Aviation Occurrence Statistics 2004 to 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tumut Shire Flood Emergency Sub Plan
Tumut Shire TUMUT SHIRE FLOOD EMERGENCY SUB PLAN A Sub-Plan of the Tumut Shire Council Local Emergency Management Plan (EMPLAN) Volume 1 of the Tumut Shire Local Flood Plan Tumut Shire Local Flood Plan AUTHORISATION The Tumut Shire Flood Emergency Sub Plan is a sub plan of the Tumut Shire Council Local Emergency Management Plan (EMPLAN). It has been prepared in accordance with the provisions of the State Emergency Service Act 1989 (NSW) and is authorised by the Local Emergency Management Committee in accordance with the provisions of the State Emergency and Rescue Management Act 1989 (NSW). November 2013 Vol 1: Tumut Shire Flood Emergency Sub Plan Page i Tumut Shire Local Flood Plan CONTENTS AUTHORISATION .............................................................................................................................................. i CONTENTS ....................................................................................................................................................... ii LIST OF TABLES ............................................................................................................................................... iii DISTRIBUTION LIST ......................................................................................................................................... iv VERSION HISTORY ............................................................................................................................................ v AMENDMENT LIST .......................................................................................................................................... -

Airline and Aircraft Movement Growth “Airports...Are a Vital Part of Ensuring That Our Nation Is Able to Be Connected to the Rest of the World...”
CHAPTER 5 AIRLINE AND AIRCRAFT MOVEMENT GROWTH “AIRPORTS...ARE A VITAL PART OF ENSURING THAT OUR NATION IS ABLE TO BE CONNECTED TO THE REST OF THE WORLD...” THE HON WARREN TRUSS, DEPUTY PRIME MINISTER 5 Airline and aircraft movement growth The volume of passenger and aircraft movements at Canberra Airport has declined since 2009/2010. In 2013/2014 Canberra Airport will handle approximately 2.833 million passengers across approximately 60,000 aircraft movements, its lowest recorded passenger volume since 2007/2008. The prospects for a future return to growth however are strong. Canberra Airport expects a restoration of volume growth in 2015/2016 and retains confidence in the future of the aviation market in Canberra, across Australia, and particularly the Asia Pacific region. Over the next 20 years passenger numbers at Canberra Airport are projected to reach 9 million passengers per annum with some 153,000 aircraft movements in 2033/2034. Canberra Airport, with its extensive infrastructure upgrades in recent years, is well positioned to meet forecast demand with only minor additional infrastructure and capitalise on growth opportunities in the regional, domestic and international aviation markets. 5.1 OVERVIEW Globally, the aviation industry has experienced enormous change over the past 15 years including deregulation of the airline sector, operational and structural changes in the post-September 11 2001 environment, oil price shocks, the collapse of airlines as a result of the global financial crisis (GFC), and the rise of new global players in the Middle East at the expense of international carriers from traditional markets. Likewise, Australia has seen enormous change in its aviation sector – the demise of Ansett, the emergence of Virgin Australia, Jetstar, and Tiger Airways, the subsequent repositioning of two out of three of these new entrant airlines and, particularly in the Canberra context, the collapse of regional airlines. -

Legislative Council
