Radiological Protection in Cone Beam Computed Tomography
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
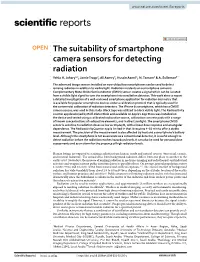
The Suitability of Smartphone Camera Sensors for Detecting Radiation Yehia H
www.nature.com/scientificreports OPEN The suitability of smartphone camera sensors for detecting radiation Yehia H. Johary1,2, Jamie Trapp2, Ali Aamry3, Hussin Aamri4, N. Tamam5 & A. Sulieman6* The advanced image sensors installed on now-ubiquitous smartphones can be used to detect ionising radiation in addition to visible light. Radiation incidents on a smartphone camera’s Complementary Metal Oxide Semiconductor (CMOS) sensor creates a signal which can be isolated from a visible light signal to turn the smartphone into a radiation detector. This work aims to report a detailed investigation of a well-reviewed smartphone application for radiation dosimetry that is available for popular smartphone devices under a calibration protocol that is typically used for the commercial calibration of radiation detectors. The iPhone 6s smartphone, which has a CMOS camera sensor, was used in this study. Black tape was utilized to block visible light. The Radioactivity counter app developed by Rolf-Dieter Klein and available on Apple’s App Store was installed on the device and tested using a calibrated radioactive source, calibration concrete pads with a range of known concentrations of radioactive elements, and in direct sunlight. The smartphone CMOS sensor is sensitive to radiation doses as low as 10 µGy/h, with a linear dose response and an angular dependence. The RadioactivityCounter app is limited in that it requires 4–10 min to ofer a stable measurement. The precision of the measurement is also afected by heat and a smartphone’s battery level. Although the smartphone is not as accurate as a conventional detector, it is useful enough to detect radiation before the radiation reaches hazardous levels. -

As Assessment of the Physics Laboratory, FY 2010
AN ASSESSMENT OF THE NATIONAL INSTITUTE OF STANDARDS AND TECHNOLOGY PHYSICS LABORATORY FISCAL YEAR 2010 Panel on Physics Laboratory Assessments Board Division on Engineering and Physical Sciences THE NATIONAL ACADEMIES PRESS Washington, D.C. www.nap.edu THE NATIONAL ACADEMIES PRESS 500 Fifth Street, N.W. Washington, DC 20001 NOTICE: The project that is the subject of this report was approved by the Governing Board of the National Research Council, whose members are drawn from the councils of the National Academy of Sciences, the National Academy of Engineering, and the Institute of Medicine. The members of the panel responsible for the report were chosen for their special competences and with regard for appropriate balance. This study was supported by Contract No. SB134106Z011, TO#8, between the National Academy of Sciences and the National Institute of Standards and Technology, an agency of the U.S. Department of Commerce. Any opinions, findings, conclusions, or recommendations expressed in this publication are those of the authors and do not necessarily reflect the views of the agency that provided support for the project. International Standard Book Number-13: 978-0-309-16158-9 International Standard Book Number-10: 0-309-16158-4 Copies of this report are available from Laboratory Assessments Board Division on Engineering and Physical Sciences National Research Council 500 Fifth Street, N.W. Washington, DC 20001 Additional copies of this report are available from the National Academies Press, 500 Fifth Street, N.W., Lockbox 285, Washington, DC 20055; (800) 624-6242 or (202) 334-3313 (in the Washington metropolitan area); Internet, http://www.nap.edu. -

Technical Activities 1983: Center for Radiation Research
— a i i lot aboob? NBSIR 84-2848 Technical Activities 1983 Center for Radiation Research U S. DEPARTMENT OF COMMERCE National Bureau of Standards National Measurement Laboratory Center for Radiation Research Washington, DC 20234 February 1984 V o/ w * ^ z \ LxJ ®^EAU 0* U S. DEPARTMENT OF COMMERCE NATIONAL BUREAU OF STANDARDS “QC — 103 . U56 84-2343 1934 NATIONAL F.ITKSA! OF STn.ID.iftDS LIBRARY ^ NBSIR 84-2848 TECHNICAL ACTIVITIES 1983 CENTER FOR RADIATION RESEARCH Randall S. Caswell, Acting Director U S. DEPARTMENT OF COMMERCE National Bureau of Standards National Measurement Laboratory Center for Radiation Research Washington, DC 20234 February 1984 U.S. DEPARTMENT OF COMMERCE, Malcolm Baldrige, Secretary NATIONAL BUREAU OF STANDARDS, Enwit Ambler. Director ABSTRACT This report summarizes research projects, measurement method develop- ment, testing and data evaluation activities, carried out during Fiscal Year 1983 in the NBS Center for Radiation Research. These activities fall in the areas of radiation measurements, atomic and plasma radiation, nuclear radiation, radiation physics, radiometric physics, and radiation sources and instrumentation. Key Words: Atomic radiation; nuclear radiation; plasma radiation; radiation instrumentation; radiation measurements; radiation physics; radiation sources; radiometric physics. i INTRODUCTION This report is a summary of the technical activities of the NBS Center for Radiation Research (CRR) for the period October 1, 1982 to September 30, 1983. The Center is one of five Centers in the National -
