provider or your local STI clinic. • In males, untreated gonorrhea can lead to sterility To learn more about STIs, or to find your local (inability to make sperm and have children). STI clinic, visit www.health.ny.gov/STD. You can find other STI testing locations at What about my sex partner(s)? https://gettested.cdc.gov. Gonorrhea is a sexually transmitted infection. If you have gonorrhea, your sex partner(s) should get tested. If they have gonorrhea, they will need to take medicine to cure it. -

Get the Facts About Necrotizing Fasciitis: “Flesh-Eating Disease”
Get the facts about necrotizing fasciitis: “Flesh-eating Disease” What is necrotizing fasciitis? There are many strains of bacteria that can cause the flesh-eating disease known as necrotizing fasciitis, but most cases are caused by a bacteria called group A strep, or Streptococcus pyogenes. More common infections with group A strep are not only strep throat, but also a skin infection called impetigo. Flesh-eating strep infections or necrotizing fasciitis is considered rare. Necrotizing fasciitis is a treatable disease. Only certain rare bacterial strains are able to cause necrotizing fasciitis, but these infections progress rapidly so the sooner one seeks medical care, the better the chances of survival. The bacteria actually cause extensive tissue damage because the tissues under the skin and those surrounding muscle and body organs are destroyed; necrotizing fasciitis is extensive and can lead to death. Is this a new disease? No. The flesh-eating infections have been described as early as the fifth century B.C. based on written accounts of necrotizing fasciitis by Hippocrates. More than 2,000 cases of this condition were reported among soldiers during the Civil War. Cases in the U.S. are generally infrequent, although small epidemics have occurred, such as the 1996 outbreak in San Francisco among injection drug abusers using contaminated “black tar” heroin. What are the signs and symptoms? Persons with the flesh-eating infection know something is wrong because of extreme pain in the infected area. Generally, an infection begins at a surgical wound or because of accidental trauma—sometimes without an obvious break in the skin—accompanied by severe pain, followed by swelling, fever, and sometimes confusion. -

What Is Staphylococcus Aureus (Staph)?
What is Staphylococcus aureus (staph)? Staphylococcus aureus, often referred to simply as "staph," are bacteria commonly carried on the skin or in the nose of healthy people. Approximately 25% to 30% of the population is colonized (when bacteria are present, but not causing an infection) in the nose with staph bacteria. Sometimes, staph can cause an infection. Staph bacteria are one of the most common causes of skin infections in the United States. Most of these skin infections are minor (such as pimples and boils) and can be treated without antibiotics (also known as antimicrobials or antibacterials). However, staph bacteria also can cause serious infections (such as surgical wound infections, bloodstream infections, and pneumonia). What is MRSA (methicillin-resistant Staphylococcus aureus)? Some staph bacteria are resistant to antibiotics. MRSA is a type of staph that is resistant to antibiotics called beta-lactams. Beta-lactam antibiotics include methicillin and other more common antibiotics such as oxacillin, penicillin and amoxicillin. While 25% to 30% of the population is colonized with staph, approximately 1% is colonized with MRSA. Who gets staph or MRSA infections? Staph infections, including MRSA, occur most frequently among persons in hospitals and healthcare facilities (such as nursing homes and dialysis centers) who have weakened immune systems. These healthcare-associated staph infections include surgical wound infections, urinary tract infections, bloodstream infections, and pneumonia. Are people who are positive for the human immune deficiency virus (HIV) at increased risk for MRSA? Should they be taking special precautions? People with weakened immune systems, which include some patients with HIV infection, may be at risk for more severe illness if they get infected with MRSA. -

Abscesses Are a Serious Problem for People Who Shoot Drugs
Where to Get Your Abscess Seen Abscesses are a serious problem for people who shoot drugs. But what the hell are they and where can you go for care? What are abscesses? Abscesses are pockets of bacteria and pus underneath you skin and occasionally in your muscle. Your body creates a wall around the bacteria in order to keep the bacteria from infecting your whole body. Another name for an abscess is a “soft tissues infection”. What are bacteria? Bacteria are microscopic organisms. Bacteria are everywhere in our environment and a few kinds cause infections and disease. The main bacteria that cause abscesses are: staphylococcus (staff-lo-coc-us) aureus (or-e-us). How can you tell when you have an abscess? Because they are pockets of infection abscesses cause swollen lumps under the skin which are often red (or in darker skinned people darker than the surrounding skin) warm to the touch and painful (often VERY painful). What is the worst thing that can happen? The worst thing that can happen with abscesses is that they can burst under your skin and cause a general infection of your whole body or blood. An all over bacterial infection can kill you. Another super bad thing that can happen is a endocarditis, which is an infection of the lining of your heart, and “septic embolism”, which means that a lump of the contaminates in your abscess get loose in your body and lodge in your lungs or brain. Why do abscesses happen? Abscesses are caused when bad bacteria come in to contact with healthy flesh. -