New South Wales Legislative Council PARLIAMENTARY DEBATES (HANSARD) Fifty-Seventh Parliament First Session Thursday, 27 February 2020 Authorised by the Parliament of New South Wales TABLE OF CONTENTS Visitors .................................................................................................................................................... 1925 Visitors ................................................................................................................................................ 1925 Motions ................................................................................................................................................... 1925 Wildlife Carers .................................................................................................................................... 1925 Very Reverend Archimandrite Apostolos Trifyllis ............................................................................ 1925 Ovarian Cancer ................................................................................................................................... 1926 Committees ............................................................................................................................................. 1926 Select Committee on Museums and Galleries .................................................................................... 1926 Establishment and Membership ...................................................................................................... 1926 Motions .................................................................................................................................................. -

Regulamento (Ue) N
11.2.2012 PT Jornal Oficial da União Europeia L 39/1 II (Atos não legislativos) REGULAMENTOS o REGULAMENTO (UE) N. 100/2012 DA COMISSÃO de 3 de fevereiro de 2012 o que altera o Regulamento (CE) n. 748/2009, relativo à lista de operadores de aeronaves que realizaram uma das atividades de aviação enumeradas no anexo I da Diretiva 2003/87/CE em ou após 1 de janeiro de 2006, inclusive, com indicação do Estado-Membro responsável em relação a cada operador de aeronave, tendo igualmente em conta a expansão do regime de comércio de licenças de emissão da União aos países EEE-EFTA (Texto relevante para efeitos do EEE) A COMISSÃO EUROPEIA, 2003/87/CE e é independente da inclusão na lista de operadores de aeronaves estabelecida pela Comissão por o o força do artigo 18. -A, n. 3, da diretiva. Tendo em conta o Tratado sobre o Funcionamento da União Europeia, (5) A Diretiva 2008/101/CE foi incorporada no Acordo so bre o Espaço Económico Europeu pela Decisão o Tendo em conta a Diretiva 2003/87/CE do Parlamento Europeu n. 6/2011 do Comité Misto do EEE, de 1 de abril de e do Conselho, de 13 de Outubro de 2003, relativa à criação de 2011, que altera o anexo XX (Ambiente) do Acordo um regime de comércio de licenças de emissão de gases com EEE ( 4). efeito de estufa na Comunidade e que altera a Diretiva 96/61/CE o o do Conselho ( 1), nomeadamente o artigo 18. -A, n. 3, alínea a), (6) A extensão das disposições do regime de comércio de licenças de emissão da União, no setor da aviação, aos Considerando o seguinte: países EEE-EFTA implica que os critérios fixados nos o o termos do artigo 18. -

Fairbairn Heritage Management Plan March 2010
Fairbairn Heritage Management Plan March 2010 Contents Department of the Environment, Water, Heritage and the Arts, letter dated 26 March 2010. Acknowledging that the Fairbairn Heritage Management Plan is in a form acceptable to the Department of the Environment, Water, Heritage and the Arts, as a Tool for the management of Heritage Values, during the ongoing development and revitalisation of Fairbairn. Management Plan compliance checklist for commonwealth heritage places under the Environment Protection and Biodiversity Conservation Amendment Regulations 2003 (No. 1) Schedule 7A – Management Plans for Commonwealth Heritage Places Schedule 7B – Commonwealth Heritage Management Principles Heritage Management Plan, Former RAAF Base Fairbairn, Canberra Airport, Graham Brooks and Associates Pty Ltd, dated 1 March 2010. MANAGEMENT PLAN COMPLIANCE CHECKLIST FOR COMMONWEALTH HERITAGE PLACES HERITAGE MANAGEMENT PLAN - FORMER RAAF BASE FAIRBAIRN MARCH 2010 Although the former RAAF Base Fairbairn is not yet on the Commonwealth Heritage List (CHL), the compliance tables have been included to ensure that the Heritage Management Plan meets the requirements of the Environment Protection and Biodiversity Conservation Act 1999 should it be listed on the CHL in the future. Environment Protection and Biodiversity Conservation Amendment Regulations 2003 (No. 1) Schedule 7A – Management Plans for Commonwealth Heritage Places Legislation Comment (Refer to) A management plan must: a) establish objectives for the identification, Section 1 Introduction protection, -

