Cornea & External Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -
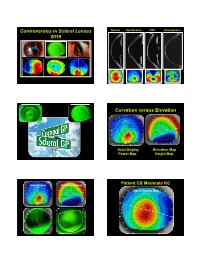
Controversies in Scleral Lenses 2019 Curvature Versus Elevation
Controversies in Scleral Lenses Normal Keratoconus PMD Keratoglobus 2019 Curvature versus Elevation Axial Display Elevation Map Power Map Height Map Axial Display Elevation Display Patient CB Moderate KC Axial Display Map +180um +180 +379 +379um Elevation Display -110 - 276 Elevation Map 655 Above the 290 microns Micron Sphere Height -276um Differential Depression Below the -110um Sphere N = 87 Patients 127 CL Fits Less than 350um Greater than 350um Patients with 350um or less of corneal elevation difference (along the greatest meridian of change) have an 88.2% chance of success with a corneal GP lens. The Re-Birth of Scleral Lenses Glass Scleral Lenses 1887 Molding Glass Scleral Lenses Average 8.5 High DK Scleral Materials Traditional Corneal / Scleral • Menicon Z Dk = 163 Shape • B & L, Boston XO2 DK = 141 • Contamac, Optimum Extreme DK = 125 • B & L, Boston XO DK = 100 • Paragon HDS 100 DK = 100 • Contamac, Optimum Extra DK = 100 • Lagado, Tyro -97 DK = 97 Scleral Shape Cone Angle Circa 1948 Klaus Pfortner New Understandings Argentina Scleral Lens Fitting Objectives Anatomy of a Scleral Lens 1. Central Vault Zone (250 to 400 microns) 2. Peripheral Lift Zone 4 3 2 1 2 3 4 3. Limbal Lift Zone 4. Scleral Landing Zone Ocular Surface Disease Scleral Lens Indications Scleral Irregular Astigmatism Lens • Keratoconus Indications • Pellucid Marginal Degeneration • Post Corneal Trauma • Post keratoplasty • Post K-Pro • Post Refractive Surgery RK, PRK and LASIK • Post HSV and HZV • Athletes • GP stability (rocking) issues Corneal Irregularity -

Peripheral Ring Opacity of the Cornea
Brit. jt. Ophthal. (I969) 53, 270 Br J Ophthalmol: first published as 10.1136/bjo.53.4.270 on 1 April 1969. Downloaded from Peripheral ring opacity of the cornea A. J. BRON Moorfields Eye Hospital, City Road, London, E.C. I A bilaterally symmetrical ring-shaped corneal opacity has been observed in two patients. The condition is described here because of its unusual appearance and because of its appar- ent uniqueness in the literature. Case reports (i) A 59-year-old Caucasian male presented at the casualty department complaining of pricking in the right eye. Symptoms were caused by a marginal infiltrate and this resolved on conventional therapy. A recurrence one month later also responded well. Each cornea presented an arcus senilis and, in the zone ofstroma affected by the arcus, an additional opacity could be seen. This was identical in each eye, and took the form of a striking, narrow, dense white ring in the stroma, passing forwards as a band from Descemet's to Bowman's membrane (Fig. l). copyright. ... ........... http://bjo.bmj.com/ k t_ ; ~~~~~~~~~~~~~~~FI (,GIas I. Drawing of right and left corneae. Insets show slit-lamp sec- tions above and belowv, in the right eye on September 26, 2021 by guest. Protected In slit section, except above, each band appeared as a slender wedge-shaped opacity with its base lying on Descemet's membrane and its apex reaching forwards to Bowman's membrane. The opacity was dense at the base and faint at the apex (Fig. 2, opposite). Between the I I to I o'clock positions, the rings were very faint in each eye and sloped inwards and forwards at an angle in each eye, 450 to the normal on the right and at a shallower angle to the normal on the left. -

Improved Preservation of Human Corneal Basement Membrane
BritishJournal ofOphthalmology 1994; 78: 863-870 863 Improved preservation ofhuman corneal basement membrane following freezing of donor tissue for Br J Ophthalmol: first published as 10.1136/bjo.78.11.863 on 1 November 1994. Downloaded from epikeratophakia Robert D Young, W John Armitage, Paul Bowerman, Stuart D Cook, David L Easty Abstract States, good results continue to be achieved by Current methods for the production of the small number ofBritish surgeons performing lenticules for epikeratophakia involve rapid the technique.4 However, no comprehensive freezing, cryolathing, and slow warming of the account of its long term outcome has yet been donor cornea. We have found that this pro- published. cedure causes structural damage to the Several complications resulting in the failure epithelial basement membrane in the donor of epikeratophakia have been reported, includ- cornea which may subsequently contribute to ing infection, graft dehiscence, persistent inter- poor postoperative re-epithelialisation of the face haze or opacity, ulceration, and imperfect implant, leading to graft failure. Endeavouring re-epithelialisation. Among these, the failure of to overcome these problems, the effects of host epithelial cells to migrate over and re- cryoprotection of donor cornea were investi- surface the anterior face of the grafted tissue gated, using dimethyl sulphoxide, in conjunc- continues to be the major reason for the removal tion with different cooling and warming rates ofepikeratophakia lenticules.'-'0 as part of the protocol for cryolathing. The Epithelial healing is itselfa complex phenome- structural integrity of the epithelial basement non involving mitosis of host cells at the graft membrane zone (BMZ) was then assessed by periphery, centripetal migration, and attach- electron microscopy and by immunofluores- ment. -