Cellulitis (You Say, Sell-You-Ly-Tis)
Cellulitis (you say, sell-you-ly-tis) Any area of skin can become infected with cellulitis if the skin is broken, for example from a sore, insect bite, boil, rash, cut, burn or graze. Cellulitis can also infect the flesh under the skin if it is damaged or bruised or if there is poor circulation. Signs your child has cellulitis: The skin will look red, and feel warm and painful to touch. There may be pus or fluid leaking from the skin. The skin may start swelling. The red area keeps growing. Gently mark the edge of the infected red area How is with a pen to see if the red area grows bigger. cellulitis spread? Red lines may appear in the skin spreading out from the centre of the infection. Bad bacteria (germs) gets into broken skin such as a cut or insect bite. What to do Wash your hands before and Cellulitis is a serious infection that needs to after touching the infected area. be treated with antibiotics. Keep your child’s nails short and Go to the doctor if the infected area is clean. painful or bigger than a 10 cent piece. Don’t let your child share Go to the doctor immediately if cellulitis is bath water, towels, sheets and near an eye as this can be very serious. clothes. Make sure your child takes the antibiotics Make sure your child rests every day until they are finished, even if and eats plenty of fruit and the infection seems to have cleared up. The vegetables and drinks plenty of antibiotics need to keep killing the infection water. -

Acute Pelvic Inflammatory Disease: Tests and Treatment Information for for You You
Acute pelvic inflammatory disease: tests and treatment Information for for you you Published August 2010 Published in August 2010 (next review date: 2014) AcuteWhat is pelvic pelvic inflammatory inflammatory disease? disease: testsPelvic inflammatory and treatmentdisease (PID) is an inflammation in the pelvis. It is usually caused by an infection spreading from the vagina and cervix (entrance of the uterus) to the uterus (womb), fallopian tubes, ovaries and pelvic area. If severe, Whatthe infection is pelvicmay result inflammatory in an abscess (collection disease? of pus) forming inside the Pelvicpelvis. inflammatory This is most disease commonly (PID) is aan tubo-ovarian inflammation inabscess the pelvis. (an It isabscess usually caused affecting by an the infection spreadingtubes and from ovaries). the vagina and cervix (entrance of the uterus) to the uterus (womb), fallopian tubes, ovaries and pelvic area. If severe, the infection may result in an abscess (collection of pus) forming inside the pelvis. ThisPID isis most common commonly and aaccounts tubo-ovarian for abscessone in (an60 abscessGP visits affecting by women the tubes under and ovaries). the age of 45 years. PID is common and accounts for one in 60 GP visits by women under the age of 45 years. fallopian tube uterus (womb) pelvis ovary or pelvic area uterus lining entrance (endometrium) of the uterus (cervix) vagina What is is ‘acute’ ‘acute’ pelvic pelvic inflammatory inflammatory disease? disease? Acute PID is when there is sudden or severe inflammation of the uterus, Acute PID is when there is sudden or severe inflammation of the uterus, fallopian tubes,fallopian ovaries tubes, and ovariespelvic area and due pelvic to infection. -

Gonorrhea Fact Sheet
FACT SHEET GONORRHEA What is gonorrhea? Gonorrhea is a sexually transmitted disease (STD) caused by a bacterium that can grow and multiply easily in the warm, moist areas of the reproductive tract, including the cervix (opening to the womb), uterus (womb), and fallopian tubes (egg canals) in women, and in the urethra (urine canal) in women and men. The germ can also grow in the mouth, throat, eyes, and anus (butt). How do people get gonorrhea? Gonorrhea is spread through contact between the penis, vagina, mouth, and anus. A man does not have to ejaculate to give gonorrhea to a sexual partner. Gonorrhea can also be transmitted to a baby during birth if the mother is infected. Gonorrhea infection can spread to other parts of the body. For example, a person can get an eye infection after touching infected genitals (private areas) and then the eyes. People who have been treated for gonorrhea may get it again if they have sexual contact with another person or untreated partner who has gonorrhea. Who is at risk for gonorrhea? Any sexually active person can be infected with gonorrhea. In the United States, the highest reported rates of infection are among sexually active teenagers, young adults, and African Americans. What are the signs and symptoms of gonorrhea? Some men have signs or symptoms that appear 2 - 5 days after infection, but the symptoms can take as long as 30 days to appear or may not appear at all. Signs and symptoms include a burning sensation when urinating (peeing), or a white, yellow, or green discharge from the penis. -