Rozporządzenia
6.2.2014 PL Dziennik Urzędowy Unii Europejskiej L 37/1 II (Akty o charakterze nieustawodawczym) ROZPORZĄDZENIA ROZPORZĄDZENIE KOMISJI (UE) NR 100/2014 z dnia 5 lutego 2014 r. zmieniające rozporządzenie (WE) nr 748/2009 w sprawie wykazu operatorów statków powietrznych, którzy wykonywali działalność lotniczą wymienioną w załączniku I do dyrektywy 2003/87/WE Parlamentu Europejskiego i Rady poczynając od dnia 1 stycznia 2006 r. ze wskazaniem administrującego państwa członkowskiego dla każdego operatora statków powietrznych (Tekst mający znaczenie dla EOG) KOMISJA EUROPEJSKA, (3) Celem tego wykazu jest zmniejszenie obciążenia admi nistracyjnego ponoszonego przez operatorów statków powietrznych poprzez udostępnienie informacji o tym, które z państw członkowskich jest regulatorem danego uwzględniając Traktat o funkcjonowaniu Unii Europejskiej, operatora statków powietrznych. (4) Objęcie operatora statków powietrznych unijnym uwzględniając dyrektywę 2003/87/WE Parlamentu Europej systemem handlu uprawnieniami do emisji gazów skiego i Rady z dnia 13 października 2003 r. ustanawiającą cieplarnianych uzależnione jest od wykonywania działal system handlu przydziałami emisji gazów cieplarnianych we ności lotniczej wymienionej w załączniku I do dyrektywy Wspólnocie oraz zmieniającą dyrektywę Rady 96/61/WE ( 1), 2003/87/WE, nie jest natomiast uzależnione od umiesz w szczególności jej art. 18a ust. 3 lit. b), czenia danego operatora w wykazie operatorów statków powietrznych ustanowionym przez Komisję na podstawie art. 18a ust. 3 wspomnianej dyrektywy. -

Annual Report 19
Darwin Alice Springs Tennant Creek A Airport Development Group International Airport Airport Airport Annual Report 19 . Highlights 2018–19 We reached a milestone The National Critical Care In October 2018, Alice Springs of 21 years since the three and Trauma Response Centre received the first of four airports were privatised was completed at Darwin charter flights from Tokyo, under the NT Airports International Airport in Nagoya and Osaka, Japan, in banner, celebrating with April 2019, creating a world- more than 10 years. a special airside premiere class, on-airport Emergency screening of the aviation Medical Retrieval Precinct. history film ‘The Sweet Little Note of the Engine.’ Virgin Australia launched a new three-times-weekly We refurbished an seasonal service to Denpasar, underused part of the Bali, in April 2019. Sustainability reporting Darwin terminal into the introduced. Emissions target ‘Green Room’, a pop-up developed and on track to community arts space, have zero net emissions by launching it in August 2018. SilkAir announced an 2030 (scope 1 and 2). increase in weekly services between Darwin and Singapore from July 2019, Ian Kew, CEO, continued marking its seventh year of Runway overlay works as Chairman of the Darwin operations to Darwin with a commenced in Alice Springs Major Business Group and seventh weekly service. at a value of circa Chairman of the Darwin $20 million. Festival. ADG staff and the company contributed $18,000 to two ‘Happy or Not’ instant community causes from our $1.4 million infrastructure customer feedback Workplace Giving initiative. boost at Tennant Creek platforms installed in Alice for improved fencing and Springs and Darwin. -

COVID-19 UPDATE – 21St January 2021