An Algorithm to Detect Kayser-Fleischer Ring in Human Eye for Diagnosing Wilson Disease
ISSN: 2319-8753 International Journal of Innovative Research in Science, Engineering and Technology (An ISO 3297: 2007 Certified Organization) Vol. 3, Issue 5, May 2014 An Algorithm to Detect Kayser-Fleischer Ring in Human Eye for Diagnosing Wilson Disease 1S.Tharageshwari, 2 D.Sasikala 1PG scholar, Department Of ECE, Vivekanandha College of Engineering For Women, Namakkal , Tamil nadu, India. 2Associate Professor, Department Of ECE, Vivekanandha College of Engineering For Women, Namakkal, Tamil nadu, India. ABSTRACT-An eye image is segmented by JSEG (J measure based segmentation) algorithm without the manual parameter adjustment and simplifies texture and color for detecting the Kayser-Fleischer ring in diagnosing Wilson Disease. Segmentation with this algorithm passes through two major stages, namely color quantization and spatial segmentation as first stage and region growing and region merging as secondary stage. The biometric measurement provides information on the percentage of the extent of the cornea tissue affected from the copper accumulation. This algorithm detects the presence of symptoms reducing occurrence of false-negative diagnoses and improves accuracy of actual methods used in practice like slit lamp method. The described techniques reduces possible interpretation errors and assists doctor to diagnose the pathology. INDEX TERMS – Wilson disease, Kayser-Fleischer Ring, segmentation, Biometric measurement. I. INTRODUCTION Wilson disease is an autosomal recessive genetic disorder that prevent the body from getting rid of extra copper. A small amount of copper obtained from food is needed to stay healthy, but too much copper is poisonous. When the copper storage capacity of the liver is surpassed, copper is passed into the bloodstream and travels to the other organs-including the brain, kidney, and eyes. -
Cornea Plana Associated with Open-Angle Glaucoma: a Case Report
Cornea plana associated with open-angle glaucoma: a case report Bilge Ozturk Sahin, Goktug Seymenoglu & Esin F. Baser International Ophthalmology The International Journal of Clinical Ophthalmology and Visual Sciences ISSN 0165-5701 Volume 31 Number 6 Int Ophthalmol (2012) 31:505-508 DOI 10.1007/s10792-011-9490-4 1 23 Your article is protected by copyright and all rights are held exclusively by Springer Science+Business Media B.V.. This e-offprint is for personal use only and shall not be self- archived in electronic repositories. If you wish to self-archive your work, please use the accepted author’s version for posting to your own website or your institution’s repository. You may further deposit the accepted author’s version on a funder’s repository at a funder’s request, provided it is not made publicly available until 12 months after publication. 1 23 Author's personal copy Int Ophthalmol (2011) 31:505–508 DOI 10.1007/s10792-011-9490-4 CASE REPORT Cornea plana associated with open-angle glaucoma: a case report Bilge Ozturk Sahin • Goktug Seymenoglu • Esin F. Baser Received: 20 October 2011 / Accepted: 22 November 2011 / Published online: 11 December 2011 Ó Springer Science+Business Media B.V. 2011 Abstract Cornea plana is a rare disease in which the Introduction cornea is flattened with a low refractive power. In addition to these features, hypermetropia, deep central Cornea plana is a rare congenital disease characterized corneal opacities, hazy corneal limbus, peripheral by a flattened corneal curvature and low refractive scleralization of the cornea and early arcus senilis can power. -

