Hip Abductors and Thigh Muscles Strength Ratios and Their Relation to Electromyography Amplitude During Split Squat and Walking Lunge Exercises
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Intramuscular Injection Is an Injection Given Directly Into The
Depo Lupron and Testosterone are both given by intramuscular injection. The following is a guideline on their administration. Eileen Durham, RN, NP Version 12 Jan 2010 Description Intramuscular (IM) injections are given directly into the central area of selected muscles. There are a number of sites that are suitable for IM injections; there are three sites that are most commonly used in this procedure described below. The volume of viscosity of the medication to be injected determines the site that should be used. IM injections cause stretching of the muscle fiber so the larger the muscle used the less discomfort. Intramuscular Injection Sites Depo Lupron Depo Lupron 3 month preparation should only be injected into the Gluteus medius due to the viscosity and volume of the medication approx. 1.5 – 2 cc. Depo Lupron 1 month preparation can be injection into the vastus lateralis or the gluteus medius. Testosterone Testosterone administered to adolescents and adults can be injected into any of the sites listed below, as long as the volume is 1 cc or less. For a volume of 1.5 use the vastus lateralis or Gluteus medius, if the volume is 2 cc you must you the largest muscle the Gluteus medius. If the volume is greater then 2 cc you must divide the dose and give 2 injections as the maximum volume in the Gluteal muscle is 2 cc. Testosterone administered to infants and toddlers use only the anteriolateral aspect of the thigh. Deltoid muscle The deltoid muscle located laterally on the upper arm can be used for intramuscular injections. -
Bacterial Meningitis and Multiple Abscess Formation in the Iliopsoas
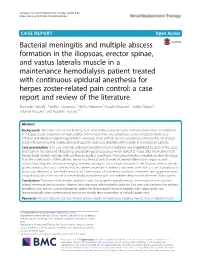
Yamada et al. Renal Replacement Therapy (2018) 4:22 https://doi.org/10.1186/s41100-018-0163-x CASEREPORT Open Access Bacterial meningitis and multiple abscess formation in the iliopsoas, erector spinae, and vastus lateralis muscle in a maintenance hemodialysis patient treated with continuous epidural anesthesia for herpes zoster-related pain control: a case report and review of the literature Shunsuke Yamada1, Narihito Tatsumoto1, Noriko Nakamura1, Kosuke Masutani1, Toshiro Maeda2, Takanari Kitazono1 and Kazuhiko Tsuruya1,3* Abstract Background: Infection is the second leading cause of mortality in patients who undergo maintenance hemodialysis. In this population, impairment in both cellular and humoral immunity contributes to the increased incidence of infection and infection-related hospitalization. However, these artificial devices occasionally enhance the risk of deep organ infection including muscle abscess, frequently leading to disability and mortality in hemodialysis patients. Case presentation: A 54-year-old male undergoing maintenance hemodialysis was hospitalized because of the acute onset pain in the back and bilateral legs and declining consciousness which started at 7 days after the treatment of herpes zoster-related neuralgia with continuous epidural anesthesia. Physical examination revealed purulent discharge from the insertion site of the catheter. Serum biochemical tests showed increased inflammatory response and malnutrition. Magnetic resonance imaging revealed meningitis and multiple abscesses in the iliopsoas, erector spinae, gluteus medius, and vastus lateralis muscles, where conventional antibiotic treatment often fails to cure. Staphylococcus aureus was detected in the cerebrospinal fluid. Combination of intravenous antibiotics treatment and aggressive open surgical drainage of the muscle abscesses finally cured meningitis and multiple deep muscle abscesses in this patient. -