COVID-19 UPDATE – 21st January 2021 MANDATORY FACE MASKS REQUIRED AT GOVE AIRPORT On Friday 8th January 2021, the Prime Minister announced (National Cabinet agreed) mandatory use of masks in domestic airports and on all domestic commercial flights. Furthermore, the NT Chief Health Officer Directions make it mandatory from the 20th January 2021 for face masks to be worn at all major NT airports and while on board an aircraft. Masks must be worn when inside the airport terminal building and when on the airfield. Children under the age of 12 and people with a specified medical condition are not required to wear a mask. Mask wearing is mandatory at the following Northern Territory airports: • Darwin International Airport • Alice Springs Airport • Connellan Airport - Ayers Rock (Yulara) • Gove Airport • Groote Eylandt A person is not required to wear a mask during an emergency or while doing any of the following: • Consuming food or beverage • Communicating with a person who is hearing impaired. • Wearing an oxygen mask AIRPORT & TRAVELLING • PLEASE NOTE: To reduce the challenges with social distancing and to minimise risks, only Airline passengers will be able to enter the Airport terminal, • please drop-off and pick-up passengers outside of the terminal building It is the responsibility of individuals to make sure they have a mask to wear when at major NT airports and while on board an aircraft. Additional Information: • Please be aware of the NT Government Border Controls, which may be in place https://coronavirus.nt.gov.au/travel/interstate-arrivals • https://www.interstatequarantine.org.au/state-and-territory-border-closures/ • AirNorth schedule - https://www.airnorth.com.au/flying-with-us/before-you-fly/arrivals- and-departures • https://www.cairnsairport.com.au/travelling/airport-guide/covid19/ . -

Low Cost Air Travel Option Between Melbourne and Canberra
ISSUE NO.81 I FEBRUARY 2017 TIGERAIR AUSTRALIA’S NEW CANBERRA SERVICE TOUCHING DOWN ON 8 DECEMBER 2016. LOW COST AIR TRAVEL OPTION BETWEEN MELBOURNE AND CANBERRA TIGERAIR AUSTRALIA CELEBRATED THE AIRLINE’S FIRST FLIGHT BETWEEN MELBOURNE AND (ABOVE) FIRE VEHICLES WELCOMED THE TIGERAIR FLIGHT WITH A CEREMONIAL CANBERRA ON THURSDAY 8 DECEMBER. WATER ARCH SALUTE. (BELOW) STEPHEN BYRON WITH TIGERAIR AUSTRALIA’S ADAM ROWE. Tigerair’s new services will prove timely for Victorians keen for affordable flights to Canberra as the city becomes an increasingly attractive tourism destination due to its rich mix of art, culture, food, exhibitions and world class events. Tigerair Australia said it is pleased to have launched low-cost services between Melbourne and Canberra, providing over 2,500 additional visitor seats every week through Melbourne and Canberra Airports. “The arrival of Tigerair opens up new opportunities to promote the capital to Melbournians and provides people in the Canberra region with a more affordable option of getting to the Victorian capital,” said ACT Chief Minister Andrew Barr. Canberra Airport’s Managing Director, Stephen Byron, echoed Minister Barr’s comments, saying he believed Tigerair’s new services provide a highly attractive option for Victorians to take advantage of the numerous tourism and business opportunities that Canberra has to offer. QATAR AIRWAYS’ NEW DOHA TO CANBERRA ROUTE CANBERRA AIRPORT IS DELIGHTED THAT QATAR AIRWAYS HAS COMMITTED TO A NEW DOHA TO CANBERRA SERVICE. STEPHEN BYRON AND GORDON RAMSEY HAVING A VIRTUAL EXPERIENCE SEARCH FOR BETTONGS. Canberra Airport Executive Chairman, Terry Snow, said Canberra would be Qatar Airways’ fifth destination in Australia. -
Collision with Terrain Involving Cessna 182, VH-KKM, 19 Km WSW Of
InsertCollision document with terrain title involving Cessna 182, VH-KKM Location19 km WSW | Date of Mount Hotham Airport, Victoria | 23 October 2013 ATSB Transport Safety Report Investigation [InsertAviation Mode] Occurrence Occurrence Investigation Investigation XX-YYYY-####AO-2013-186 Final – 16 April 2015 Cover photo: Aircraft owner Released in accordance with section 25 of the Transport Safety Investigation Act 2003 Publishing information Published by: Australian Transport Safety Bureau Postal address: PO Box 967, Civic Square ACT 2608 Office: 62 Northbourne Avenue Canberra, Australian Capital Territory 2601 Telephone: 1800 020 616, from overseas +61 2 6257 4150 (24 hours) Accident and incident notification: 1800 011 034 (24 hours) Facsimile: 02 6247 3117, from overseas +61 2 6247 3117 Email: [email protected] Internet: www.atsb.gov.au © Commonwealth of Australia 2015 Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form license agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. -