Application of Uranium Exploration Data and Techniques in Environmental Studies
1AEA-TECDOC-827 Application of uranium exploration data and techniques in environmental studies Proceedings of a Technical Committee meeting held in Vienna, 9-12 November 1993 WJ INTERNATIONAL ATOMIC ENERGY AGENCY October 1995 The IAEA does not normally maintain stocks of reports in this series. However, microfiche copies of these reports can be obtained from IN IS Clearinghouse International Atomic Energy Agency Wagramerstrasse 5 P.O. Box 100 A-1400 Vienna, Austria Orders should be accompanied by prepayment of Austrian Schillings 100,- in the form of a cheque or in the form of IAEA microfiche service coupons which may be ordered separately from the IN IS Clearinghouse. IAEA-TECDOC-827 Application of uranium exploration data and techniques in environmental studies Proceedings of a Technical Committee meeting held in Vienna, 9-12 November 1993 ffl INTERNATIONAL ATOMIC ENERGY AGENCY /A> The originating Section of this publication in the IAEA was: Nuclear Materials and Fuel Cycle Technology Section International Atomic Energy Agency Wagramerstrasse 5 P.O. Box 100 A-1400 Vienna, Austria APPLICATION OF URANIUM EXPLORATION DATA AND TECHNIQUES IN ENVIRONMENTAL STUDIES IAEA, VIENNA, 1995 IAEA-TECDOC-827 ISSN 1011-4289 © IAEA, 1995 Printed by the IAEA in Austria October 1995 FOREWORD During recent years, the degradation of the environment has become the subject of daily conversation, as well as popular and scientific articles. Usually the concern is man's destruction or alteration of the perceived natural environment. More often than not there is little understanding that the earth's natural environment is largely determined by the underlying geology, and its derivatives, modified by the local biosphere and climatic conditions. -
DIRSIG Water Manual (Version 1.0)
DIRSIG Water Manual (version 1.0) The content contained in this manual has been pulled primarily from chapters of a dissertation (Goodenough 2007), though some limited content from a validation document (Mobley, et al 1993) is included for reference. A recent conference paper demonstrating on-going validation is also included (Speir 2010). Most of the input syntax relevant to users is presented in the third section (“Chapter 5”). The first two sections provide background information on the radiometry and techniques used for the in- water solutions. A section including limited verification/validation is included in the fourth section and additional information is attached covering the original canonical problem set and a brief introduction to additional validation work. Finally, a list of possibly useful references is provided at the end. Chapter 2 Radiometric Foundation of Photon Mapping Contents 2.1 Introduction . 15 2.2 SI Base Units . 16 2.3 Rays and Photons . 16 2.4 Spectral Notation . 18 2.5 Radiometric Terms . 19 2.5.1 Spectral Flux, Φλ .................................... 19 2.5.2 Spectral Radiant Intensity, Iλ .............................. 19 2.5.3 Spectral Irradiance, Eλ ................................. 20 2.5.4 Spectral Radiance, Lλ .................................. 21 2.6 Volumetric Additions . 24 2.7 Radiative Transfer Equation . 25 2.7.1 Inherent Optical Properties . 25 2.7.2 The Integro-Differential Form of the RTE . 29 2.7.3 Solution of a Linear First Order ODE . 30 2.7.4 The Integral Form of the RTE . 32 2.7.5 Practical Form of the RTE . 32 2.8 Computation of the RTE Components . 34 2.1 Introduction Discussion of radiative transfer requires an efficient language that can be used to describe the concepts un- derlying the physical processes. -
Cosmic Rays Editorial