Piriformis Syndrome: the Literal “Pain in My Butt” Chelsea Smith, PTA
Piriformis Syndrome: the literal “pain in my butt” Chelsea Smith, PTA Aside from the monotony of day-to-day pains and annoyances, piriformis syndrome is the literal “pain in my butt” that may not go away with sending the kids to grandmas and often takes the form of sciatica. Many individuals with pain in the buttock that radiates down the leg are experiencing a form of sciatica caused by irritation of the spinal nerves in or near the lumbar spine (1). Other times though, the nerve irritation is not in the spine but further down the leg due to a pesky muscle called the piriformis, hence “piriformis syndrome”. The piriformis muscle is a flat, pyramidal-shaped muscle that originates from the front surface of the sacrum and the joint capsule of the sacroiliac joint (SI joint) and is located deep in the gluteal tissue (2). The piriformis travels through the greater sciatic foramen and attaches to the upper surface of the greater trochanter (or top of the hip bone) while the sciatic nerve runs under (and sometimes through) the piriformis muscle as it exits the pelvis. Due to this close proximity between the piriformis muscle and the sciatic nerve, if there is excessive tension (tightness), spasm, or inflammation of the piriformis muscle this can cause irritation to the sciatic nerve leading to symptoms of sciatica (pain down the leg) (1). Activities like sitting on hard surfaces, crouching down, walking or running for long distances, and climbing stairs can all increase symptoms (2) with the most common symptom being tenderness along the piriformis muscle (deep in the gluteal region) upon palpation. -

Applications of the Pedicled Vastus Lateralis Flap for Patients with Complicated Pressure Sores
Spinal Cord (1997) 35, 437 ± 442 1997 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/97 $12.00 Applications of the pedicled vastus lateralis ¯ap for patients with complicated pressure sores AB Schmidt1, G Fromberg1 and M-H Ruidisch2 1Abt. fuÈr Plastische-, Hand-, Kiefer- und rekonstruktive Mikrochirurgie, BG Unfallklinik Murnau; 2Abt. fuÈr RuÈckenmark- und WirbelsaÈulenverletztungen, BG Unfallklinik Murnau, Germany The vastus lateralis muscle- or musculocutaneous ¯ap is a well established tool in the surgery of pressure sores of the pelvic region. Its size, its constant large axial vascular pedicle originating from the lateral circum¯ex femoral artery, and its ability to carry quite a large skin island from the distal lateral region of the upper thigh makes this ¯ap a very versatile one in the management of dicult situations. The vastus lateralis ¯ap allows the simultaneous closure of defects in the trochanteric and sacral region, a technique which has not been described previously. A pedicled vastus lateralis ¯ap may be the only remaining local salvage procedure for defects due to obstruction of internal and external iliac arteries and aortobifemoral bypass surgery. This is another application which has not yet been described in the medical literature. The outcome of a series of 38 vastus lateralis ¯aps and the complications are shown. The follow-up period ranged from 3 months to 4 years. One ¯ap was lost. More complications were seen at the donor site than at the reconstructed defect. In patients who may be able to walk or stand at a later date, potential impairment of these functions has to be considered. -

Rehabilitation of Soft Tissue Injuries of the Hip and Pelvis T
Donald and Barbara Zucker School of Medicine Journal Articles Academic Works 2014 Rehabilitation of soft tissue injuries of the hip and pelvis T. F. Tyler Northwell Health T. Fukunaga Hofstra Northwell School of Medicine J. Gellert Follow this and additional works at: https://academicworks.medicine.hofstra.edu/articles Recommended Citation Tyler TF, Fukunaga T, Gellert J. Rehabilitation of soft tissue injuries of the hip and pelvis. 2014 Jan 01; 9(6):Article 1396 [ p.]. Available from: https://academicworks.medicine.hofstra.edu/articles/1396. Free full text article. This Article is brought to you for free and open access by Donald and Barbara Zucker School of Medicine Academic Works. It has been accepted for inclusion in Journal Articles by an authorized administrator of Donald and Barbara Zucker School of Medicine Academic Works. INVITED CLINICAL COMMENTARY REHABILITATION OF SOFT TISSUE INJURIES OF THE HIP AND PELVIS Timothy F. Tyler MS, PT, ATC1 Takumi Fukunaga DPT, ATC, CSCS1 Joshua Gellert DPT IJSPT ABSTRACT Soft tissue injuries of the hip and pelvis are common among athletes and can result in significant time loss from sports participation. Rehabilitation of athletes with injuries such as adductor strain, iliopsoas syn- drome, and gluteal tendinopathy starts with identification of known risk factors for injury and comprehen- sive evaluation of the entire kinetic chain. Complex anatomy and overlapping pathologies often make it difficult to determine the primary cause of the pain and dysfunction. The purpose of this clinical commen- tary is to present an impairment-based, stepwise progression in evaluation and treatment of several com- mon soft tissue injuries of the hip and pelvis. -