Photorefractive Keratectomy for Correction of Epikeratophakia
CASE REPORTS AND SMALL CASE SERIES high myopia resulting from poste- results might be related to the pre- Photorefractive Keratectomy rior lenticonus. Postsurgical refrac- existing corneal stromal abnormali- for Correction of tion was stable for 8 years, then a ties in their patients, which were not Epikeratophakia Regression rapid myopic regression of the epi- observed in our group. Thus, PRK keratophakic lenses was observed can effectively be used to treat epi- Excimer laser photorefractive kera- the following year (Table). In- keratophakic regressed lenses in a se- tectomy (PRK) is widely used for the stead of removing the failed epikera- lected group of patients in whom correction of myopia, astigmatism, tophakic lenses, we performed PRK both the epikeratograft and the sur- and hyperopia.1,2 It has also been on the eyes. rounding cornea are clear. This used for correction of astigmatism method eliminates the need for re- after penetrating keratoplasty.3 Results. Two and a half years after moval of the epikeratograft and ex- Epikeratophakia has been used PRK, the refraction in all 4 eyes is posing the patient to the risks of suc- in the treatment of nontolerant con- stable and the epigrafts are clear. The cessive penetrating keratoplasty. tact lens keratoconous patients.4,5 Table presents the refraction and vi- The epigrafts were made from ma- sual acuity results for the eyes be- Hirsh Ami, MD chined corneal tissue that was found fore PRK and at 3 months, 1 year, Solberg Yoram, MD, PhD unsuitable for penetrating kerato- and 21⁄2 years after PRK. No haze has Cahana Michael, MD plasty. -

ANTERIOR CORNEAL MOSAIC*T by A
Br J Ophthalmol: first published as 10.1136/bjo.52.9.659 on 1 September 1968. Downloaded from Brit. J. Ophthal. (1968) 52, 659 ANTERIOR CORNEAL MOSAIC*t BY A. J. BRON Moorfields Eye Hospital, City Road Branch, London THE corneal anatomy has received intensive study in recent years, but an aspect of its structure which is readily observed clinically has received little attention in the literature. In all normal corneae, after the instillation of fluorescein into the conjunctival sac, a striking mosaic pattern may be observed on the surface of the corneal epithelium after massage of the cornea through the lids. This pattern will be referred to as the anterior corneal mosaic. It was first observed by the author in patients whose eyes had been padded for corneal disease. It was noted in some that a mosaic pattern appeared after the instilla- tion of fluorescein. This pattern disappeared in a short period of time, but could readily be re-induced by pressure on the cornea through the lids. It is the purpose of this paper to describe the characteristics of the anterior corneal mosaic and to discuss its significance. This pattern was studied by Fischer (1928), and has since been re-studied by Schweitzer (1967). Methods Induction of the Mosaic A drop of 2 per cent. fluorescein is instilled into the conjunctival sac and the cornea is viewed with the cobalt beam of the slit lamp. If necessary the fluorescein is diluted to produce a bright fluorescence. A thumb is placed on the upper lid of the eye under examination and with the eye in the straight-ahead position, the lid is moved up and down over the cornea with light or moderate pressure applied to the globe. -

Its Not Just Dry Eye NCOS2021
5/31/21 DISCLOSURES CORNEA ENDOTHELIOPATHIES NOPE, THAT’S NOT JUST DRY EYE: PRIMARY SECONDARY OTHER CORNEAL DISEASES • Corneal guttata • Contact lens wear • Fuchs dystrophy • Surgical procedures • Posterior Polymorphous Dystrophy (PPD) • Age related Cecelia Koetting, OD FAAO • Congenital hereditary endothelial dystrophy • Iatrogenic (im munodeficiency) (CHED) • Glaucoma induced Virginia Eye Consultants • Iridocorneal endothelial syndrome (ICE) • Ocular inflammation Norfolk, VA 1 2 3 OTHER CORNEAL CORNEAL FUNCTION • Keratoconus • Central cloudy dystrophy of Francois • Pellucid marginal degeneration • Thiel-Behnke corneal dystrophy • Shields the eye from germs, dust, other harmful matter • Lattice Dystrophy • Ocular Bullous pemphigoid WHY IS THE CORNEA IMPORTANT? • Contributes between 65-75% refracting power to the eye • Recurrent corneal erosion (RCE) • SJS • Filters out some of the most harmful UV wavelengths • Granular corneal dystrophy • Band Keratopathy • Reis-Bucklers corneal dystrophy • Corneal ulcer • Schnyder corneal dystrophy • HSV/HZO • Congenital Stromal corneal dystrophy • Pterygium • Fleck corneal dystrophy • Burns/Scars • Macular corneal dystrophy • Perforations • Posterior amorphous corneal dystrophy • Vascularized cornea 4 5 6 CORNEAL ANATOMY CORNEA Epithelium Bowmans Layer • Cornea is a transparent, avascular structure consisting of 6 layers • A- Anterior Epithelium: non-keratinized stratified squamous epithelium; cells migrate from BRIEF ANATOMY REVIEW Stroma basal layer upward and periphery to center • B- Bowmans Membrane: -

