(A Bladder Chimney) for the Treatment of Severe Neurogenic Vesical Dysfunction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Continent Urostomy Guide
$POUJOFOU6SPTUPNZ(VJEF "QVCMJDBUJPOPGUIF6OJUFE0TUPNZ"TTPDJBUJPOTPG"NFSJDB *OD i4FJ[FUIF 0QQPSUVOJUZw CONTINENT UROSTOMY GUIDE Ilene Fleischer, MSN, RN, CWOCN, Author Patti Wise, BSN, RN, CWOCN, Author Reviewed by: Authors and Victoria A.Weaver, RN, MSN, CETN Revised 2009 by Barbara J. Hocevar, BSN,RN,CWOCN, Manager, ET/WOC Nursing, Cleveland Clinic © 1985 Ilene Fleischer and Patti Wise This guidebook is available for free, in electronic form, from United Ostomy Associations of America (UOAA). UOAA may be contacted at: www.ostomy.org • [email protected] • 800-826-0826 CONTENTS INTRODUCTION . 3 WHAT IS A CONTINENT UROSTOMY? . 4 THE URINARY TRACT . 4 BEFORE THE SURGERY . .5 THE SURGERY . .5 THE STOMA . 7 AFTER THE SURGERY . 7 Irrigation of the catheter(s) 8 Care of the drainage receptacles 9 Care of the stoma 9 Other important information 10 ROUTINE CARE AT HOME . 10 Catheterization schedule 11 How to catheterize your pouch 11 Special considerations when catheterizing 11 Care of the catheter 12 Other routine care 12 HELPFUL HINTS . .13 SUPPLIES FOR YOUR CONTINENT UROSTOMY . 14 LIFE WITH YOUR CONTINENT UROSTOMY . 15 Clothing 15 Diet 15 Activity and exercise 15 Work 16 Travel 16 Telling others 17 Social relationships 17 Sexual relations and intimacy 17 RESOURCES . .19 GLOSSARY OF TERMS . 20 BIBLIOGRAPHY . .21 1 INTRODUCTION Many people have ostomies and lead full and active lives. Ostomy surgery is the main treatment for bypassing or replacing intestinal or urinary organs that have become diseased or dysfunctional. “Ostomy” means opening. It refers to a number of ways that bodily wastes are re-routed from your body. A urostomy specifi cally redirects urine. -

Suprapubic Cystostomy: Urinary Tract Infection and Other Short Term Complications A.T
Suprapubic Cystostomy: Urinary Tract Infection and other short term Complications A.T. Hasan,Q. Fasihuddin,M.A. Sheikh ( Department of Urological Surgery and Transplantation, Jinnah Postgraduate Medical Center, Karachi. ) Abstract Aims: To evaluate the frequency of urinary tract infection in patients with suprapubic cystostomy and other complications of the procedure within 30 days of placement. Methods: Patients characteristics, indication and types of cystostomy and short term (within 30 days); complications were analyzed in 91 patients. Urine analysis and culture was done in all patients to exclude those with urinary tract infection. After 15 and 30 days of the procedure, urine analysis and culture was repeated to evaluate the frequency of urinary tract infection. The prevalence of symptomatic bacteriuria with its organisms was assessed. Antibiotics were given to the postoperative and symptomatic patients and the relationship of antibiotics on the prevention of urinary tract infection was determined. Results: Of the 91 cases 88 were males and 3 females. The mean age was 40.52 ± 18.95 with a range of 15 to 82 years.Obstructive uropathy of lower urinary tract.was present in 81% cases and 17(18.6%) had history of trauma to urethra. All these cases had per-urethral bleeding on examination while x-ray urethrogram showed grade H or grade III injury of urethra. Eighty two of the procedures were performed per-cutaneously and 7 were converted to open cystostomies due to failure of per-cutaneous approach. Nine patients had exploratory laparotomy. Duration of catheterization was the leading risk factor for urinary tract infection found in 24.1% at 15 days and 97.8% at 30 days. -
Cystectomy (Bladder Removal) with Ileal Conduit Urinary Diversion
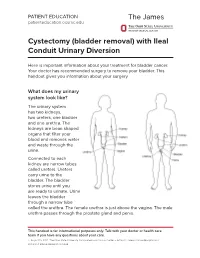
PATIENT EDUCATION patienteducation.osumc.edu Cystectomy (bladder removal) with Ileal Conduit Urinary Diversion Here is important information about your treatment for bladder cancer. Your doctor has recommended surgery to remove your bladder. This handout gives you information about your surgery. What does my urinary system look like? The urinary system has two kidneys, two ureters, one bladder and one urethra. The kidneys are bean shaped organs that filter your blood and removes water and waste through the urine. Connected to each kidney are narrow tubes called ureters. Ureters carry urine to the bladder. The bladder stores urine until you are ready to urinate. Urine leaves the bladder through a narrow tube called the urethra. The female urethra is just above the vagina. The male urethra passes through the prostate gland and penis. This handout is for informational purposes only. Talk with your doctor or health care team if you have any questions about your care. © August 19, 2021. The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute. Cystectomy (bladder removal) with Ileal Conduit Urinary Diversion A cystectomy is surgery to remove the bladder. In men, the prostate, seminal vesicles and lymph nodes may also be removed. In women, the ovaries, fallopian tubes, uterus, cervix, vagina, urethra and lymph nodes may be removed. Your doctor will talk with you about the surgery and what is best for you. After the bladder is removed, your doctor will make a new urinary system. One option is an ileal conduit, also called a urostomy. This will direct your urine to drain through a small opening in your abdomen (belly) called a “stoma”. -

