MS in Focus 6 Intimacy and Sexuality English
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Imperial Tobacco Australia Limited
Imperial Tobacco Australia Limited Submission to the House Standing Committee on Health and Ageing regarding the Inquiry into Plain Tobacco Packaging 22 July 2011 www.imperial-tobacco.com An IMPERIAL TOBACCO GROUP company Registered Office: Level 4, 4-8 Inglewood Place, Norwest Business Park, Baulkham Hills NSW 2153 TABLE OF CONTENTS 1 EXECUTIVE SUMMARY 1 2 COMPANY BACKGROUND 6 3 NO CREDIBLE RESEARCH TO SUPPORT THE INTRODUCTION OF PLAIN PACKAGING 7 4 INCREASED TRADE IN ILLICIT TOBACCO 10 4.1 Combating counterfeit product 11 4.2 Illicit trade impact from unproven regulations 14 4.3 Plain Packaging is not an FCTC obligation 15 4.4 Plain Packaging will place Australia in breach of FCTC obligations 16 5 PLAIN PACKAGING WILL BREACH THE LAW AND INTERNATIONAL TREATIES 19 5.1 Specific Breaches of the TRIPS Agreement 20 5.2 Plain Packaging will breach the Agreement on Technical Barriers to Trade 25 5.3 Breaches of Free Trade Agreements and Bilateral Investment Treaties 27 5.4 Threat to Australia’s reputation 28 6 THE BILL IS UNCONSTITUTIONAL 29 7 NEGATIVE IMPACT ON COMPETITION, CONSUMERS AND RETAILERS 32 7.1 Adverse effects on consumers and retailers 32 7.2 Known effects on businesses and retailers 34 8 INADEQUATE TIME FOR COMPLIANCE 36 8.1 Uncertainty created by incomplete draft Regulations 38 8.2 Previous timelines at introduction of Graphic Health Warnings 2005/6 40 8.3 The Bill and draft Regulations omit important consumer information 41 8.4 Strict Liability and Criminal Penalties 42 9 AUSTRALIA the “NANNY STATE” 43 9.1 Over regulation 43 -

Point-Of-Sale: Tobacco Industry's Last Domain to Fight Bans
POINT‐OF‐SALE: TOBACCO INDUSTRY’S LAST DOMAIN TO FIGHT BANS ON ADVERTISING AND PROMOTIONS Introduction With tobacco advertising and promotions being either totally or partially banned in the mass media in ASEAN, the tobacco industry has shifted its focus to the point-of-sale (POS), it is now the principal avenue for marketing and promoting cigarettes, particularly to vulnerable minors. Cigarette displays at POS are aimed at keeping cigarettes visible and normalizing the product in the public’s mind. POS outlets are ubiquitous, and there is usually no control over their numbers as well as no regulations over what can be sold, which gives the tobacco industry an easy way to make cigarettes easily available. Most countries in the region allow cigarette advertising and promotions at POS. The Philippines and Thailand are licensing the POS outlets. And Thailand is the only ASEAN country that has a comprehensive ban of tobacco industry advertising and promotions at POS that includes a ban of cigarette packs display. Cigarette packs and cartons must be hidden under the cashier’s counter and its display rack and shelves must be covered. SURVEILLANCE Country Current Remarks law/regulation on POS Cambodia Partial ban Enforcement starts in August 2011 Except pack display Indonesia Partial ban Except pack display Lao PDR Partial ban Except pack display INDUSTRY Malaysia Partial ban Except pack display Philippines Partial ban Except pack display Thailand Comprehensive ban Vietnam Partial ban Allows display of only 1 pack or 1 carton per brand Regional industry tactics and trends in POS TOBACCO Marketing channels Cigarettes are sold in POS such as supermarkets, sundry shops, kiosks, newsstands, mobile vans, street vendors, market stalls, minimarts and convenience stores. -

Menthol Content in U.S. Marketed Cigarettes