INTERNATIONAL SPACE SCIENCE INSTITUTE No 11, November 2003 Published by the Association Pro ISSI Cosmic Rays Editorial In a deep cave some people have fire lights up in the background Impressum been caught since their early child- casting additional shadows from hood. They are chained down in the unknown objects onto the wall a way that they even cannot turn of our cave. This second fire are their heads around. They can only the cosmic ray particles that reach SPATIUM see shadows on the walls of their us from the depth of the universe. Published bythe inconvenient shelter, which are Apart from the electromagnetic Association Pro ISSI cast by a fire blazing in the back- spectrum,where astronomical ob- twice a year ground. The shadows stem from servations have taken place since objects of unknown form and ma- mankind started looking at the terial carried by some servants. stars, the cosmic rays are inde- INTERNATIONAL SPACE During the years they have given pendent and complementary mes- SCIENCE the shadows names and they inter- sengers from violent processes in INSTITUTE pret them as the real it y. the universe. That is why cosmic Association Pro ISSI rays are such a fascinating topic, Hallerstrasse 6,CH-3012 Bern One of these cave dwellers is able which is still in our days rich of Phone +41 (0)31 631 48 96 to shake-off his chains and leave mysteries. Fax +41 (0)31 631 48 97 the cave. His eyes get dazzled by the light of the Sun at first, but This issue of Spatium is a short President after a while he becomes able to summary of articles edited by the Prof.Heinrich Leutwyler, see all the wonderful objects that International Space Science Insti- University of Bern cast the shadows. -

PHYSICS LABORATORY Technical Activities 1991
NISTIR 4741 U.S. DEPARTMENT OF COMMERCE TECHNOLOGY ADMINISTRATION PHYSICS National Institute of Standards and Technology LABORATORY Submitted to the //4741 1992 DESCRIPTIONS OF COVER ILLUSTRATIONS The molecular structure of the ethylene-ketene weakly bound com- plex is shown as derived from mi- crowave spectroscopy (viewed along The NIST High Accuracy Cryo- the C = C bond of ethylene). The genic Radiometer (HACR) ties opti- geometry shows that the heavy cal power measurements to electri- atoms of the two molecules are cal power measurements, based on crossed at 90 degrees, as predicted the NIST standard volt and ohm. by organic chemists for the cyclo- Each power source causes a tem- addition reaction which produces perature rise on a receiving cavity cyclobutanone. (Molecular Spectros- in the center, which is precisely copy Division) measured and balanced. Cryogenic The building and antennas in the operation, which is not a part of are the short-wave Scanning Electron Microscopy background traditional electrical substitution broadcast facilities for radio station with Polarization Analysis (SEMPA) radiometry, substantially reduces broadcasts time and magnetization images show the WWV which uncertainties and systematic errors. domains in a clean Fe single crystal frequency information to the United The Radiometric Physics Division States. The van in the foreground is whisker (bottom panel), where the relies on the HACR to derive mea- a mobile satellite communication white and black regions denote surement scales in radiometry and magnetization to the right and left terminal used by the Time and photometry. Frequency Division for experiments respectively. The top panel shows on accurate time transfer. One ob- the magnetization in a 2 nm thick jective of this work is the develop- Fe film separated from the Fe whis- ment of a highly accurate satellite ker of the bottom panel by an evap- time service. -

Technical Activities 1982: Center for Radiation Research
5 TA3732 A 11 ID . ... ^ ^ i ecnmcai Activities 1 982 Center for Radiation Research U.S. DEPARTMENT OF COMMERCE National 8ureau of Standards National Measurement Laboratory Center for Radiation Research Washington, DC 20234 February 1983 DEPARTMENT OF COMMERCE )NAL BUREAU OF STANDARDS I I i i NATIONAL BUREAU OF STANDARDS LIBri'.P.Y Mar p | u HC5+ - £ NBSIR 83-2654 too ?3-a?bS TECHNICAL ACTIVITIES 1982 11x3 CENTER FOR RADIATION RESEARCH Chris E. Kuyatt, Director U.S. DEPARTMENT OF COMMERCE National Bureau of Standards National Measurement Laboratory Center for Radiation Research Washington, DC 20234 February 1 983 U.S. DEPARTMENT OF COMMERCE, Malcolm Baldrige, Secretary NATIONAL BUREAU OF STANDARDS, Ernest Ambler. Director I I I I I I I ABSTRACT This report summarizes research projects, measurement method develop- ment, testing and data evaluation activities, carried out during Fiscal Year 1982 in the NBS Center for Radiation Research. These activities fall in the areas of radiation measurements, atomic and plasma radiation, nuclear radiation, radiation physics, radiometric physics, and radiation sources and instrumen- tation. Key Words: Atomic radiation; nuclear radiation; plasma radiation; radiation instrumentation; radiation measurements; radiation physics; radiation sources; radiometric physics. i . INTRODUCTION This report is a summary of the technical activities of the NBS Center for Radiation Research (CRR) for the period October 1, 1981 to September 30, 1982. The Center is one of five Centers in the National Measurement Laboratory. -
Radiation Report