Cataract Influence on Iris Recognition Performance
Cataract influence on iris recognition performance Mateusz Trokielewicz1,2, Adam Czajka2,1, Piotr Maciejewicz3 1Biometrics Laboratory, Research and Academic Computer Network, Wawozowa 18, 02-796 Warsaw, Poland; 2Institute of Control and Computation Engineering, Warsaw University of Technology, Nowowiejska 15/19, 00-665 Warsaw, Poland; 3Department of Ophthalmology, Medical University of Warsaw, Lindleya 4, 02-005 Warsaw, Poland ABSTRACT This paper presents the experimental study revealing weaker performance of the automatic iris recognition methods for cataract-affected eyes when compared to healthy eyes. There is little research on the topic, mostly incorporating scarce databases that are often deficient in images representing more than one illness. We built our own database, acquiring 1288 eye images of 37 patients of the Medical University of Warsaw. Those images represent several common ocular diseases, such as cataract, along with less ordinary conditions, such as iris pattern alterations derived from illness or eye trauma. Images were captured in near-infrared light (used in biometrics) and for selected cases also in visible light (used in ophthalmological diagnosis). Since cataract is a disorder that is most populated by samples in the database, in this paper we focus solely on this illness. To assess the extent of the performance deterioration we use three iris recognition methodologies (commercial and academic solutions) to calculate genuine match scores for healthy eyes and those influenced by cataract. Results show a significant degradation in iris recognition reliability manifesting by worsening the genuine scores in all three matchers used in this study (12% of genuine score increase for an academic matcher, up to 175% of genuine score increase obtained for an example commercial matcher). -

Bilateral, Anterior Stromal Ring Opacity of the Cornea
Downloaded from bjo.bmj.com on 11 December 2006 Bilateral, anterior stromal ring opacity of the cornea Gerrit R J Melles, Johan P de Séra, Cathrien A Eggink, Johan R M Cruysberg and Perry S Binder Br. J. Ophthalmol. 1998;82;522-525 Updated information and services can be found at: http://bjo.bmj.com/cgi/content/full/82/5/522 These include: References 1 online articles that cite this article can be accessed at: http://bjo.bmj.com/cgi/content/full/82/5/522#otherarticles Rapid responses You can respond to this article at: http://bjo.bmj.com/cgi/eletter-submit/82/5/522 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at the service top right corner of the article Notes To order reprints of this article go to: http://www.bmjjournals.com/cgi/reprintform To subscribe to British Journal of Ophthalmology go to: http://www.bmjjournals.com/subscriptions/ Downloaded from bjo.bmj.com on 11 December 2006 522 Br J Ophthalmol 1998;82:522–525 Bilateral, anterior stromal ring opacity of the cornea Gerrit R J Melles, Johan P de Séra, Cathrien A Eggink, JohanRMCruysberg, Perry S Binder Abstract degenerative changes with advancing age. In Aims/background—To describe a bilat- the current report, we describe the presence of eral, mid peripheral, ring-shaped corneal a bilateral, ring-shaped, mid peripheral corneal opacity, not resembling any known cor- opacification as an isolated finding in a young, neal degeneration, dystrophy, or other healthy patient, who did not have a history of disorder, and occurring without ocular or ocular inflammation. -

Congenital Ocular Anomalies in Newborns: a Practical Atlas
www.jpnim.com Open Access eISSN: 2281-0692 Journal of Pediatric and Neonatal Individualized Medicine 2020;9(2):e090207 doi: 10.7363/090207 Received: 2019 Jul 19; revised: 2019 Jul 23; accepted: 2019 Jul 24; published online: 2020 Sept 04 Mini Atlas Congenital ocular anomalies in newborns: a practical atlas Federico Mecarini1, Vassilios Fanos1,2, Giangiorgio Crisponi1 1Neonatal Intensive Care Unit, Azienda Ospedaliero-Universitaria Cagliari, University of Cagliari, Cagliari, Italy 2Department of Surgery, University of Cagliari, Cagliari, Italy Abstract All newborns should be examined for ocular structural abnormalities, an essential part of the newborn assessment. Early detection of congenital ocular disorders is important to begin appropriate medical or surgical therapy and to prevent visual problems and blindness, which could deeply affect a child’s life. The present review aims to describe the main congenital ocular anomalies in newborns and provide images in order to help the physician in current clinical practice. Keywords Congenital ocular anomalies, newborn, anophthalmia, microphthalmia, aniridia, iris coloboma, glaucoma, blepharoptosis, epibulbar dermoids, eyelid haemangioma, hypertelorism, hypotelorism, ankyloblepharon filiforme adnatum, dacryocystitis, dacryostenosis, blepharophimosis, chemosis, blue sclera, corneal opacity. Corresponding author Federico Mecarini, MD, Neonatal Intensive Care Unit, Azienda Ospedaliero-Universitaria Cagliari, University of Cagliari, Cagliari, Italy; tel.: (+39) 3298343193; e-mail: [email protected].