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Nicotine Manuscript Author Tob Res. Author Manuscript Author manuscript; available in PMC 2017 July 01. Published in final edited form as: Nicotine Tob Res. 2016 July ; 18(7): 1575–1580. doi:10.1093/ntr/ntv162. Menthol Content in U.S. Marketed Cigarettes Jiu Ai, Ph.D.1, Kenneth M. Taylor, Ph.D.1, Joseph G. Lisko, M.S.2, Hang Tran, M.S.2, Clifford H. Watson, Ph.D.2, and Matthew R. Holman, Ph.D.1 1Office of Science, Center for Tobacco Products, United States Food and Drug Administration, Silver Spring, MD 20993 2Tobacco Products Laboratory, National Center for Environmental Health, Centers for Disease Control and Prevention, Atlanta, GA Abstract Introduction—In 2011 menthol cigarettes accounted for 32 percent of the market in the United States, but there are few literature reports that provide measured menthol data for commercial cigarettes. To assess current menthol application levels in the U.S. cigarette market, menthol levels in cigarettes labeled or not labeled to contain menthol was determined for a variety of contemporary domestic cigarette products. Method—We measured the menthol content of 45whole cigarettes using a validated gas chromatography/mass spectrometry method (GC/MS). Results—In 23 cigarette brands labeled as menthol products, the menthol levels of the whole cigarette ranged from 2.9 to 19.6 mg/cigarette, with three products having higher levels of menthol relative to the other menthol products. The menthol levels for 22 cigarette products not labeled to contain menthol ranged from 0.002 to 0.07 mg/cigarette. -

Kohl's Corporation 12 March 2021 Dear Ms. Michelle Gass, We Have the Honour to Address You in Our Capacities As Working Group On
PALAIS DES NATIONS • 1211 GENEVA 10, SWITZERLAND Mandates of the Working Group on the issue of human rights and transnational corporations and other business enterprises; the Special Rapporteur in the field of cultural rights; the Special Rapporteur on minority issues; the Special Rapporteur on freedom of religion or belief; the Special Rapporteur on contemporary forms of slavery, including its causes and consequences; the Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment; and the Special Rapporteur on trafficking in persons, especially women and children REFERENCE: AL OTH 118/2021 12 March 2021 Dear Ms. Michelle Gass, We have the honour to address you in our capacities as Working Group on the issue of human rights and transnational corporations and other business enterprises; Special Rapporteur in the field of cultural rights; Special Rapporteur on minority issues; Special Rapporteur on freedom of religion or belief; Special Rapporteur on contemporary forms of slavery, including its causes and consequences; Special Rapporteur on torture and other cruel, inhuman or degrading treatment or punishment; and Special Rapporteur on trafficking in persons, especially women and children, pursuant to Human Rights Council resolutions 44/15, 37/12, 43/8, 40/10, 42/10, 43/20 and 44/4. We are independent human rights experts appointed and mandated by the United Nations Human Rights Council to report and advise on human rights issues from a thematic or country-specific perspective. We are part of the special procedures system of the United Nations, which has 56 thematic and country mandates on a broad range of human rights issues. -
Tobacco Compliant List by Brand Name ______
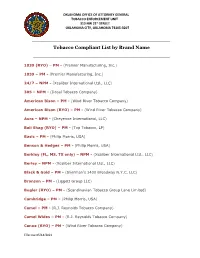
OKLAHOMA OFFICE OF ATTORNEY GENERAL TOBACCO ENFORCEMENT UNIT 313 NW 21st STREET OKLAHOMA CITY, OKLAHOMA 73105-3207 _____________________________________________________________________________ Tobacco Compliant List by Brand Name _________________________________________ 1839 (RYO) – PM - (Premier Manufacturing, Inc.) 1839 – PM - (Premier Manufacturing, Inc.) 24/7 – NPM - (Xcaliber International Ltd., LLC) 305 – NPM - (Dosal Tobacco Company) American Bison – PM - (Wind River Tobacco Company) American Bison (RYO) – PM - (Wind River Tobacco Company) Aura – NPM - (Cheyenne International, LLC) Bali Shag (RYO) – PM - (Top Tobacco, LP) Basic – PM - (Philip Morris, USA) Benson & Hedges – PM - (Philip Morris, USA) Berkley (FL, MS, TX only) – NPM - (Xcaliber International Ltd., LLC) Berley – NPM - (Xcaliber International Ltd., LLC) Black & Gold – PM - (Sherman’s 1400 Broadway N.Y.C. LLC) Bronson – PM - (Liggett Group LLC) Bugler (RYO) – PM - (Scandinavian Tobacco Group Lane Limited) Cambridge – PM – (Philip Morris, USA) Camel – PM - (R.J. Reynolds Tobacco Company) Camel Wides – PM - (R.J. Reynolds Tobacco Company) Canoe (RYO) – PM - (Wind River Tobacco Company) Effective 05/14/2021 