Arafura Resouces Ltd Nolans Environmental Impact Statement volume three P Radiation Report Appendix P Arafura Resources Limited Nolans Project RADIATION REPORT Occupational and Environmental Radiation Measurements and Predictions Prepared for Arafura Resources Limited Nolans Project by Mark Sonter – Radiation Advice & Solutions Pty Ltd Jim Hondros – JRHC Enterprises Pty Ltd March 2016 Page 1 Arafura Resources Limited Nolans Project 1 Executive Summary ................................................................................................................ 4 2 Aim of Report ............................................................................................................................ 5 3 Introduction to Radiation .................................................................................................... 5 4 National & international regime for radiation control .............................................. 6 4.1 Overview ..................................................................................................................................... 6 4.2 ICRP System of Dose Limitation, ALARA, and Regulatory Limits ................................................ 7 4.3 Dose Limitation ........................................................................................................................... 7 5 Natural Background Radiation........................................................................................... 8 5.1 Radiation types and origins ........................................................................................................ -

Mitteilungen S 2014
2014 / mitteilungen S 2014 Special Issue Metrology with Synchrotron Radiation PTB-Mitteilungen Special Issue No. 3–4 Braunschweig and Berlin Physikalisch-Technische Bundesanstalt Physikalisch-Technische Physikalisch-Technische Bundesanstalt Braunschweig and Berlin National Metrology Institute Metrology with Synchrotron Radiation Cover picture (Top) View of the electron storage ring Metrology Light Source (MLS) of PTB in Berlin-Adlershof. (Bottom) The buildings of BESSY II and the MLS. Special Journal for the Economy and Science Official Information Bulletin of the Physikalisch-Technische Bundesanstalt Braunschweig and Berlin Special Issue Volume 124 (2014), No. 3 and 4 Contents Metrology with Synchrotron Radiation • Mathias Richter, Gerhard Ulm: Metrology with Synchrotron Radiation – a Brief Introduction 3 • Roman Klein, Reiner Thornagel, Gerhard Ulm: The Electron Storage Rings MLS and BESSY II as Primary Source Standards 7 • Roman Klein, Rolf Fliegauf, Simone Kroth, Wolfgang Paustian, Mathias Richter, Reiner Thornagel: Source-based Radiometry with Synchrotron Radiation 16 • Alexander Gottwald, Udo Kroth, Michael Krumrey, Peter Müller, Frank Scholze: Detector-based Radiometry with Cryogenic Radiometers and Monochromatized Synchrotron Radiation 21 • Mathias Richter, Alexander Gottwald, Michael Krumrey: Metrology for X-ray Lasers 27 • Alexander Gottwald, Roman Klein, Michael Krumrey, Peter Müller, Wolfgang Paustian, Thomas Reichel, Frank Scholze, Reiner Thornagel: Radiometric Characterization of Space Instrumentation 30 • Michael Krumrey, -

Center for Radiation Research
Center for Radiation Research J -QC 100 October 1986 .1156 # 86-3441 U.S. DEPARTMENT OF COMMERCE National Bureau of Standards 1986 NBS RESEARCH NBSIR 86-3441 INFORMATION CENTER UUO 1 JO Center for Radiation Research Chris E. Kuyatt, Director U.S. DEPARTMENT OF COMMERCE National Bureau of Standards National Measurement Laboratory Center for Analytical Chemistry Gaithersburg, MD 20899 October 1986 U.S. DEPARTMENT OF COMMERCE, Malcolm Baldrige, Secretary National Bureau of Standards, Ernest Ambler, Director ABSTRACT This report summarizes research projects, measurement method development, calibration and testing, and data evaluation activities that were carried out during Fiscal Year 1986 in the NBS Center for Radiation Research. These activities fall in the areas of atomic and plasma radiation, radiation physics, radiometric physics, radiation sources and instrumentation, ionizing radiation, and nuclear physics. Key Words: Atomic radiation, ionizing radiation; measurement support; nuclear radiation; plasma radiation; radiation instrumentation, radiation measurements; radiation physics, radiation sources; radiometric physics. i INTRODUCTION This report is a summary of the technical activities of the NBS Center for Radiation Research (CRR) for the period October 1, 1985 to September 30, 1986. The Center is one of four Centers in the National Measurement Laooratory. The Center for Radiation Research develops and maintains the scientific competences and experimental facilities necessary to provide the Nation with a central basis for uniform