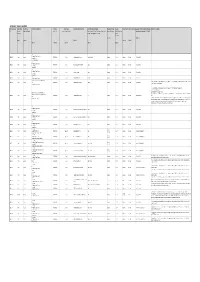
The Table of Services (PDF)
APPENDIX 1: TABLE OF SERVICES Proposed Service Contract type Availability Brief Service Description Airframe Aircraft Type Nominated Operational Base Firebombing Delivery System Passenger Carriage Fuelling Service Period Approximate timing Specimen Contract applicable Schedules Additional Information ID Primary / Absolute / Partial RW / FW Type 1 / Type 2 / Type 3 Tank / Bucket / (Bucket) / Long line bucket / Tank or Required / Optional Wet-A Hire / Wet- (in addition to Schedules 1, 2, 3,4, & 5) Secondary bucket / Tank (preferred) or Bucket B Hire / Dry Hire (Note 7) (Note 11) (Note 1) (Note 2) (Note 5) (Note 9) (Note 10) (Note 3) (Note 4) (Note 4) (Note 6) (Note 8) AAS Firefighter & Cargo Transport RW21302 Primary Absolute ROTARY WING Type 3 Moorabbin Airport, Victoria Bucket (Optional) Required Wet-B 14 weeks Dec-Mar Schedules A & B Burning (Note 14) Firebombing (optional) AAS Firefighter & Cargo Transport RW21303 Primary Absolute ROTARY WING Type 3 Ovens helibase, Victoria (Note A) Bucket Required Wet-B 14 weeks Dec-Mar Schedules A & B Firebombing Burning (Note 14) AAS Firefighter & Cargo Transport RW21304 Primary Absolute ROTARY WING Type 3 Bairnsdale, Victoria Bucket Required Wet-B 14 weeks Dec-Mar Schedules A & B Firebombing Burning (Note 14) AAS RW21305 Primary Absolute ROTARY WING Type 3 Bendigo Airport, Victoria (Bucket) Required Wet-B 14 weeks Dec-Mar Schedules B Burning (preferred) (Note 14) Airborne Information Gathering (AIG) (Note 16) This Service requires a specific configuration to support regular 'airborne information gathering' operations (Refer to Section 2.1 of Part B RW21307 Primary Absolute AAS ROTARY WING Type 3 Moorabbin Airport, Victoria (Bucket) Required Wet-B 14 weeks Dec-Mar Schedules B & C in the Invitation to Tender document). -
2010-11 Victorian Floods Rainfall and Streamflow Assessment Project
Review by: 2010-11 Victorian Floods Rainfall and Streamflow Assessment Project December 2012 ISO 9001 QEC22878 SAI Global Department of Sustainability and Environment 2010-11 Victorian Floods – Rainfall and Streamflow Assessment DOCUMENT STATUS Version Doc type Reviewed by Approved by Date issued v01 Report Warwick Bishop 02/06/2012 v02 Report Michael Cawood Warwick Bishop 07/11/2012 FINAL Report Ben Tate Ben Tate 07/12/2012 PROJECT DETAILS 2010-11 Victorian Floods – Rainfall and Streamflow Project Name Assessment Client Department of Sustainability and Environment Client Project Manager Simone Wilkinson Water Technology Project Manager Ben Tate Report Authors Ben Tate Job Number 2106-01 Report Number R02 Document Name 2106R02_FINAL_2010-11_VIC_Floods.docx Cover Photo: Flooding near Kerang in January 2011 (source: www.weeklytimesnow.com.au). Copyright Water Technology Pty Ltd has produced this document in accordance with instructions from Department of Sustainability and Environment for their use only. The concepts and information contained in this document are the copyright of Water Technology Pty Ltd. Use or copying of this document in whole or in part without written permission of Water Technology Pty Ltd constitutes an infringement of copyright. Water Technology Pty Ltd does not warrant this document is definitive nor free from error and does not accept liability for any loss caused, or arising from, reliance upon the information provided herein. 15 Business Park Drive Notting Hill VIC 3168 Telephone (03) 9558 9366 Fax (03) 9558 9365 ACN No. 093 377 283 ABN No. 60 093 377 283 2106-01 / R02 FINAL - 07/12/2012 ii Department of Sustainability and Environment 2010-11 Victorian Floods – Rainfall and Streamflow Assessment GLOSSARY Annual Exceedance Refers to the probability or risk of a flood of a given size occurring or being exceeded in any given year.