Capri – PM - (R.J. Reynolds Tobacco Company) Carlton – PM - (R.J. Reynolds Tobacco Company) Carnival – NPM - (KT&G Corporation) Chesterfield – PM - (Philip Morris, USA) Cheyenne – NPM - (Cheyenne International, LLC) Cigarettellos – PM - (Sherman’s 1400 Broadway N.Y.C. LLC) Classic – PM - (Sherman’s 1400 Broadway N.Y.C. LLC) Commander – PM - (Philip Morris, USA) Crowns – PM - (Commonwealth Brands, Inc.) DTC – NPM - (Dosal Tobacco Company) Dave’s – PM - (Philip Morris, USA) Decade – NPM - (Cheyenne International, LLC) Doral – PM - (R.J. Reynolds Tobacco Company) Drum (RYO) – PM - (Top Tobacco, LP) Dunhill International – PM - (R.J. Reynolds Tobacco Company) Dunhill – PM - (R.J. Reynolds Tobacco Company) Eagle 20's – PM - (Liggett Group LLC) * Vector Tobacco Inc. -

Vaping and E-Cigarettes: Adding Fuel to the Coronavirus Fire?
Vaping and e-cigarettes: Adding fuel to the coronavirus fire? abcnews.go.com/Health/vaping-cigarettes-adding-fuel-coronavirus-fire/story By Dr. Chloë E. Nunneley 26 March 2020, 17:04 6 min read Vaping and e-cigarettes: Adding fuel to the coronavirus fire?Because vaping can cause dangerous lung and respiratory problems, experts say it makes sense that the habit could aggravate the symptoms of COVID-19. New data released by the Centers for Disease Control and Prevention last week warns that young people may be more impacted by COVID-19 than was initially thought, with patients under the age of 45 comprising more than a third of all cases, and one in five of those patients requiring hospitalization. Although scientists still don’t have good data to explain exactly why some young people are getting very sick from the novel coronavirus, some experts are now saying that the popularity of e-cigarettes and vaping could be making a bad situation even worse. Approximately one in four teens in the United States vapes or smokes e-cigarettes, with the FDA declaring the teenage use of these products a nationwide epidemic and the CDC warning about a life-threatening vaping illness called EVALI, or “E-cigarette or Vaping- Associated Lung Injury.” Public health experts believe that conventional cigarette smokers are likely to have more serious illness if they become infected with COVID-19, according to the World Health Organization. Because vaping can also cause dangerous lung and respiratory problems, 1/4 experts say it makes sense that the habit could aggravate the symptoms of COVID-19, although they will need longer-term studies to know for sure. -

Office of Tobacco Control Annual Report 2016
2016 ANNUAL REPORT MISSISSIPPI STATE DEPARTMENT OF HEALTH OFFICE OF TOBACCO CONTROL table of contents Introduction..............................................................................................................page 3 Overview....................................................................................................................page 4 Mission + Values.....................................................................................................page 5 Infrastructure, Administration, and Management...........................................page 6 Economic Impact...................................................................................................page 12 Tobacco Tax Revenue...........................................................................................page 16 Adult Tobacco Data..............................................................................................page 20 Statewide Interventions........................................................................................page 24 Cessation Services................................................................................................page 27 Community Interventions....................................................................................page 29 Youth Tobacco Data..............................................................................................page 31 Youth Programs.....................................................................................................page 36 Mass Reach Health Communication -