Complications of Urinary Diversion
Complications of Urinary Diversion Jennifer L. Dodson, M.D. Department of Urology Johns Hopkins University Types of Diversion Conduit Diversions Ileal conduit Colon conduit Continent Diversions Continent catheterizable reservoir Continent rectal pouch 1 Overview of Complications Mechanical Stoma problems Bowel obstruction Ureteral obstruction Reservoir perforation Metabolic Altered absorption Altered bone metabolism Growth delay Stones Cancer Conduit Diversions Ileal Conduit: Technically simplest Segment of choice Colon Conduit: Transverse or sigmoid Used when ileum not appropriate (eg: concomitant colon resection, abdominal radiation, short bowel syndrome, IBD) Early complications (< 30 days): 20-56% Late complications : 28-81% Risks: abdominal radiation abdominal surgery poor nutrition chronic steroids Farnham & Cookson, World J Urol, 2004 2 Complications of Ileal Conduit Campbell’s Urology, 8th Edition, 2002 Conduit: Bowel Complications Paralytic ileus 18-20% Conservative management vs NGT Consider TPN Bowel obstruction 5-10% Causes: Adhesions, internal hernia Evaluation: CT scan, Upper GI series Anastomotic leak 1-5 % Risk factors: bowel ischemia, radiation, steroids, IBD, technical error Prevention: Pre-operative bowel prep Attention to technical detail Stapled small-bowel Anastomosis (Campbell’s Blood supply, tension-free anastomosis, Urology, 8th Ed, 2004) realignment of mesentery Farnham & Cookson, World J Urol, 2004 3 Conduit Complications Conduit necrosis: Acute ischemia to bowel -
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a pouch on a person’s abdomen (belly). It is performed for people who have otherwise untreatable urinary incontinence (leakage) chronic urinary infections, or dangerous bladder conditions that may damage kidney function. The goal of these procedures is to improve a person’s long term health and quality of life. What is a stoma? A stoma is the end of the urinary diversion that protrudes through your abdominal wall. The stoma is red, moist, soft, and has no nerve endings. A pouch is placed around the stoma to collect the urine. You will meet with an enterostomal therapy nurse prior to surgery to find the optimal location for the stoma on your abdomen, provide education regarding stoma and skin management, and show you samples of the ostomy pouches that may be used over your stoma after surgery. What is done during the surgery? A urinary diversion surgery is performed in the operating room under general anesthesia (you are not awake for the procedure). The procedure can take 3 to 5 hours, depending on the complexity. Types of urinary diversions: 1. Ileovesicostomy. Department of Urology 734-936-7030 - 1 - In this procedure, the surgeon isolates a 15cm segment of intestine (ileum) from the GI tract. The bowels are then reconnected so that you will still have regular bowel movements, if you had regular movements before. A small hole is made in the bladder and the isolated segment is then sewn to the bladder. -
Urinary Sample Collection Methods in Ileal Conduit Urinary Diversion Patients a Randomized Control Trial Markku H
Ostomy Care Ostomy Care J Wound Ostomy Continence Nurs. 2018;45(1):59-62. Published by Lippincott Williams & Wilkins Urinary Sample Collection Methods in Ileal Conduit Urinary Diversion Patients A Randomized Control Trial Markku H. Vaarala ABSTRACT PURPOSE: The purpose of this study was to compare bacteriological urinalysis findings using 3 urinary sample collection methods (clean stoma catheterization, urine dripping from the stoma, urine collected from the clean urostomy pouch) in ileal conduit urinary diversion patients. DESIGN: Randomized controlled trial. SAMPLE AND SETTING: Twenty-seven patients with ileal conduit urinary diversion from an outpatient urology clinic were enrolled; 9 patients were seen twice, for a total of 36 subjects and comparisons. METHODS: Data were collected during a clinic visit by a trained research nurse. Patients were randomized into 2 groups: group A had the first urine sample collected by clean stoma catheterization, followed by sample collection by urine dripping from the stoma; group B had the first urine sample collection by urine dripping from the stoma, followed by sample collected by clean stoma catheterization. All patients had a third urine sample collected from a factory-clean urostomy pouch. Bacteriological urinalysis findings were compared among methods. Descriptive analyses were summarized using mean, percentage, and frequency. The mean ages of the patients between the groups were compared with the t test. Other between-group comparisons were performed using the Fisher exact test. Urinary culture finding differences among the same patients were evaluated using the McNemar test. Sensitivity and specificity of the different urine sample collection methods were calculated assuming urine sample collection by catheterization as a reference method. -