The Role of and Relationship Between Hamstring and Quadriceps Muscle Myofascial Trigger Points in Patients with Patellofemoral Pain Syndrome
The role of and relationship between Hamstring and Quadriceps muscle myofascial trigger points in patients with patellofemoral pain syndrome. By Karen Louise Frandsen Smith A mini-dissertation submitted in partial compliance with the requirements for the Master’s Degree in Technology: Chiropractic at the Durban University of Technology I, Karen Louise Frandsen Smith, declare that this dissertation is representative of my own work in both conception and execution (except where acknowledgements indicate to the contrary). _______________________ ________________ Karen Louise Frandsen Smith Date Approved for Submission _______________________ ________________ Dr Brian Kruger (supervisor) Date M. Tech. Chiro., C.C.S.P. Dedication I dedicate this work to everyone who loves me and have supported me throughout these years of studying and all the difficult times. It is thanks to you that I have reached my dream. Dad, you would be so proud. i Acknowledgements Thank you to the DUT staff, patients, and supervisor, Dr Brian Kruger for making this happen. Thanks to my class mates for making the years fly by, and creating lifelong memories. This dissertation would not have been completed without supportive, generous and helpful people. Special thanks to you, Dr Danella Lubbe for motivating me and thank you so much Dr Charmaine Korporaal for “picking me up” and helping me finish. Endless gratitude goes to you Damon, Cherine, Mom and Viggo. You are / were all my anchors in the storm, and without your belief in me, I would be nowhere. ii Abstract Purpose: Patellofemoral Pain Syndrome is a common condition in all age groups, with a multi- factorial etiology. -

Effects of a Gluteal Muscles Specific Exercise Program on the Vertical
International Journal of Environmental Research and Public Health Article Effects of a Gluteal Muscles Specific Exercise Program on the Vertical Jump Tomás Gallego-Izquierdo 1, Gerardo Vidal-Aragón 2, Pedro Calderón-Corrales 2, Álvaro Acuña 2, Alexander Achalandabaso-Ochoa 3,* , Agustín Aibar-Almazán 3 , Antonio Martínez-Amat 3 and Daniel Pecos-Martín 1 1 Physiotherapy and Pain Group, Department of Physical Therapy, University of Alcala, 28801 Madrid, Spain; [email protected] (T.G.-I.); [email protected] (D.P.-M.) 2 Physical Therapist, Department of Physical Therapy, University of Alcala, 28801 Madrid, Spain; [email protected] (G.V.-A.); pedrocalderon.fi[email protected] (P.C.-C.); [email protected] (Á.A.) 3 Department of Health Sciences, Faculty of Health Sciences, University of Jaén, 23071 Jaén, Spain.; [email protected] (A.A.-A.); [email protected] (A.M.-A.) * Correspondence: [email protected]; Tel.: +34-953213651 Received: 9 June 2020; Accepted: 23 July 2020; Published: 27 July 2020 Abstract: The vertical jump is a complex movement where many factors are involved in the final result. Currently, how a specific exercise program for gluteal muscles can affect the vertical jump is unknown. So, the aim of this study was to examine the effect of a specific exercise program for the gluteal muscles on a vertical jump. Forty-nine amateur athletes completed an 8-week program. The experimental group received a specific gluteal muscle training program in addition to their regular training routine, whereas the control group received their regular training routine. Jump height, flight time, speed and power were assessed (baseline, postintervention, and 4-week follow-up). -