Edition 1.0 2/40 TKM60P User's Manual
Edition 1.0 2/40 TKM60P User’s manual 0. Preliminary information .................................................................................................. 4 0.1. SYMBOLS AND CONVENTIONS USED IN THIS MANUAL.................................................................. 4 0.2. INDEX OF REVISIONS........................................................................................................................... 4 1. Introduction...................................................................................................................... 5 1.1. Incremental and absolute encoders ........................................................................................................ 5 1.2. Mechanical assembly.............................................................................................................................. 5 1.3. The TKM60P absolute encoder .............................................................................................................. 6 2. The TKM60P encoder ...................................................................................................... 7 2.1. Technical characteristics......................................................................................................................... 7 2.2. Electrical characteristics.......................................................................................................................... 8 2.3. Mechanical characteristics ..................................................................................................................... -

Action Needed: E-Cigarettes
ACTION NEEDED: E-CIGARETTES Since their introduction in 2008, e-cigarettes have become both ubiquitous and an increasing source of public policy concern and debate. This concern stems primarily from drastic increases in youth e-cigarette use. The most recent data show that 27.5% of high schoolers are using these products — a rate of youth tobacco product use not seen in nearly two decades. The public health community, parents and educators are shocked and worried to find their children and students using these products at home and even in class. Young people are reporting severe signs of dependence, E-cigarettes are now threatening including using e-cigarettes when they first wake up, inability to concentrate in the classroom without to undo all the progress that the using an e-cigarette, and even waking in the night public health community and to get a nicotine fix. government have made over decades We have known for decades that youth in particular to reduce cigarette smoking should not be exposed to nicotine because it changes brain chemistry to create a stronger addiction, can lead to memory and concentration Current generation of e-cigarettes problems, and can make youth who use it more susceptible to addiction to other substances. Research also suggests that young people who use e-cigarettes are four times more likely to go on to smoke combustible cigarettes. E-cigarettes are now threatening to undo all the progress that the public health community and JUUL government have made over decades to reduce cigarette smoking. Indeed, the surgeon general raised the alarm by issuing an advisory declaring a youth e-cigarette epidemic in December 2018. -
Tobacco Compliant List by Brand Name ______
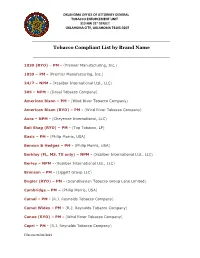
OKLAHOMA OFFICE OF ATTORNEY GENERAL TOBACCO ENFORCEMENT UNIT 313 NW 21st STREET OKLAHOMA CITY, OKLAHOMA 73105-3207 _____________________________________________________________________________ Tobacco Compliant List by Brand Name _________________________________________ 1839 (RYO) – PM - (Premier Manufacturing, Inc.) 1839 – PM - (Premier Manufacturing, Inc.) 24/7 – NPM - (Xcaliber International Ltd., LLC) 305 – NPM - (Dosal Tobacco Company) American Bison – PM - (Wind River Tobacco Company) American Bison (RYO) – PM - (Wind River Tobacco Company) Aura – NPM - (Cheyenne International, LLC) Bali Shag (RYO) – PM - (Top Tobacco, LP) Basic – PM - (Philip Morris, USA) Benson & Hedges – PM - (Philip