Continent Urinary Reservoirs and Bladder Substitutes.Pdf
������������������ ��������������� ������������������� �������������������� ���������������� ��������������������� Continent Cutaneous Urinary Reservoirs and Bladder Substitutes Anatomy The bladder is an organ in the pelvis that collects, stores and expels urine. Urine is produced by the kidneys and travels down two tube-like structures called the ureters. The ureters connect the kidneys to the bladder. Urine leaves the bladder through another tube-like structure called the urethra. (Figure 1) Removal of the bladder (cystectomy) may be necessary in some people with bladder cancer, congenital disor- ders of the urinary tract, and in some people who have suffered surgical, traumatic or neurologic damage to the bladder. In these situations, another method of col- lecting and excreting urine must be found. The most common and easiest method for urinary diversion is to use a short piece of intestine as the connection between the ureters and the outside of the body (ileal or colon conduit). This type of diversion is easy for the patient to manage and has a low rate of complication. However, an ostomy bag must be worn at all times to collect urine. Newer surgical techniques are available which do not require the patient to wear an ostomy bag. These newer proce- dures involve creation of a continent urinary reser- voir that collects and stores urine. What is a Continent Urinary Reservoir and How is it Made? A continent urinary reser- voir is an internal “pouch” made from segments of the intestine. Urinary reservoirs can be made from small intestine alone, large intestine alone or from a combination of the above. (Figure 2) The bowel segments selected for use are disconnected from the remainder of the intestinal tract to avoid mixing the gastrointestinal contents (feces) with urine. -

A Patient Guide to Urinary Diversions This Information Will Help You Understand Your Surgical Procedure
Northwestern Memorial Hospital Patient Education CARE AND TREATMENT A Patient Guide to Urinary Diversions This information will help you understand your surgical procedure. It will be a resource for your ostomy care after leaving the hospital. Feel free to write down any questions you may have for To understand your physician and nurse. During your hospital stay, you will be visited by a wound, ostomy how your ostomy and continence (WOC) nurse. This nurse is trained and certified in the care of patients with an ostomy. The WOC nurse will work functions, you with your physician and staff nurses to aid you in your recovery. When you leave the hospital, the WOC nurse will continue to be a need to become resource person for you. familiar with the The urinary system urinary system. To understand how your ostomy functions, you need to become familiar with the urinary system (see Figure 1). The system’s main purpose is to remove urinary waste products from the body. Urine is produced in the kidneys, moves through the ureters and is stored in the bladder until urine is emptied. Urinary diversion – what is it? Sometimes the bladder must be removed or no Figure 1 longer can store urine. In these cases, some type of Kidneys bypass is needed. This is called a urinary diversion. Conditions which may lead to urinary diversion are: ■ Birth defects ■ Trauma ■ Infections ■ Tumors Ureters ■ Other blockages (not managed by conservative measures) There are several types of urinary diversions. The most common, an ileal conduit, involves a section of bowel that Bladder is removed and separated from the gastrointestinal (GI) tract. -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Ureterosigmoidostomy: a Useful Technique