Necrotizing Soft-Tissue Infections
11/1/2020 Necrotizing Fasciitis ▪Is a surgical diagnosis characterized by friability of the superficial fascia, Necrotizing dishwater-gray exudate, and a notable Soft-Tissue absence of pus. Infections N ENGL J MED 2017;377:2253-65. 1 2 Necrotizing fasciitis type I: Necrotizing fasciitis type II ▪ Polymicrobial infection involving aerobic ▪ Often associated with gas in the tissue ▪ A monomicrobial infection. and anaerobic organisms. and thus is difficult to distinguish from gas gangrene ▪ Seen in the elderly or in those with ▪ Among gram-positive organisms, group A streptococcus is the underlying illnesses. ▪ Nonclostridial anaerobic cellulitis and most common pathogen, followed by MRSA. synergistic necrotizing cellulitis are type ▪ Predisposed I variants. Both occur in patients with ▪ May occur in any age group and in those without underlying illness ▪ Diabetic or decubitus ulcers diabetes and typically involve the feet, ▪ Hemorrhoids with rapid extension into the leg ▪ Aeromonas hydrophila (freshwater laceration) ▪ Rectal fissures ▪ Necrotizing fasciitis should be ▪ Vibrio vulnificus (saltwater laceration, ingestion of raw oysters, ▪ Episiotomies considered in patients with systemic cirrhosis) ▪ Colonic or urologic surgery or gynecologic manifestations of sepsis, such as procedures. tachycardia, leukocytosis, acidosis, or ▪ Necrotizing group A streptococcal and clostridial infections are marked hyperglycemia mediated by bacterial exotoxins and the host response ▪ Ludwigs- submandibular ▪ Lemierre’s –thrombophlebitis of jugular ▪ Fournier’s-urethral breach 3 4 Invasive Group A Streptococcal Soft-Tissue Infections Invasive Group A Streptococcal Soft-Tissue Infections (Streptococcus Continued pyogenes) ▪ Infection with a defined portal of bacterial entry: Infection that arises spontaneously in the deep tissue, without an overt wound or lesion: ▪ In 50% of patients with group A streptococcal necrotizing fasciitis or myonecrosis, are without a portal ▪ S. -

Subcutaneous Abscesses and Cellulitis Emily Rothstein, DVM, DACVD
Subcutaneous Abscesses and Cellulitis Emily Rothstein, DVM, DACVD BASIC INFORMATION If the animal is seriously ill, other laboratory tests may be Description recommended to determine what effects the infection is having on A subcutaneous abscess is a collection of pus and infected mate- other organs in the body. rial within the tissues beneath the skin. Cellulitis is an infection or inflammatory reaction that has spread out within these tissues, TREATMENT AND FOLLOW-UP rather than being confined to one pocket. Causes Treatment Options The most common cause is a bacterial infection, although fun- An abscess must often be surgically opened to provide drainage, gal infections and even sterile processes can cause similar signs. and this usually requires general anesthesia or heavy sedation. Bacteria are introduced into the deeper tissues through a wound Sometimes dead tissue is removed, the cavity is flushed with an or injury or by rupture of a hair follicle. (See also the handout antiseptic solution, and a drain is left in place to allow continued for Deep Bacterial Pyoderma and Furunculosis .) Some of the drainage from the site. Cellulitis may be treated with warm, wet more common causes are cat and dog bite wounds, punctures from compresses initially. In some instances, an abscess will form (even thorns, and injuries that cause a break in the skin. with appropriate treatment) that requires surgical drainage. In both situations, antibiotics are given, usually for about 14 days. Clinical Signs Warm, wet compresses are often recommended postoperatively A painful swelling is commonly detected under the skin, and to encourage drainage and provide comfort. -