Morris, USA) Berkley (FL, MS, TX only) – NPM - (Xcaliber International Ltd., LLC) Berley – NPM - (Xcaliber International Ltd., LLC) Bronson – PM - (Liggett Group LLC) Bugler (RYO) – PM - (Scandinavian Tobacco Group Lane Limited) Cambridge – PM – (Philip Morris, USA) Camel – PM - (R.J. Reynolds Tobacco Company) Camel Wides – PM - (R.J. Reynolds Tobacco Company) Canoe (RYO) – PM - (Wind River Tobacco Company) Capri – PM - (R.J. Reynolds Tobacco Company) Effective 06/01/2021 Carlton – PM - (R.J. Reynolds Tobacco Company) Carnival – NPM - (KT&G Corporation) Chesterfield – PM - (Philip Morris, USA) Cheyenne – NPM - (Cheyenne International, LLC) Crowns – PM - (Commonwealth Brands, Inc.) DTC – NPM - (Dosal Tobacco Company) Decade – NPM - (Cheyenne International, LLC) Doral – PM - (R.J. Reynolds Tobacco Company) Drum (RYO) – PM - (Top Tobacco, LP) Dunhill -

Taryield Brand Nicotine Yield CO Yield 1 SILK CUT SILVER KING SIZE 0.1 1 1 MAYFAIR FINE 0.1
file:///J|/eattree/special_licence/6737/mrdoc/pdf/code_frames/cig09.txt UK Data Archive Study Number SN 6716 - General Lifestyle Survey: Secure Access TarYield Brand Nicotine Yield CO Yield 1 SILK CUT SILVER KING SIZE 0.1 1 1 MAYFAIR FINE 0.1 1 2 LAMBERT & BUTLER WHITE 0.2 1 3 MARLBORO KING SIZE (SILVER) 0.3 3 3 SILK CUT BLUE KING SIZE 0.3 3 3 SUPERKINGS WHITE 0.4 3 4 SILK CUT MENTHOL KING SIZE 0.4 5 5 PALL MALL ORANGE 0.5 5 5 RICHMOND KING SIZE MENTHOL 0.4 5 5 LAMBERT & BUTLER GOLD 0.4 5 5 LAMBERT & BUTLER MENTHOL 0.5 5 5 RICHMOND SMOOTH KING SIZE 0.4 6 5 SILK CUT PURPLE KING SIZE 0.5 5 5 JPS KING SIZE WHITE 0.5 6 5 SILK CUT 100S 0.5 6 5 MAYFAIR MENTHOL KING SIZE 0.6 6 5 SUPREME SUPERKINGS WHITE 0.5 5 5 MAXIM SUPERKINGS GOLD 0.5 5 5 BALMORAL SUPERKINGS BLUE 0.5 5 6 LONDIS SUPERKINGS WHITES 0.5 6 6 MARLBORO KING SIZE (GOLD) 0.5 6 6 PARK ROAD SUPERKINGS BLUE 0.6 6 6 NATURAL AMERICAN SPIRIT (YELLOW) 0.7 6 6 SKY WHITE SUPERKINGS 0.5 5 6 JPS KING SIZE GREEN 0.5 6 6 WARWICK SUPERKINGS WHITE 0.5 5 6 BALMORAL KING SIZE BLUE 0.5 7 6 WINSTON BLUE KING SIZE 0.5 7 6 SILK CUT SUPER SLIM 0.7 5 6 MARLBORO MENTHOL KING SIZE 0.5 7 6 CAMEL BLUE 0.5 7 6 JPS KING SIZE SILVER 0.5 7 6 SILK CUT SLIMS PURPLE 0.6 7 6 ROTHMANS ROYALS KING SIZE (BLUE) 0.6 6 6 DORCHESTER SUPERKINGS SMOOTH 0.6 7 6 RED BAND SUPERKINGS WHITE 0.5 6 6 SILK CUT SUPER SLIM MENTHOL 0.7 5 6 DORCHESTER SUPERKINGS MENTHOL 0.6 6 6 WINDSOR BLUE KING SIZE SMOOTH 0.5 7 6 RONSON SUPERKINGS SMOOTH 0.6 7 6 DAVIDOFF GOLD 0.6 6 file:///J|/eattree/special_licence/6737/mrdoc/pdf/code_frames/cig09.txt -

Brand Finance Tobacco 50 2017
Tobacco 50 2017 The annual report on the world’s most valuable tobacco brands March 2017 Foreword Contents steady downward spiral of poor communication, Foreword 2 wasted resources and a negative impact on the bottom line. Definitions 4 Methodology 6 Brand Finance bridges the gap between the marketing and financial worlds. Our teams have Executive Summary 8 experience across a wide range of disciplines from market research and visual identity to tax and Full Table 11 accounting. We understand the importance of design, advertising and marketing, but we also Understand Your Brand’s Value 12 believe that the ultimate and overriding purpose of How We Can Help 14 brands is to make money. That is why we connect brands to the bottom line. Contact Details 15 By valuing brands, we provide a mutually intelligible language for marketers and finance teams. David Haigh, CEO, Brand Finance Marketers then have the ability to communicate the What is the purpose of a strong brand; to attract significance of what they do and boards can use customers, to build loyalty, to motivate staff? All the information to chart a course that maximises true, but for a commercial brand at least, the first profits. answer must always be ‘to make money’. Without knowing the precise, financial value of an asset, how can you know if you are maximising your Huge investments are made in the design, launch returns? If you are intending to license a brand, how and ongoing promotion of brands. Given their can you know you are getting a fair price? If you are potential financial value, this makes sense.