Myofascial Pain Syndrome of Gluteus Minimus Mimicking Lumbar Radiculitis -A Case Report
Anesth Pain Med 2015; 10: 16-20 http://dx.doi.org/10.17085/apm.2015.10.1.16 ■Case Report■ Myofascial pain syndrome of gluteus minimus mimicking lumbar radiculitis -A case report- Department of Anesthesiology and Pain Medicine, Daegu Fatima Hospital, Daegu, Korea Joong-Ho Park, Kwang-Suk Shim, Young-Min Shin, Chiu Lee, Sang-Gon Lee, and Eun-Ju Kim Myofascial pain syndrome (MPS) can be characterized by pain difficult. Delays in making the correct diagnosis can result in caused by trigger points (TrPs) and fascial constrictions. Patients longer hospital stays, higher hospital fees, and unnecessary with MPS of the gluteus minimus muscles often complain of diagnostic tests and inadequate treatments. The authors have symptoms such as hip pain, especially when standing up after sitting or lying on the affected side, limping, and pain radiating down to successfully diagnosed and treated a patient with MPS of the the lower extremities. A 24-year-old female patient presenting with gluteus minimus initially diagnosed with lumbar radiculitis. motor and sensory impairments of both lower extremities was With thorough physical examination and injection of TrPs referred to our pain clinic after initially being diagnosed with lumbar radiculitis. Under the impression of MPS of the gluteus minimus under ultrasonography guidance, the patient was relieved of her muscles following through evaluation and physical examination of symptoms. We report this case to emphasize the importance of the patient, we performed trigger point injections under ultrasonography physical examination in patients presenting with symptoms guidance on the myofascial TrPs. Dramatic improvement of the suggestive of lumbar radiculitis. -

X X X X X X X X X X Xx X
INJURY PREVENTION THE forward arm swing lean (torso and upper body) x lateral Whole trunk lean x x trunk x rotation hip x extension pelvic drop Body vertical displacement (head to toe) I’m lying facedown on an exam table at a state-of-the-art running clinic in New heel whip York City, about to perform a basic exer- cise for professional analysis. “Okay, Katie, I’d like you to lift your right leg in knee the air, using your glutes,” says Colleen x flexion at mid- Brough, P.T., M.S., the physical therapist stance who’s there to check my strength and x x form. No problem, I think. She places her x hand on my right hamstring—my achy, troublesome one—as I lift and then FIX lower my leg back down to the table with knee Chronically injured and disheartened, x flexion minimal effort and an attitude of That’s cadence at initial contact a Runner’s World editor sought holistic all? “You contracted your hamstring as dynamic well as your back,” Brough says gently. knee alignment help from a team of therapists. Her “Try again, but this time, power the move with your glutes by squeezing your butt diagnosis (sleeping glutes?) and hard- before and while doing the lift.” Okay, got won lessons (master the clamshell!) it. Simple enough. But it isn’t. Impossible, actually. I lie there motionless, slowly can help you, too, stay healthy, happy, coming to the realization that clenching your face doesn’t help you clench your foot initial BODY BREAKDOWN contact and on the road butt cheeks. -

The Absence of Piriformis Muscle, Combined Muscular Fusion, and Neurovascular Variation in the Gluteal Region
Autopsy Case Report The absence of piriformis muscle, combined muscular fusion, and neurovascular variation in the gluteal region Matheus Coelho Leal1 , João Gabriel Alexander1 , Eduardo Henrique Beber1 , Josemberg da Silva Baptista1 How to cite: Leal MC, Alexander JG, Beber EH, Baptista JS. The absence of piriformis muscle, combined muscular fusion, and neuro-vascular variation in the gluteal region. Autops Case Rep [Internet]. 2021;11:e2020239. https://doi.org/10.4322/ acr.2020.239 ABSTRACT The gluteal region contains important neurovascular and muscular structures with diverse clinical and surgical implications. This paper aims to describe and discuss the clinical importance of a unique variation involving not only the piriformis, gluteus medius, gluteus minimus, obturator internus, and superior gemellus muscles, but also the superior gluteal neurovascular bundle, and sciatic nerve. A routine dissection of a right hemipelvis and its gluteal region of a male cadaver fixed in 10% formalin was performed. During dissection, it was observed a rare presentation of the absence of the piriformis muscle, associated with a tendon fusion between gluteus and obturator internus, and a fusion between gluteus minimus and superior gemellus muscles, along with an unusual topography with the sciatic nerve, which passed through these group of fused muscles. This rare variation stands out with clinical manifestations that are not fully established. Knowing this anatomy is essential to avoid surgical iatrogeny. Keywords Anatomic Variation; Anatomy; Buttocks; Muscle; Piriformis Muscle Syndrome. INTRODUCTION The gluteal region contains important Over the years, these variations have been neurovascular and muscular structures that may classified and distributed into different groups. impose diverse clinical and surgical approaches. -