Bacterial Skin Infections
What is Impetigo? • When treated appropriately, impetigo heals over a • Avoid touching the infected areas and prevent others • Impetigo is a superficial bacterial infection of the few days without leaving scars, although there may from touching them too. skin. be temporary redness and darker pigmentation that • Wash hands after touching affected area. • The most common bacteria causing impetigo is may take weeks or months to resolve. • Wash hands before and after applying creams or Staphylococcus aureus, or “Staph aureus”. Less ointments to the affected area. commonly, it can be caused by another bacteria, How is impetigo diagnosed? • Do not share towels or personal items until the Streptococcus. • Impetigo is diagnosed by the typical appearance and infected area is completely healed. Bacterial Skin • Impetigo is common in young children but can symptoms. • Do not let your child return to school or childcare also affect people of other ages, especially those • A skin swab from the affected area may be taken to facilities until the lesions are dried and healed. Infections with skin that is damaged by cuts, insect bites, or identify the bacteria. eczema. • If the infection recurs, a swab from your child’s nose What is erysipelas/cellulitis? • The bacteria can spread by skin-to-skin contact or by to test for the presence of “Staph aureus” may be • Erysipelas and cellulitis are bacterial infections touching contaminated surfaces such as towels and indicated. affecting deeper layers of skin. clothes. • The most common bacteria causing erysipelas or How is impetigo treated? cellulitis is Streptococcus, but other bacteria may be Treatment depends on the severity and extent of the involved, including Staphylococcus aureus. -

A Study of Various Isolates from Pus Sample with Their Antibiogram from Jln Hospital, Ajmer
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 10 Ver. VI (Oct. 2015), PP 64-68 www.iosrjournals.org A Study of Various Isolates from Pus Sample with Their Antibiogram from Jln Hospital, Ajmer 1Vijeta Sharma, 2Geeta Parihar, 3Vijaylaxmi Sharma, 4Harshita Sharma 1,2,3,4Department of Microbiology, JLN Medical College, Ajmer (Rajasthan) Abstract: This study was conducted in the Department of Microbiology, J. L. N. Medical College, Ajmer (Raj.) for a period of 6 months. A total of randomly 100 pus samples received in the bacteriology section of microbiology department from the various wards of J.L.N Hospital to identify the common aerobic bacterial isolates and to study their antimicrobial susceptibility. Out of 100 culture, 48 (48%) were gram negative and 25 (25%) were gram positive. Mixed growths were seen in 20 (20%) samples and no growth in (7%) cases. The most common organism isolated was Klebsiella (28%) followed by Pseudomonas aeruginosa 20 (20%), Coagulase negative staphylococcus 10 (10%), Staphylococcus aureus 8 (8%), Proteus mirabilis 5 (5%), Enterococcus faecalis 4 (4%), E.coli 3 (3%), Citrobacter 2(2%) and Streptococcus pyogens in 3 (3%) of case. It was observed from that gram positive organisms were sensitive to Gentamicin, Amoxyclav, Linezolid and Vancomycin but resistant to Ampicilline and Cotrimoxazole. For Ciprofloxacin and Erythromycin sensitivity was moderate. Gram negative organisms were sensitive to Amikacin, Imipenem and moderately sensitive to Tetracycline, Ciprofloxacin, Cefotaxime and amoxyclave. Keywords: Wound Samples, Gram negative isolates, Gram positive isolates, antimicrobial sensitivity I. Introduction: Pyogenic infection is characterized by several local inflammation, usually with pus formation, generally caused by one of the pyogenic bacteria, which can produce the accumulation of dead leukocytes and infectious agent commonly known as pus (Koneman etal., 2005). -

Staph Infection Fact Sheet
Staph Infection Fact Sheet What is Staphylococcus aureus (staph)? Staphylococcus aureus, often referred to simply as “staph,” are bacteria commonly carried on the skin or in the nose of healthy people. Approximately 30% of the population is colonized (when bacteria are present, but not causing an infection) in the nose with staph bacteria. Sometimes, staph can cause an infection. Staph bacteria are one of the most common causes of skin infections in the United States. Most of these skin infections are minor and can be treated without antibiotics. However, staph bacteria also can cause serious infections including surgical wound infections, bloodstream infections, and pneumonia. What is MRSA (methicillin-resistant Staphylococcus aureus)? MRSA is a type of staph that is difficult to treat due to its resistant to antibiotics called beta-lactams. Beta-lactam antibiotics include methicillin and other more common antibiotics such as oxacillin, penicillin and amoxicillin. Who gets staph or MRSA infections? Staph infections, including MRSA, occur most frequently among persons in hospitals and healthcare facilities who have weakened immune systems. These healthcare- associated infections include surgical wound infections, urinary tract infections, bloodstream infections, and pneumonia. Staph Infection Fact Sheet What is community-associated MRSA (CA-MRSA)? Staph and MRSA can also cause illness in persons outside of hospitals and healthcare facilities. MRSA infections that are acquired by persons who have not been recently (within the past year) hospitalized or had a medical procedure (such as dialysis, surgery, catheters) are now known as CA-MRSA infections. Staph or MRSA infections in the community are usually manifested as skin infections, such as pimples and boils, and occur in otherwise healthy people.