Ureterosigmoidostomy: A Useful Technique Pages with reference to book, From 133 To 135 M. Sajjad Husain, Farakh A. Khan ( Department of Urology Postgraduate Medical Institute, Lahore. ) Abstract Eight patients of bladder extrophy who had ureterosigmoidostomy have been retrospectively analysed. Six patients experienced no postoperative complications. There was no mortality. Open transcolonic mucosa to mucosa proves to be a useful technique of anastomosis. This type of urinary diversion is socially acceptable to Pakistani patients (JPMA 33:13 3, 1983). Introduction Ureterosigmoidostomy was first reported as a procedure for urinary diversion in 1952 by Simon. This attempt was a partial success and posed problems because of infection and leakage at the site of anastomosis. There has been various improvisations since. Coffey (1921). introduced submucosal tunnel to prevent reflux and Nesbit (1949) devised mucosa to mucosa anastomosis to prevent the formation of stricture. Later end to side mucosal anastomosis was described (Cordonnier, 1950). Leadbetter and Clarke (1955) combined the techniques of Coffey and Nesbit. In 1950 ileal conduit was popularised as a procedure for urinary diversion and as a result ureterosigmoidostorny went out of favour (Bricker, 1950). Results of long term Critical evaluation of patients who had ileal conduit diversion were disappointing (Stevens and Eckstein, 1977; Nieh et al., 1978; Jones et al., 1980; Philip et al., 1980; Orr et al., 1981). The pendulum is therefore likely to swing back in favour of a simpler technique i.e. open transcolonic method with formation of submucosal tunnel and direct mucosal anastomosis developed by Goodwin et al.(1953). We report a retrospective review of our experience with open transcolonic method and direct mucosal anastomosis technique in Pakistan. -
1 an Ileal Conduit Urinary Diversion Some Practical Questions
An Ileal Conduit Urinary Diversion Some practical questions & answers with Nancy, a bladder cancer survivor with an Ileal Conduit. An ileal conduit is a system of urinary drainage which a surgeon creates using the small intestine after removing the bladder. To do this, the surgeon takes a short segment of the small intestine and places it at an opening he has made on the surface of the abdomen to create a mouth, or stoma. The ureters, which normally carry urine from the kidneys to the bladder, are then attached to the other end of the segment of intestine. The urine now travels from the kidneys, via the ureters and the newly formed ileal conduit, to the stoma and out into a collecting pouch known as an ostomy bag (or urostomy.) This is worn outside the body around the stoma 24 hours a day. Because the nerves and blood supply are preserved, the new conduit is able to propel the urine out of the body and into the urostomy. Tell us about Recuperation after the Surgery Nancy: One of the advantages of the ileal conduit is that it requires less surgical time than other, more complex, diversions. This procedure was developed during the 1940’s and is still the most used technique for urinary diversion. When I was released from the hospital, I came home with no tubes or catheters. I had no diet restrictions because only a small part of the intestine is used. However, I understand many doctors will recommend a low residue diet for the first few weeks post op. -

Surgical Management of Urolithiasis in Patients After Urinary Diversion
Surgical Management of Urolithiasis in Patients after Urinary Diversion Wen Zhong1, Bicheng Yang1, Fang He2, Liang Wang3, Sunil Swami4, Guohua Zeng1* 1 Department of Urology, the First Affiliated Hospital of Guangzhou Medical University, Guangdong Key Laboratory of Urology, Guangzhou, China, 2 Department of Gynecology and Obstetrics, the Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, China, 3 Department of Biostatistics and Epidemiology, College of Public Health, East Tennessee State University, Johnson, Tennessee, United States of America, 4 Department of Epidemiology, College of Public Health and Health Professions, University of Florida, Gainesville, Florida, United States of America Abstract Objective: To present our experience in surgical management of urolithiasis in patients after urinary diversion. Patients and Methods: Twenty patients with urolithiasis after urinary diversion received intervention. Percutaneous nephrolithotomy, percutaneous based antegrade ureteroscopy with semi-rigid or flexible ureteroscope, transurethral reservoir lithotripsy, percutaneous pouch lithotripsy and open operation were performed in 8, 3, 2, 6, and 1 patients, respectively. The operative finding and complications were retrospectively collected and analyzed. Results: The mean stone size was 4.563.1 (range 1.5–11.2) cm. The mean operation time was 82.0611.5 (range 55–120) min. Eighteen patients were rendered stone free with a clearance of 90%. Complications occurred in 3 patients (15%). Two patients (10%) had postoperative fever greater than 38.5uC, and one patient (5%) suffered urine extravasations from percutaneous tract. Conclusions: The percutaneous based procedures, including percutaneous nephrolithotomy, antegrade ureteroscopy with semi-rigid ureteroscope or flexible ureteroscope from percutaneous tract, and percutaneous pouch lithotripsy, provides a direct and safe access to the target stones in patients after urinary diversion, and with high stone free rate and minor complications.