Chapter 10 the Knee Joint
The Knee Joint • Knee joint – largest joint in body Chapter 10 – very complex The Knee Joint – primarily a hinge joint Manual of Structural Kinesiology Modified for Prentice WE: Arnheim’s principles of athletic training , ed 12, New R.T. Floyd, EdD, ATC, CSCS York, 2006, McGraw-Hill; from Saladin, KS: Anatomy &physiology: the unity of forms and function , ed 2, New York, 2001, McGraw- Hill. © 2007 McGraw-Hill Higher Education. All rights reserved. 10-1 © 2007 McGraw-Hill Higher Education. All rights reserved. 10-2 Bones Bones • Enlarged femoral condyles articulate on • Fibula - lateral enlarged tibial condyles – serves as the attachment for • Medial & lateral tibial condyles (medial & knee joint lateral tibial plateaus) - receptacles for structures femoral condyles – does not articulate • Tibia – medial with femur or patella – bears most of weight – not part of knee joint Modified from Anthony CP, Kolthoff NJ: Textbook of anatomy and physiology , ed 9, St. Louis, 1975, Mosby. © 2007 McGraw-Hill Higher Education. All rights reserved. 10-3 © 2007 McGraw-Hill Higher Education. All rights reserved. 10-4 Bones Bones • Patella • Key bony landmarks – sesamoid (floating) bone – Superior & inferior patellar poles – imbedded in quadriceps – Tibial tuberosity & patellar tendon – Gerdy’s tubercle – serves similar to a pulley – Medial & lateral femoral in improving angle of condyles pull, resulting in greater – Upper anterior medial tibial mechanical advantage in surface – Head of fibula knee extension Modified from Anthony CP, Kolthoff NJ: Textbook of anatomy and physiology , ed 9, St. Louis, 1975, Mosby. © 2007 McGraw-Hill Higher Education. All rights reserved. 10-5 © 2007 McGraw-Hill Higher Education. All rights reserved. -
Gluteal Region and Back of Thigh Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Gluteal Region and Back of Thigh Doctors Notes Notes/Extra explanation Editing File Objectives Know contents of gluteal region: Groups of Glutei muscles and small muscles (Lateral Rotators). Nerves & vessels. Foramina and structures passing through them as: 1-Greater Sciatic Foramen. 2-Lesser Sciatic Foramen. Back of thigh : Hamstring muscles. Movements of the lower limb Hip = Thigh Knee=Leg Foot=Ankle Flexion/Extension Flexion/Extension Flexion/Extension Rotation Adduction/Abduction Inversion/Eversion Contents Of Gluteal Region: Muscles / Nerves / Vessels 1- Muscles: • Glutei: 1. Gluteus maximus. 2. Gluteus medius. 3. Gluteus minimus. Abductors: • Group of small muscles (Lateral Rotators): 1. Gluteus medius. 2. Gluteus minimus. 1.Piriformis. Rotators: 2.Obturator internus 1. Obturator internus. 3.Superior gemellus 2. Quadratus femoris. 4.Inferior gemellus Extensor: 5.Quadratus femoris Gluteus maximus. Contents Of Gluteal Region: Muscles / Nerves / Vessels 2- Nerves (All from Sacral Plexus): 1. Sciatic nerve. 2. Superior gluteal nerve. 3. Inferior gluteal nerve. 4. Post. cutaneous nerve of thigh. 5. Nerve to obturator internus. 6. Nerve to quadratus femoris. 7. Pudendal nerve. Contents Of Gluteal Region: Muscles / Nerves / Vessels 3- VESSELS: (all from internal iliac vessels): 1. Superior gluteal 2. Inferior gluteal 3. Internal pudendal vessels. Greater sciatic foreamen: Greater sciatic notch of hip bone is transformed into foramen by: sacrotuberous (between the sacrum to ischial tuberosity) & sacrospinous (between the sacrum to ischial spine ) Structures passing through Greater sciatic foramen : Nerves: Vessels: Greater sciatic foramen Above 1. Superior gluteal nerves, 2. Superior gluteal piriformis vessels. Lesser sciatic foramen muscle. 3. Piriformis muscle. Belew 4. Inferior gluteal nerves 10.